

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spinal cord injury (SCI) refers to an insult to the spinal cord resulting in an either temporary or permanent change in the cord's normal motor, sensory or autonomic function. In recent years, acute SCI as a result of accidents from various domains have greatly increased among the middle age group, resulting in irreversible symptoms and various degrees of paralysis. The potential for pharmacological intervention to either preserve or recover neurological function exists because most traumatic injuries do not involve actual physical transection of the cord but rather as a result of a contusive, compressive or stretch injury24).
The pathophysiological mechanisms involved with SCI are both primary and secondary (neurogenic shock, vascular insults such as haemorrhage and ischemia-reperfusion, excitotoxicity, calcium mediated secondary injury and fluid-electrolyte disturbances in mitochondrion function)5), after which damaged neuronal axons have to undergo regeneration but this process is orchestrated by the presence of inhibitory substances in the extra cellular matrix (ECM)1). There are three theories trying to explain why the adult central nervous system (CNS) cannot regenerate; one theory proposes that Nogo, a molecule expressed by myelin, prevents axonal growth; the second theory emphasizes the role of glial scars; the third theory proposes that chondroitin sulfate proteoglycans (CSPGs) prevent axon growth32). Various studies have shown that therapies targeting second mechanism pathways and inhibitory substances in the ECM have beneficiary neuronal effects61131).
Experimental evidence suggests that MP, a synthetic glucocorticoid, reverts the effects of secondary injury when high dosage is administered soon after injury3). Its mechanism of action includes preventing lipid peroxidation, posttraumatic ischemia, destruction of neuronal and microvascular membranes, anti-inflammatory effects mediated through the suppression of NK-B binding924). However, glucocorticoid receptor expression is rapid but only transiently induced after SCI29), perhaps explaining the very limited therapeutic window of MP. Studies have also reported MP to have a variety of side effects616).
Tranilast (TR) N-(3,4-dimethoxycinnamoyl)-anthranilic acid is an anti-inflammatory drug with several mechanisms of action, approved in Japan and South Korea, since 1982 for the treatment of bronchial asthma as it was found to inhibit the antigen induced release of histamine from mast cells2128). TR has been used to inhibit keloid formation due to its antiproliferative and inhibition of collagen deposition182228). TR has a broad range of anti-inflammatory actions. Inhibition of vascular chymase, of platelet-derived growth factor (PDGF)-and transforming growth factor B1 (TGF-B1)-induced smooth muscle cell proliferation and migration are mechanisms that may explain at least in part, inhibition of vascular inflammation26). Its low toxicity and apparent effectiveness in suppressing cell proliferation, migration, and invasiveness as demonstrated in a number of in vitro and in vivo models of proliferation disorders emphasize its therapeutic potential. Studies by Hananda et al.8) showed that TR inhibits inflammation in the acute phase of SCI and reduces glial and fibrotic scars.
Studies have shown that targeting multiple pro inflammatory pathways may be more effective than targeting a single effector molecule41431). This paper for the first time uses methylprednisolone (MP) and TR to evaluate their synergic action and neuroprotective effects.
Go to : 
MATERIALS AND METHODS
Experimental animal
Animals
A total of 48 female wistar rats of specific pathogen free grade, aged 10–12 weeks, weighing 230–250 g were provided by the animal experimental center of Jilin University, Changchun, China (SCXK-2011-004). The animal research ethic committee of Jiamusi University approved the study. All experimental procedures were performed in accordance with the guidance and suggestions for care and use of laboratory animals, published by the Ministry of Science and Technology of People's Republic of China. Rats were maintained in ventilated, humidity (50–60%) well temperature controlled room (21+/-2℃) on 12 hours light/dark cycle. The animals were housed on sawdust and received food pellets and water ad libitum. Rats were acclimatized to their environment for 1 week before any experimental procedure. All behavioral experiments were performed during the light phase of cycle, i.e., between 8 : 00 am to 3 : 00 pm.
Surgical procedure of SCI
Rats were anaesthetized by injecting 10% chloral hydrate (350 mg/kg body weight) intraperitoneally. Dorsal aspect of thoracic region was shaved and scrubbed with povidone iodine solution. Under aseptic precautions and draping, a dorsal longitudinal mid-line incision was made over T9–11 vertebral region. Fascia and para vertebral muscles were gently dissected until the lamina and transverse processes were exposed. Haemostasis was strictly secured. Laminectomy at T10 was done, spinal cord exposed and compressed using an aneurysm clip (Yasargil aneurysm clips FE716K) as previously used by Jazayeri et al.10), and held in place vertically for 30 seconds. Para vertebral muscles and skin was sutured in layers. 1 mL of NS with crystalline penicillin (80000 units diluted in 5 mL NS) was injected subcutaneously following surgery in order to replace the body fluid loss during surgery and as prophylaxis for any post-operative infection. During recovery from anaesthesia, rats were placed on warm pad and covered with warm towel until re-establishment of thermoregulation and righting reflex. Following disappearance of tail wagging reflex, paralysis of both hind limbs the models were considered successful. Antibiotics (crystalline penicillin 80000 units diluted in 5 mL NS) were injected subcutaneously for 7 days to prevent any infection. Rats were nursed and housed in a cage with water and softened rodent chow provided Ad libitum. Rats demonstrated spontaneous emptying of bladder and bowel day 2 after surgery (Fig. 1, 2).
Experimental animals
Rats were randomly allocated into the following groups : Group 1 : Control Group : Rats were subjected to SCI with IP injection of the carrier solution (5 mL/kg of 5% dimethylsulfoxide in 0.9% normal saline) following SCI; Group 2 : TR group : Rats were administered TR [200 mg/(kg), IP] at 1 and 4 h after SCI and from day 2 received 200 mg/(kg/d); Group 3 : MP group, MP (0.75 mg/kg, IP) was administered at 1 and 4 h after SCI according to the methods of Messina et al.22). Group 4 : TR [200 mg/(kg)] and MP (0.75 mg/kg, IP) group, TR and MP were administered at 1 and 4 h after SCI and from day 2 received TR dosage of 200 mg/(kg/d). Rats from each group were used in the following experiments.
MPO activity
MPO activity, an indicator of polymorphonuclear leukocyte (PMN) accumulation, was determined in the spinal cord tissue as previously described20) at 24 hours after SCI. At the specific time following SCI, spinal cord tissues were obtained and weighed. The tissues were then prepared according to instructions from the MPO kit (Nanjing Jiancheng Bioengineering Institute). The rate of change in absorbance was measured spectrophotometrically at 460 nm. MPO activity was defined as the quantity of enzyme required to degrade 1 µmol of peroxide min at 37℃ and was expressed as units of u/g of wet tissue. MPO activity was obtained by the following calculations : MPO activity=(measured OD value-Control OD value)/(11.3×mass of sample tissue used kg).
Determination of spinal cord water content
Spinal cord edema was evaluated by determining the water content of the spinal cord. For the time course study, the injured spinal cords for all groups were dried for 24 h at 110℃ for determination of the dry weight (Havppvel method). Water content in spinal cord tissue was obtained by the following calculations : spinal cord water content (%)=(wet weight-dry weight)/wet weight×100%.
Behavioural assessment
Rats were tested for locomotor function prior to SCI then at day 1, 3, 7, 10, and 14 subsequent to SCI. The rats were allowed to move for 4 mins in an open field and hind limb functions were assessed by 2 observers blinded to the rat experimental procedures and scored based on the Basso, Beattie and Breshnahan (BBB) locomotor rating scale developed by Basso et al.2). The BBB scale is a 21-point system based on operationally defined behavioural features that follow the process of recovery from complete paralysis to normal locomotion where a score of 0 indicates complete hind limb paralysis and a score of 21 indicates complete normal locomotion function.
Tissue processing, staining, and histopathology
On day 7 and 14 subsequent to SCI, three rats from each of the groups were sacrificed for immunohistological staining. Sections of the spinal cord encompassing the injury site were dissected and fixed by immersion in 4% formaldehyde for 24 h, and cryoprotection in 10% sucrose at 4 degrees Celsius until they sank, the spinal cords were then embedded in optimum cutting temperature (OCT) compound, frozen and cut into 3-micrometer cryostat sections in the horizontal plane. The tissue sections were stained with a Haematoxylin and Eosin (H&E) Staining Kit to assess the morphology of the injury site. Eight to ten sections were stained for GFAP to identify GFAP positive cells and distribution of GFAP. Immunohistochemical staining was performed using Rabbit GFAP antibody Kit (Boster, Wuhan) in accordance with the manufacturer's instructions. Images were captured using a FV 300 confocal microscope (Olympus, Tokyo, Japan) for analysis.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 20.0 for windows (SPSS Inc., Chicago, IL, USA). One way analysis of variance followed by Bonferroni's post hoc test was utilized to determine significant differences among multiple groups. Independent sample t-test was used to compare significance mean differences between two groups. Image Pro-Plus 6.0 was used for histopathologic analysis of images captured. All values were expressed as the mean±standard deviation, p<0.05 was considered to indicate a statistically significant value.
Go to :
RESULTS
Evaluation of the combination therapy on spinal cord water content
According to the present study, the water content of the spinal cords was measured at 24 h after SCI. There was significant difference between the groups. Compared to the control group the individual therapy MP (75/kg) showed significant reduction in spinal cord water content p<0.05. TR did not show significant change in spinal cord water content p>0.05. The combined therapy MP (75/kg) and TR (200 mg/kg) had better results and significantly ameliorated the increase in spinal water content after SCI and showed reduction in spinal cord water; p<0.05 vs. the control, p<0.05 vs. MP and TR (Fig. 3).
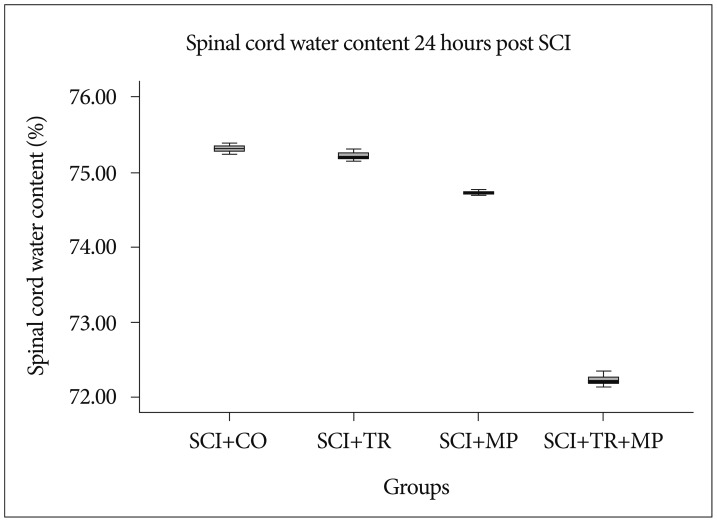 | Fig. 3Percentage changes in the water content of spinal cord tissues using different therapies 24 h after SCI. The combination therapy significantly ameliorated the spinal cord water content compared to the individual therapies. p<0.05 vs. the control group. SCI : spinal cord injury, MP : methylprednisolone, TR : tranilast.
|
Evaluating the combination therapy; on neutrophil infiltration
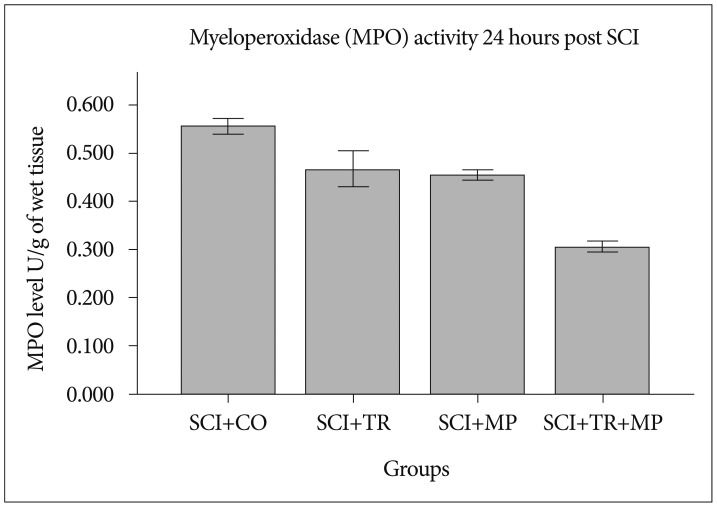
MPO activity was measured in the spinal cord tissue samples for each group 24 h after SCI so as to investigate the degree of neutrophil infiltration. The independent therapies MP and TR exhibited significant reduction in the MPO activity compared to the control p<0.05. The combined therapy using MP (75/kg) and TR (200/kg) significantly reduced neutrophil infiltration better than the individual therapies; p<0.05 vs. the control, p<0.05 vs. MP and TR (Fig. 4).
Behavioural analysis
BBB locomotor rating scale was used to analyze the recovery of locomotor function after SCI. All rats were assessed for locomotor function pre-injury, and on days 1, 3, 5, 7, 10, and 14 post injury. All rats had normal limb function and obtained a score of 21 before SCI. Following SCI the rats in all the groups had a BBB score of 0 indicating total injury. Individual therapies MP and TR indicated significant improvement in hind limb function at day 7, 10, and 14 p<0.05 vs. the control. The combined therapy with MP and TR indicated consistently higher scores and were statistically significant from day 3 to day 14 after SCI p<0.05 vs. control and p<0.05 vs. individual therapies MP and TR (Fig. 5).
 | Fig. 5Changes in locomotor deficits after a spinal cord ingury. Behavioral scores were measured by the BBB methods. The BBB socres decrease afyer an injury (0. Indicating complete injury) and slowly and gradually increase. The combined therapy with MP and TR promoted a signficant behavioral recovery following a SCI p<0.05 vs. the individual therapies of MP and TR. SCI : spinal cord injury, BBB : Basso, Beattie, and Bresnahan, MP : methylprednisolone, TR : tranilast.
|
Histopathology findings
H&E staining
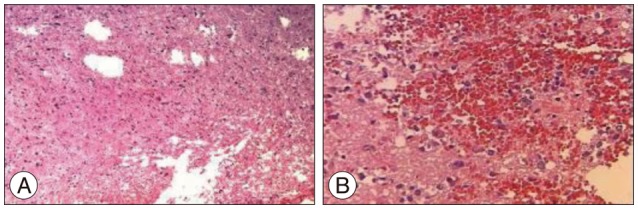
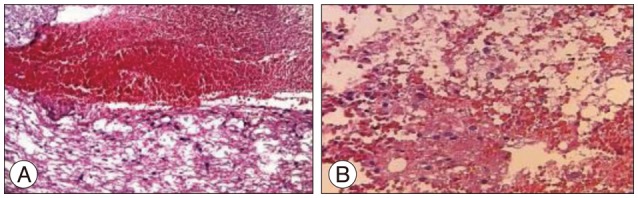
H&E staining was done on spinal cord tissues at 14 days after SCI to see the morphologic changes at the injury site and the extend of neural damage using aneurysm clip to create SCI model. At the injury site the structure of the spinal cord was destroyed and formation of cystic spaces was observed. The nerve fibres were disorganized with liquefaction of spinal tissue. Extradural haemorrhage was observed at the injury site with neutrophil infiltration and necrotic tissue. Neuronal apoptosis and the number of gliocytes increased (Fig. 6, 7).
GFAP : immunohistochemistry results
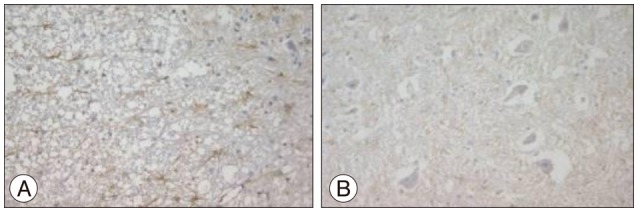
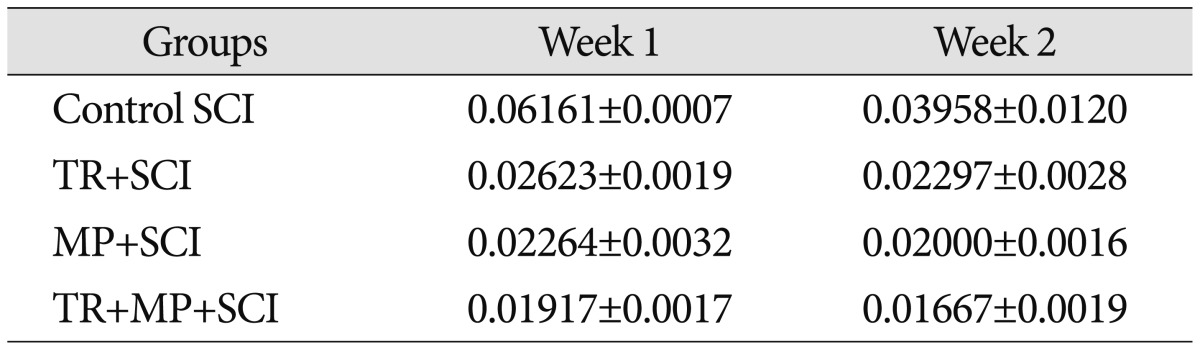
The amount of gfap expression was recorded based on the average optical density as shown in Table 1. The cytoplasm of the GFAP positive cells appeared brown and radial like projections were seen protruding from the cytoplasm. At 7 days after SCI the control group showed deep staining to positive cells showing hypertrophy and neurite extension. GFAP positive cells were highly concentrated at the site of injury alongside extradural haemorrhage. No glial scar was seen at this stage. The groups with the individual therapies of MP and TR showed a less dense staining compared to the control group and the GFAP expression was significantly less, p<0.05 vs. the control group. There was no significant difference between the GFAP expression of the individual therapies and the combined therapy of MP and TR p>0.05. At 14 days there was slight drop in the GFAP expression in all groups but the drop was not statistically significant p>0.05. The individual therapies and the combined therapy showed a less dense staining and the positive cells were distributed at the injury site surrounding the neural cells, cavities and astrocyte hypertrophy was also observed. The difference in the mean GFAP expression between the groups was not statistically significant p>0.05 (Table 1, Fig. 8, 9, 10, 11).
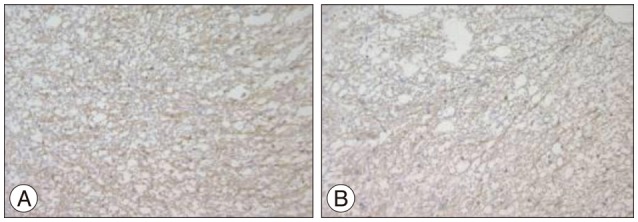
 | Fig. 8Control Group. At 7 and 14 days after SCI glial fibrillary acidic protein (GFAP) expression was enhanced at he injury site, extradural haemorrhage was observed at 7 days after SCI (A). Cells were deeply stained and there was astrocyte hypertrophy (B). magnification, ×200. A : 7days post SCI. B : 14 days post SCI.
|
 | Fig. 9TR group. At 7 and 14 days post SCI the staining for GFAP was less dense and were concentrated at the injury site around cavitations formed. Magnification ×200. A : 7 days post SCI. B : 14 days post SCI.
|
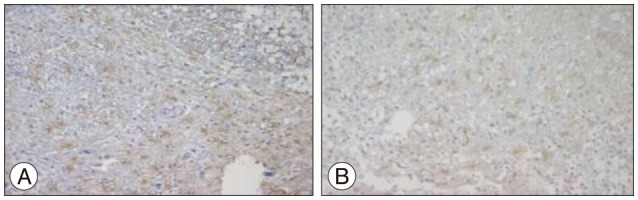 | Fig. 10MP group. At 7 and 14 days after SCI the injury site showed less dense GFAP staining and the positive cells were around cavities (A) magnification ×200 (B). A : 7 days post SCI. B : 14 days post SCI.
|
Go to :
DISCUSSION
Results from this study provide evidence that a combination therapy of MP with TR significantly reduced posttraumatic spinal cord edema, neutrophil infiltration and improved functional recovery better than single individual therapies. The combination therapy also significantly reduced the amount of GFAP expression at the injury site.
Both therapies have been shown to have neuroprotective effects after SCI. Studies by Hananda et al.8) showed that TR inhibits inflammation in the acute phase of SCI and reduces glial and fibrotic scars. The present study also showed that TR has neuroprotective functions after SCI. MP has been extensively studied and shown to have neuroprotective function13). MP is used in high doses after SCI. This is the first study to show enhanced neuroprotective outcome after SCI using MP and TR.
Till date traumatic SCIs are managed with many challenges and with limited options. Following trauma immediate surgical treatment is carried out to stabilize the injured area and to prevent further damage to the spinal cord. SCI leads to lifelong disability and various degrees of neurological deficit depending on the nature and magnitude of the trauma. No appropriate treatment exists for treating victims or minimizing their suffering. The secondary injury mechanism following SCI is characterized by neurogenic shock, vascular insults such as haemorrhage and ischemia-reperfusion, excitotoxicity, calcium mediated secondary injury and fluid-electrolyte disturbances in mitochondrion function and other miscellaneous processes5). These mechanisms present many pathways by which injury is inflicted on the spinal cord and are thus potential targets for drug therapies to reduce the degree of injury to the spinal cord in the acute phase, so it is logical to think that using therapies targeting several pathways will lead to better results. Studies have shown that therapies targeting multiple proinflammatory pathways may be more effective than those targeting a single effector molecule32). Li et al.14) showed that combining MP and amino guanidine (AG) significantly reduced the levels of neutrophil infiltration (MPO activity), cytokine expression (TNF-α and IL-1β) and apoptosis (Bax and Bcl-2 expression) confirming that strategies targeting multiple proinflammatory pathways may be more effective than those using a single drug molecule. This was also confirmed in the present study using MP and TR.
Following SCI astrocytes become hypertrophic, and proliferate in the process of reactive gliosis. This is followed by the up regulation of GFAP and other inhibitory ECM components such as CSPG and Vim. This leads to the formation of a glial scar that is unfavorable toward axonal regeneration and neurological recovery23). Studies on glial scar show that manipulating the extrinsic factors that block growth in the immediate environment of the glial scar may be able to induce long distance and functional regeneration after CNS injury25).
In the present study the combination therapy resulted in reduced expression of GFAP one week post SCI but there was no significant difference compared to the individual therapies. Studies suggest that MP down regulation of astrocyte reactivation and inhibition of CSPG expression is through glucocorticoid receptor inhibition15). TR mechanism of action is unclear but can be attributed to inhibition of vascular chymase, platelet-derived growth factor- and transforming growth factor B1 which studies have shown to be initiating factors of gliosis1219) as well as suppression of collagen synthesis27).
GFAP expression showed peak values in the first week post SCI30) so we propose that higher doses of TR in the therapeutic combination should be administered in the first week post SCI so as to further enhance down regulation of GFAP. So further studies can be performed using different doses of TR in the combination during the first week, as well as a detailed investigation on the molecular mechanism of the combination therapy.
Go to :
 XML Download
XML Download