

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
To stand upright, the human body must maintain a balance between spinal curvature and pelvic morphology1). As the spine and the pelvis are connected in a biomechanical system420), the morphology of pelvic curve will change to compensate for changes in spinal curvature.
When lumbar spondylolisthesis occurs, the sagittal shape of the pelvis will be inevitably affected. Recently, a few studies have reported the pelvic parameters in lumbar spondylolisthesis11151619). However, the pelvic parameters only record local changes in pelvic morphology and do not take into account how the spine compensates for pelvic changes. Jackson et al.56) notes that the pelvis and spine should be considered a whole unit when considering biomechanics, and for this, he proposed the pelvic radius (PR) technique, which reportedly has similar reliability to pelvic parameters7). Sergides notes that the PR technique can help to prevent poor visualization of C7, which is typical when using sagittal vertical axis from C7 plumb line (SVA) measurements18). To the best of our knowledge, there are few studies assessing sagittal alignment in spondylolisthesis using the PR technique6). The aim of this study was to investigate the sagittal pelvic morphology in lumbar isthmic spondylolisthesis using the PR technique, compared to controls.
MATERIALS AND METHODS
Patient population
We retrospectively reviewed 74 Chinese patients who had a confirmed diagnosis of lumbar isthmic spondylolisthesis on X-ray and a three-dimensional CT from January 2011 to April 2014. The local Institutional Review Board approved the study. The average age of the subjects was 49.2±9.5 years (range : 30–66 years). There were 17 males and 57 females, which included 30 grade I slippages and 44 grade II slippages according to the system of Meyerding. They all had low-grade spondylolisthesis; 34 subjects had spondylolisthesis at L4 and 40 subjects at L5. The exclusion criteria were as follows : 1) previous spinal fracture or surgery, 2) spinal infection or tumor, 3) hip disease, and 4) lower limb deformities.
Control group
Healthy volunteers consisted of 23 females and 24 males with an average age of 23.3 years (range : 21–27 years). They had no previous history of spinal, pelvic, or hip disorders. All subjects were college students. They were informed of the risks of participating in this study and signed an informed consent form.
Radiographic parameters
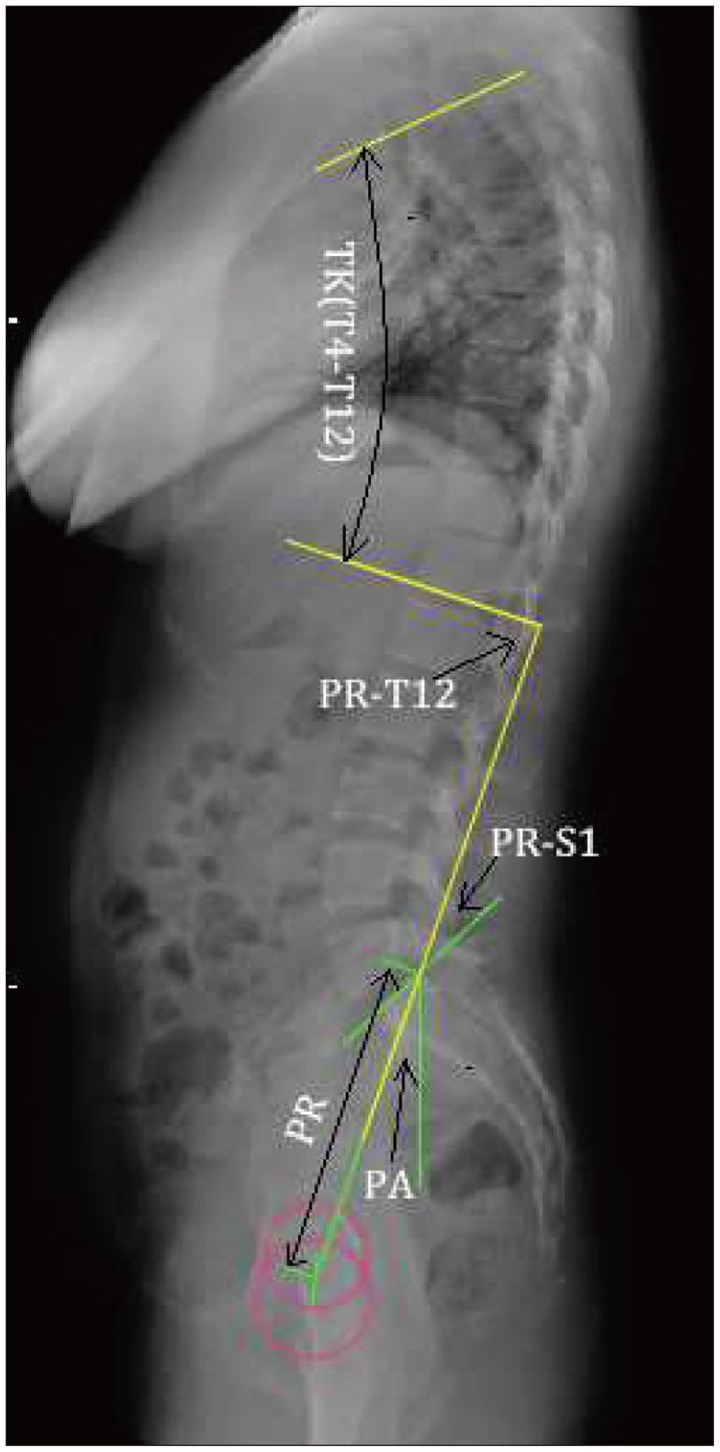
For each subject, the lateral view of spinal radiograph, including the base of the skull and the upper section of the femur, was obtained. Subjects were asked to stand upright with their knees extended, with their elbows bent to accommodate shoulder flexion to 30°13). The parameters using the PR technique included (Fig. 1) : 1) Pelvic radius (PR), the distance from the hip axis to the posterior-superior corner of the S1 endplate; the hip axis was located in the middle between the two femoral bead mid-points. 2) The pelvic angle (PA), the angle between the PR line and the plumb line. 3) Pelvic morphology (PR-S1), the angle between the PR line and the S1 endplate line. 4) Total lumbopelvic lordosis (PR-T12) and thoracic kyphosis (TK), both T12-PR and T4–12, measured using the Cobb technique.
Statistical analysis
Statistical analysis was performed using SPSS software (SPSS for Windows version 13.0, SPSS Inc., Chicago, IL, USA). We compared the demographic factors and spinal parameters of the patients and the healthy volunteers using an independent-samples t-test, with subgroups for gender, L4 and L5 spondylolisthesis, and I° and II° spondylolisthesis. The statistical significance level was set at p<0.05.
RESULTS
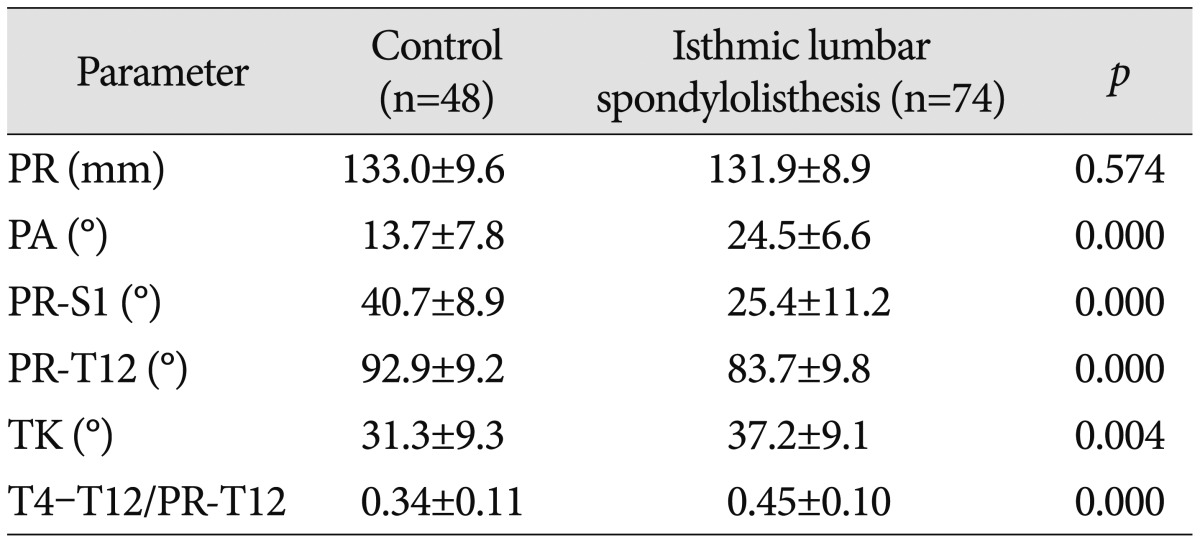
Compared to the control group, the TK (37.2±9.1°) and the PA (24.5±6.6°) of the total patients were significantly greater (p<0.05), and the PR-S1 (25.4±11.2°) and PR-T12 (83.7±9.8°) were significantly lower (p<0.05), while there was no significant difference in the PR (Table 1). However, the TK/PR-T12 ratio was consistently between 0.15 and 0.75 in the patient group.
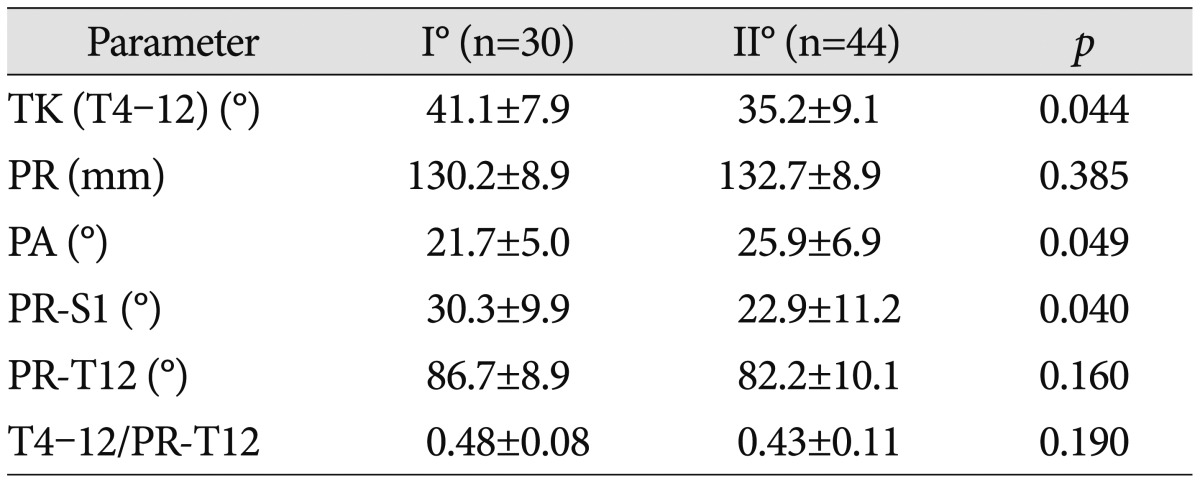
The patient group was divided into those with grade I and grade II spondylolisthesis. The PA was significantly greater for grade I patients (21.7±5.0°) and grade II patients (25.9±6.9°) compared with the control group, respectively (13.7±7.8°) (p<0.05), and the PR-S1 and PR-T12 were significantly lower. The TK was significantly greater for grade I patients (41.1±7.9°) than that of the control group (31.3±9.3°) (p=0.001) (Table 2).
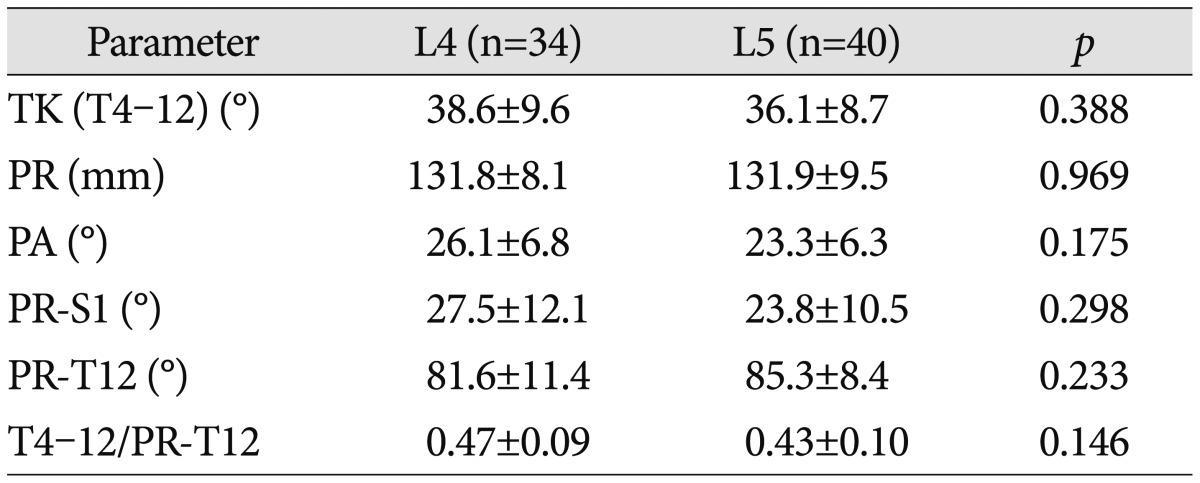
The patient group was divided into L4 and L5 spondylolisthesis subgroups. We compared the TK (T4–12), PR, PA, PR-S1, PR-T12, and the TK/PR-T12 ratio between L4 and L5 subgroups, and found no statistical difference between the two groups (p>0.05), as shown in Table 3.
DISCUSSION
The physiological curvature of the spine includes cervical lordosis, thoracic kyphosis, lumbar lordosis, and sacral kyphosis. Normal physiological curvature is an important factor to ensure that people can walk upright and maintain balance, as the spine and the pelvis area work together as a unit to enable normal ambulation. However, spondylolisthesis inevitably leads to changes in the sagittal pelvic morphology.
Studying sagittal balance helps us to understand the changes in the lumbopelvic biomechanics in lumbar spondylolisthesis and provide theories to guide clinical treatment.
Most previous studies have focused on pelvic parameters1116). Since the spine and pelvis are a whole, when the sagittal alignment of the lumbar spine changes, the upper spine will make compensatory changes to regain balance9). Therefore, the standalone use of pelvic parameters to evaluate the sagittal balance of lumbar spondylolisthesis may overlook the compensatory effect of the thoracic spine. Jackson et al.6) described a PR technique to evaluate sagittal spinopelvic balance, which includes PR, PA, PR-T12, and PR-S1. They have reported that the reliability of PR-T12, PI, and PR-S1 is similar7). In addition to PR-S1, it is not necessary to identify the whole S1 endplate when use the PR technique to measure. Using PI and SVA methods, clear visualization of the S1 endplate and the C7 vertebra is essential. But according to reports, the C7 vertebrae can be clearly identified on the whole spine lateral radiographs only in about half of the cases18). Our study also found that the C7 vertebrae could not be fully visualized in most patients. Using the PR techniques, we can obtain more accurate data than the PI and SVA methods. Jackson et al.7) indicated that the PR technique was more reliable than plumbline measurement.
Meanwhile, Jackson et al.57) proposed the concept of "congruent" spinopelvic alignment. "Congruent" alignment should meet the following three conditions : 1) PR-T12 is between 70° and 100°, 2) the PA is between 3° and 33°, and 3) the T4–12/PR-T12 ratio is between 0.15 and 0.75.
Geometrically, PR-T12 is the sum of PR-S1 and T12–S1. Its value is in a relatively narrow range in healthy individuals, about 90°±10°18). Thus, the total lumbopelvic lordosis decreases when the PR-S1 increases, and vice versa.
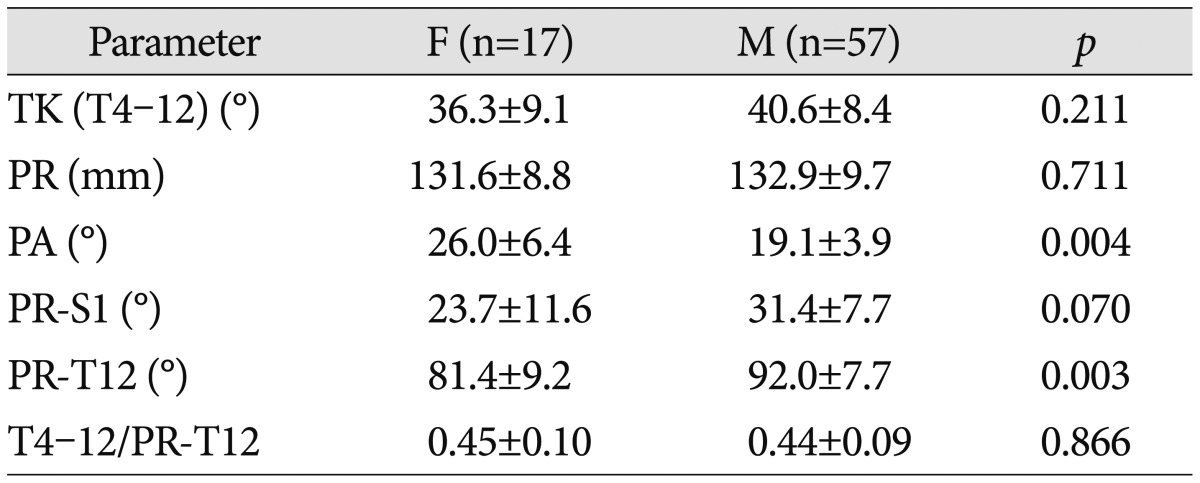
We found that the PA of spondylolisthesis was significantly increased, while the PR-S1 and PR-T12 were significantly reduced, and, as the degree of spondylolisthesis increased, the PA increased, but the PR-S1 decreased. Therefore, with an increasing degree of spondylolisthesis, the pelvis rotates around the hip axis, leading to verticalization of the sacrum17). Meanwhile, we found that the PA of females is greater than that of males, indicating that the female pelvis tilts backward seriously. Thus, the shear force of the female lumbosacral part is greater16) and the probability of the occurrence of spondylolisthesis is also greater.
Park et al.15) observed that lumbar spondylolisthesis can affect the sagittal balance of the lumbar spine. Sergides et al.18) pointed out that although PR-T12 can quickly evaluate sagittal lumbar balance, the compensatory effect of the upper spine cannot be ignored.
We found that the PA, PR-S1, and PR-T12 of low-grade spondylolisthesis differed from the normal ranges significantly, demonstrating that the local morphology of the lumbar spine and pelvis have changed. However, according to the "congruent" spinopelvic alignment criteria7), for low-grade spondylolisthesis patients, the sagittal trunk is still in a state of balance. This demonstrates that when the local morphology of the lumbar spine and pelvis changes, the remainder of the spine will compensate in terms of position to maintain overall balance, such as intervertebral hyperextension and pelvic retroversion10). Therefore, the PR technique enables effective evaluation of spinal sagittal balance and minimizes the measurement error caused by unclear views of C7.
Because the L4/L5 vertebrae are the apex of lumbar lordosis2), the lower lumbar spine is a predominant region for biomechanical transmission, and thus lumbar spondylolisthesis often occurs in this region. Oh et al.14) observed that spondylolisthesis of different segments of the lower lumbar spine incurs similar changes in pelvic morphology. We observed similar results in our study : there was no significant difference in the PR and related parameters between L4 and L5 spondylolisthesis. For severe spondylolisthesis (slip percentage >50%), the difference in the pelvic morphological changes of different segments of spondylolisthesis requires further investigation.
Mac-Thiong et al.12) indicated that sagittal imbalance is more likely to cause pain and dysfunction. Posterior pedicle screw fixation is the major surgical treatment for spondylolisthesis. By restoring sagittal balance, it can reduce the incidence of flat back syndrome and pathology in the adjacent segments8), thus achieving a better prognosis320). Satisfactory clinical outcomes are dependent on preoperative measurements, which can help us to adjust the angle of pedicle screws during operations and restore sagittal spinopelvic balance.
Our study had several limitations, such as a small number of cases; in addition, we did not include severe spondylolisthesis and multiple-level spondylolisthesis, which may affect the results.
CONCLUSION
Pelvic morphology is abnormal in spondylolisthesis, but spinopelvic balance is not affected. The gender and grade of slippage had an effect on the sagittal configuration of the pelvis, but there are no differences in terms of the impacts different segments of vertebral slip had on pelvic morphology.

 XML Download
XML Download