

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Choroidal fissure cysts are benign intracranial cysts occurring at the level of choroidal fissure. They are usually asymptomatic and discovered incidentally. They are usually small, quite round and noncompressive3). Magnetic resonance imaging (MRI) signal characteristics are similar to cerebrospinalfluid (CSF). Contrast enhancement, surrounding edema and gliosis are absent2). The differential diagnosis of choroidal fissure cysts include parasitic, epidermoid and arachnoid cysts. They are almost always benign with interval follow-up showing no imaging changes. Progression of such cysts are very rare. In this report, an extremely unusual case of growing and hemorrhagic choroidal fissure cyst is presented.
Go to : 
CASE REPORT
A 22-year-old female presented with one month history of headache. Physical and neurological examination was totally normal. Cranial MRI showed a left-sided choroidal fissure cyst measuring 4×5 mm (Fig. 1). The cyst was hemorrhagic and showed fluid-fluid level on T2-weighted and susceptibility weighted images. There was neither contrast enhancement nor surrounding edema or mass effect. MR angiography showed no vascular abnormality. During the next 14 months she was followed conservatively. During this period she occasionally suffered headache, but her neurological examination remained normal. Follow-up MRI showed that the size of the cyst had increased gradually, eventually becoming 10×8 mm, while other imaging features had not changed (Fig. 2). Six months after the latest MRI scan, the patient was admitted to our emergency department with severe headache. Her neurological examination was still normal. MRI and computed tomography (CT) showed an intracystic hematoma, 25×25 mm in size, with surrounding edema and slight mass effect (Fig. 3). The patient was operated via left frontotemporal craniotomy. Hematoma was reached through left middle temporal sulcal way. Hematoma and thin cyst wall were removed. There was no vascular malformation. The cyst wall was not attached to the choroid plexus. After the operation, she was symptom free without headache or neurological deficits. Postoperative pathological examination diagnosed as neuroepithelial cyst (Fig. 4).
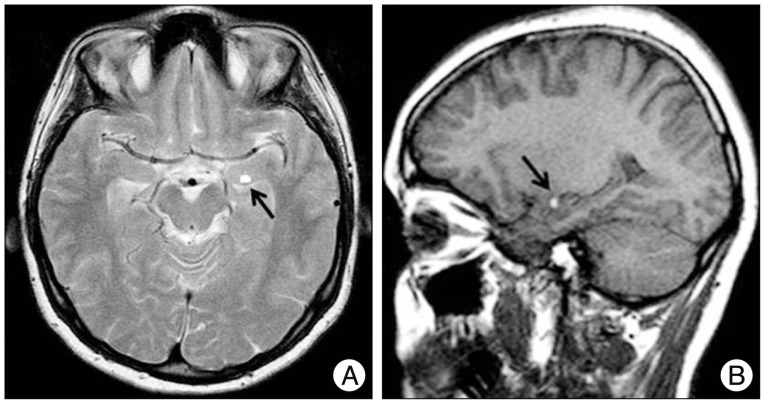 | Fig. 1A small hemorrhagic choroidal fissure cyst (arrows) is noted on T2 weighted axial (A), sagittal (B) images MRI scan.
|
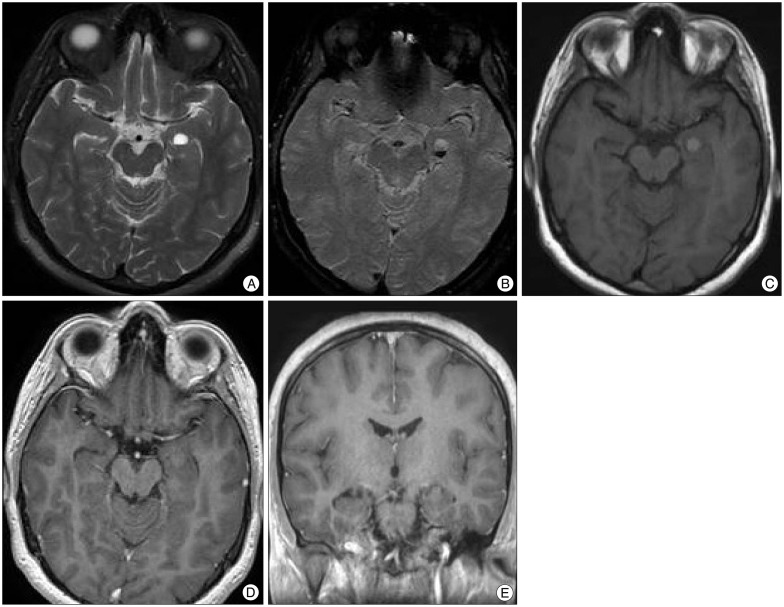 | Fig. 2MRI of growing hemorrhagic choroidal fissure cyst. T2 weighted (A), susceptibility weighted MRI axial (B) scans show hemorrhagic cyst with fluid-fluid levels. T1 weighted axial (C), T1 contrast axial (D), andT1 contrast coronal (E) images show no contrast enhancement.
|
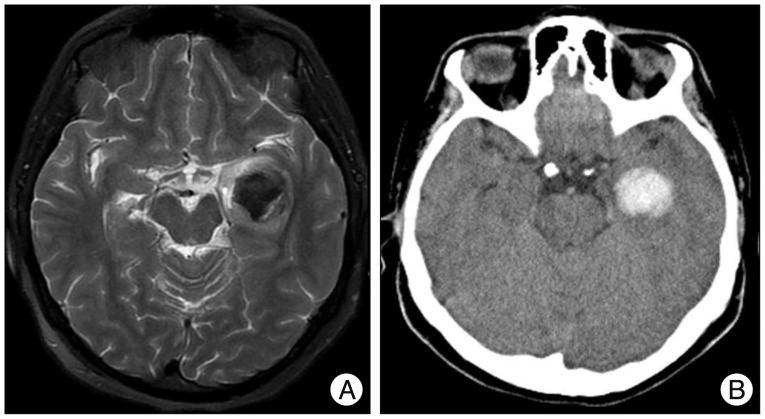 | Fig. 3T2 weighted axial image (A) and CT scan (B) show large intracystic hemorrhage with surrounding edema.
|
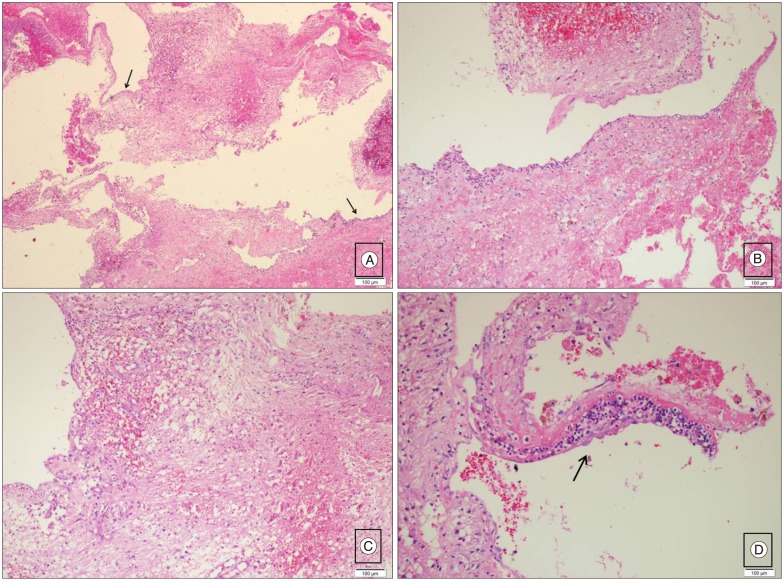 | Fig. 4A : Thin cyst wall (arrows) was directly abuted the gliotic parenchyma (Haematoxylin & Eosin ×40). B : The cyst wall have no real epithelium. There is a minimal inflammatory cell infiltration on cyst wall (Haematoxylin & Eosin ×100). (C) Reactive gliozis around the cyst wall (Haematoxylin & Eosin ×100). D : The cyst wall was covered focally with real epithelium. The cyst have a low cuboidal lining (arrows) (Haematoxylin & Eosin ×200) (Permission from Turkan Rezanko).
|
Go to :
DISCUSSION
CSF containing cysts at the level of choroidal fissure are rare embryological lesions3). The choroidal fissure is the narrow cleft between the fornix and thalamus along which the choroid plexus is attached. The edges of the thalamus and fornix bordering this choroidal fissure have small ridges, called the teniae, along which the tela choroidea, the membrane in which the choroid plexus arises, is attached. The choroidal fissure is formed at approximately 8 weeks of embryonic development when the vascular piamater that forms the epithelial roof of the third ventricle invaginates into the medial wall of the cerebral hemisphere. No nervous tissue develops between the ependyma and piamater along this invagination that forms the choroidal fissure, thus creating the thinnest site in the wall of the lateral ventricle. The choroidal arteries, which supply the choroid plexus enter the ventricles through the choroidal fissure. The veins coursing in the walls of the ventricles exit the ventricles bypassing through the margin of the choroidal fissure in the subependymal location to reach the internal cerebral, basal, or great veins4). Developmental errors may occur at the time of formation of primitive choroid plexus anywhere along the choroid fissure, thus forming a cyst5). However, the etiology is stil controversial. The cysts may be of the neuroepithelial or arachnoid type5). Lesions are spherical to ovoid, measure up to several centimeters in size2). Sherman et al.5) Reviewed the MRI studies of choroidal fissure cysts and reported 26 cases, mostly adults, with neurological symptoms such as complex migraine, seizure, gait disturbance, tremor, vertigo, hearing loss, paresthesia, hemiparesis and visual scotomata. Clinical follow-up without development of symptoms referable to the cyst average 17.8 months. None of these patients was operated. They reported that the cysts could not explain the patients' signs or symptoms5). de Jong et al.3) reported 6 patients with a CSF-containing cyst at the level of choroidal fissure with neurological symptoms such as headache, narcolepsy and hyperactivity disorder. All patients were followed with MRI which demonstrated total absence of progression of the lesions. Conservative treatment was used3). There are limited reports about choroidal fissure cyst being treated via surgery. These usually require only follow-up. Tubbs et al.6) reported progression of choroidal fissure cysts which were treated with fenestration and possible ventriculo-peritoneal shunting. Baka and Sanders1) reported a case of spontaneous hemorrhagic choroid plexus cyst in lateral ventricle. It was thought that the cyst was incidental and was not related to the patient's symptoms. Therefore, no treatment or further investigation was suggested1). Differentiation between neuroepithelial and arachnoid CSF-containing cysts at the level of choroidal fissure can only be made by histopathological examination3). Differentiation of benign choroidal fissure cysts from other cysts (cystic neoplasms or infectious cysts) is important because of the need for active treatment in the latter group. Cystic neoplasms or infectious cysts were excluded in our case because of the absence of a solid component, contrast enhancement, perilesional edema or mass effect. Dermoid cyst could also be considered in the differential diagnosis; however, in our case T1 hyperintensity represented hemorrhage and did not correspond to lipid content, since on fat-saturated T2 weighted images, nondependant part of the lesion was bright, not following the signal of fat. The presence of hemorrhage could be explained by the close relationship of the lesion with the choroid plexus of the temporal horn or the presence of heterotopic choroid plexus within the cyst. In cases of choroidal fissure cysts, at least 2 years of clinical and radiological follow-up is recommended, while surgery is indicated only in accompanying life-threatening conditions such as massive hemorrhage.
Go to :
 XML Download
XML Download