

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Thoracic ossification of posterior longitudinal ligament (T-OPLL) often requires surgical treatment in cases of symptomatic progressive myelopathy. There are various kinds of surgical options for thoracic OPLL. Direct decompression could be achieved with anterior, posterior or a combined approach. Indirect decompression could be achieved with laminectomy, laminoplasty or posterior instrumented correction of thoracic kyphosis5811121314151826272830). Although direct removal of T-OPLL is ideal for neural element decompression, complications associated with the anterior approach, e.g., neurologic deficit and dural tear/cerebrospinal fluid (CSF) leakage, leads us to explore other potential surgical options513141718). Because laminectomy had a poor outcome due to progression of thoracic kyphosis and persistent ventral compression, instrumented fusion with or without direct removal of T-OPLL mass with posterior approach was introduced with comparable recovery rate to anterior approach59111213141819). Although indirect decompression can be achieved with this technique13), circumferential decompression is sometimes a more suitable surgical option8111227). However, in these instances, a complication rate of approximately 30% has been encountered, most notably in beak-type T-OLL (growth of OPLL mass across a disc space at a single segment)131528). The OPLL mass is traditionally removed with a high-speed drill581011122130). Slipping off the cutting surface and entrapping important soft tissues, such as neural structure, may leads to serious complication. The ultrasonic osteotome is a recent introduction to the clinical field27202324). Such devices utilize back and forth micro-motion rather than rotatory-motion to allow precise removal of bone with minimal impact to the adjacent soft tissues27202324). Energy from the cutting edges of these devises is preferentially transmitted to hard structures (bone)27202324). Adjacent soft tissues (ligamentum flavum, posterior longitudinal ligament, dura) are spared as these structures can bend, vibrate and deform to vibratory micromotion27202324). The advantage of a tissue selective cutting device may be utilized in the removal of compressive T-OPLL. We have applied the ultrasonic osteotome for posterior circumferential decompression of T-OPLL in a series of patients and have described the surgical technique and patient outcomes.
MATERIALS AND METHODS
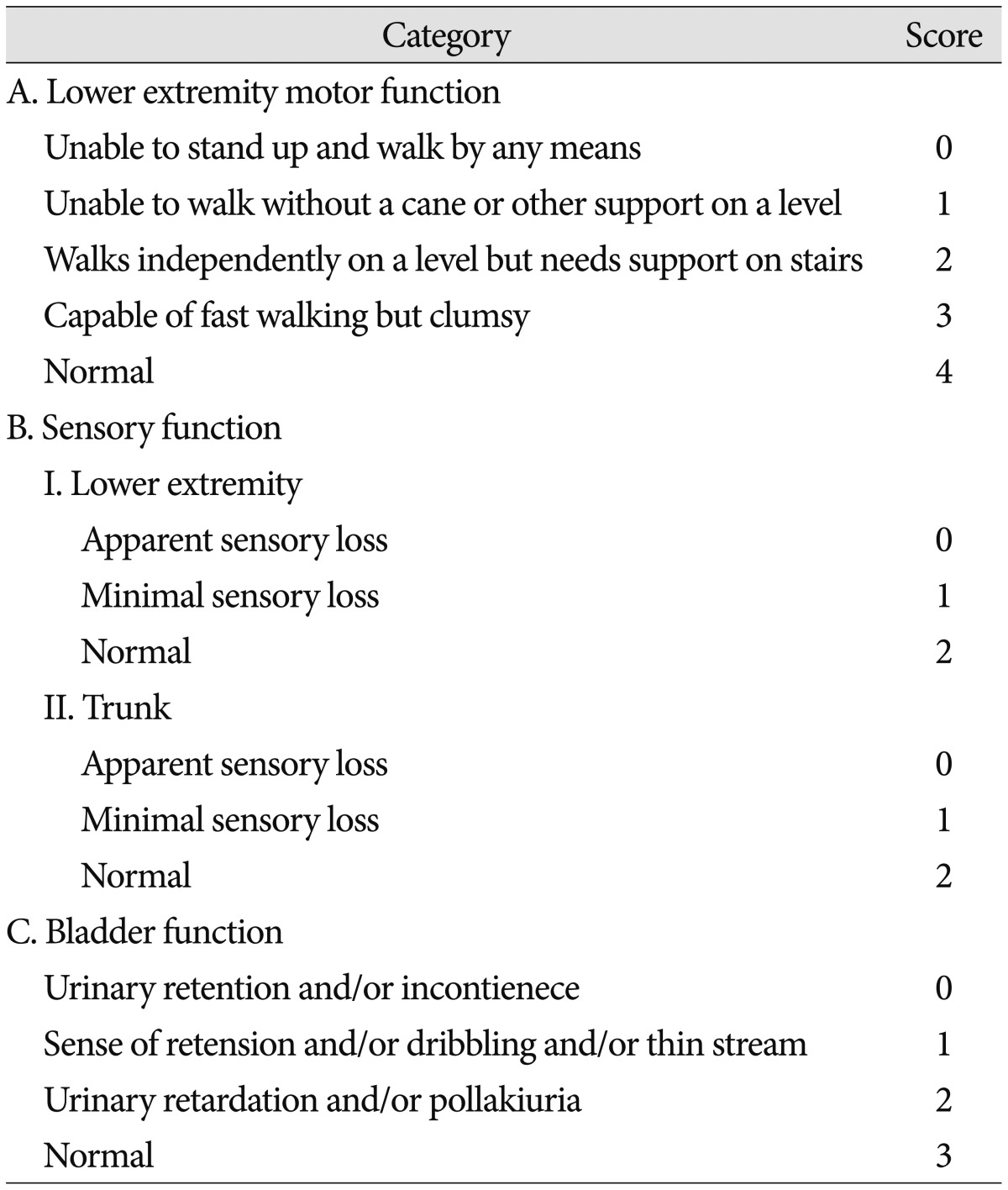
Starting October 2012, we have applied the ultrasonic osteotome for four consecutive patients with beak-type OPLL (Table 1). The preoperative chief complaint was gait disturbance in all patients. Two patients underwent cervical laminoplasty 2 and 3 years previously secondary to cervical OPLL (Case 1 and 3). Their main problem was paraparesis and symptom was partially improved in Case 1 and normalized in Case 3 after cervical laminoplasty. However, gait disturbance was aggravated 12 months and 30 months after initial surgery, respectively. In the other patients, there was no history of spine surgery. Neurological status was assessed with the Japanese Orthopedic Association (JOA) scoring system for thoracic myelopathy (Table 2)811121314). Magnetic resonance (MR) imaging and/or computed tomography (CT) scan were obtained both pre- and post-operatively and patients were scheduled to be followed-up at postoperative month 1, 3, 6, 12 and yearly thereafter.
Surgical techniques
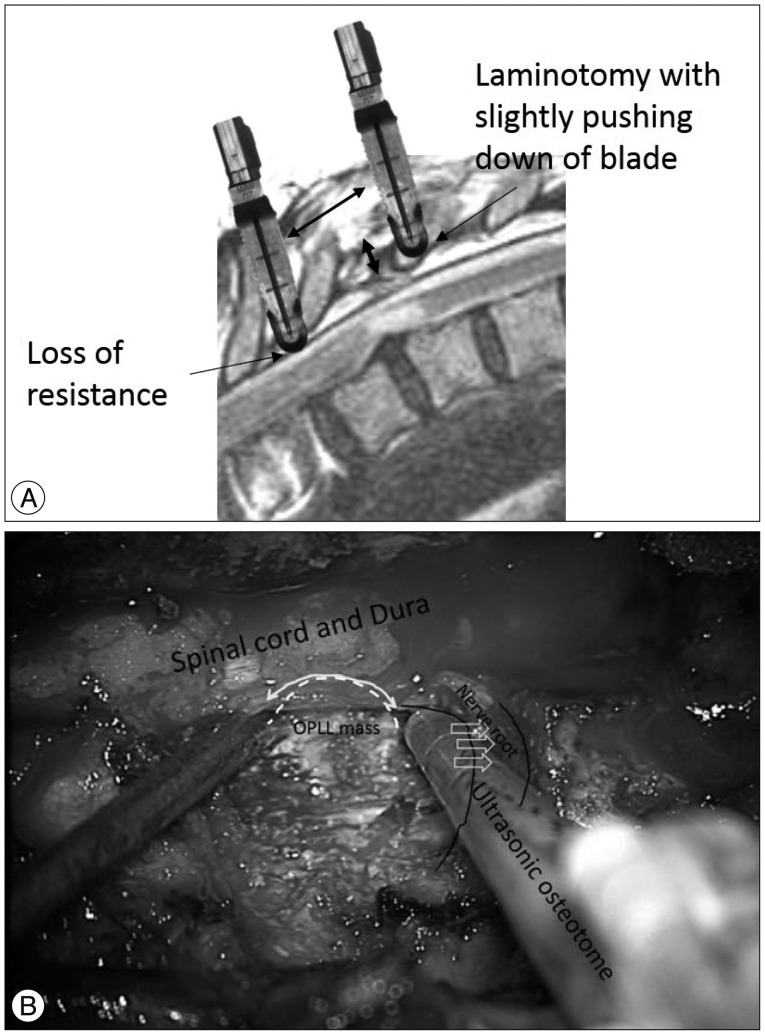
Posterior circumferential decompression and instrumented fusion was performed in all patients. Intraoperative neuromonitoring [transcranial motor evoked potential (TcMEP) and somatosensory evoked potential (SSEP)] were applied in all patients, but TcMEP was not obtainable in 2 patients (Case 1 and 3). All operations were performed via midline skin incision. First, pedicle screws were inserted 1-2 levels above and 1-2 levels below the index level. The lateral margin of lamina was cut at the junction of facet joint with the ultrasonic osteotome (BoneScalpel, Misonix, NY, USA) (Fig. 1). The lamina was gradually cut with ultrasonic osteotome by slight pushing down its blade against lamina with a vertical motion. When inner cortical bone was cut, loss of resistance was felt and the ostetome was not inserted beyond the depth (Fig. 2A) (Supplementary Video 1 in the online-only Data Supplement). After elevation of cut lamina with clamp, the cranial and caudal ligamentum flavum of elevated lamina was resected with Kerrison rongeur. After laminotomy, the remained facet joint, transverse process and pedicles were removed with conventional rongeur and punch. Spinal nerve roots at the index level were resected bilaterally after no change in intraoperative neuromonitoring (INM) upon 10 minutes of neurovascular bundle clipping. After dissecting the lateral margin of the OPLL mass from the dura, the superior and inferior margin of the beak-type OPLL mass was identified. The base of OPLL mass was removed initially. Next, the OPLL mass attached to dura was removed with the ultrasonic osteotome (Fig. 2B). Use of the ultrasomic osteotome allowed direct resection of the OPLL mass under gentle dural retraction with a suction tip until half of its width was resected. A similar technique was repeated on the contralateral side. After removal of OPLL mass, the removed lamina was replaced by connecting to cranial and caudal lamina with miniplate or translaminar screw (Fig. 3, 4)2229). Finally, rods were fixed to pedicle screws and pedicle screws were inserted at the index vertebra to enhance stability and reduce extent of surgery1). After grafting allobone chips on the decorticated lamina, the surgical wound was closed in a layer by layer fashion.
RESULTS
Patient characteristics, preoperative and postoperative neurological status are described in Table 1. There was no change in TcMEP in Case 2 and 4, and no change in SSEP in all cases. Dura tear was occurred in one case and it was repaired with adhesive sealant without neurological sequel. Postoperative neurological deficits were not encountered in any patients. All patients were discharged within 1 week after surgery. Gait disturbance was improved in Case 2, 3 and 4, but independent walking without assistance was not recovered in Case 1.
Illustrative case : Case 3 (Fig. 3)
A 67-year-old female patient presented with 6 months of paraparesis. Preoperative MR imaging and CT scan showed a beak-type OPLL mass and spinal cord compression at T5-6 (Fig. 3A-D). Cervical laminoplasty was performed 3 years prior due to cervical OPLL, but paraparesis (motor power grade IV/V) developed 2.5 years after her previous surgery. Preoperative JOA score was 2/11 (1+0+0+1). Posterior circumferential decompression and instrumented fusion was performed with the use of the ultrasonic osteotome. With the help of tissue selectivity of ultrasonic osteotome, the OPLL mass could be directly resected from the dura. The final portion of OPLL was difficult to remove, once the mass lost connection with the base of the OPLL mass, due to ineffective transmission of ultrasonic energy. During the operation, there was no significant change in intraoperative SSEP monitoring. TcMEP was not detectable. Dural injury was occurred during removal of OPLL and the defect was repaired with adhesive dural sealant. Postoperative CT scan showed nearly complete removal of the OPLL mass (Fig. 3E-H), but a small fragment of OPLL mass was left (Fig. 2G). The lamina was replaced with mini-plates (Fig. 3I). There was no sequelae associated with the dural tear. The patient's preoperative paraparesis was improved and independent ambulation was possible 1 month after surgery. Ten months after the date of surgery, the JOA score was 8/11 (2+2+2+2); a recovery rate of 67% (Supplementary Video 2 in the online-only Data Supplement).
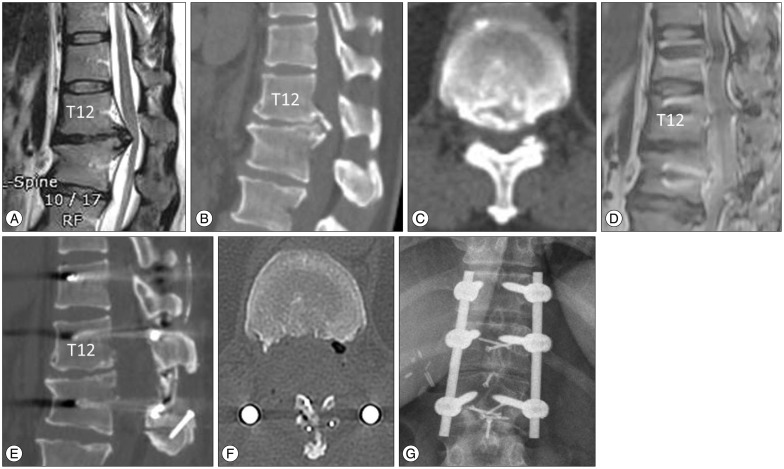
Case 4 (Fig. 4)
Different from Case 3, the base of OPLL mass was removed with ultrasonic osteotome and the OPLL mass was detached and removed from the dura. Because the energy was emitted from the end of osteotome, the T12 root could be safely retracted with the osteotome during resection of OPLL (Fig. 2B), and the T12 root was preserved. Preoperative paraparesis was improved at postoperative month 1 (a recovery rate of 43%) (Supplementary Video 3 in the online-only Data Supplement).
DISCUSSION
In the present cases report we have shown the feasibility of utilizing the ultrasonic osteotome for posterior circumferential decompression operations for thoracic beak-type OPLL. The ultrasonic osteotome has the advantage of tissue selectivity and eliminates the dangerous rotatory motion of the high speed burr, thus allowing a more safe removal of T-OPLL. The nerve root could be preserved with this technique, because of non-rotatory motion of ultrasonic osteotome.
Surgical options for beak-type T-OPLL
There are various kinds of surgical options for beak-type T-OPLL. Direct decompression could be obtained with anterior, posterior or a combined approach. Indirect decompression could be achieved with laminectomy, laminoplasty or a posterior instrumented correction of thoracic kyphosis5811121314151826272830).
Matsumoto et al.13) evaluated various surgical approaches for beak-type T-OPLL in 45 patients; 8 patients underwent laminectomy, 16 underwent laminoplasty, 12 underwent anterior decompression via anterior approach, 5 underwent anterior decompression via posterior approach, 2 underwent both anterior and posterior approach and 2 underwent anterior decompression via sternum splitting approach13). Clinical outcome, surgical technical difficulty and safety are important factors in determining the desired approach. Regarding clinical outcome, removal of the T-OPLL mass seems to be associated with a better outcome; a mean recovery rate of JOA was about 60% with circumferential decompression and about 30-40% with only posterior decompression1328). An anterior approach may be preferable to remove T-OPLL, but the transthoracic/extraplerual approach or trans-sternal approach is technically challenging and is associated with a higher complication rate41618). A recent review on this subject has shown that neurological deficit occurred in 2.7-18.8% of patients after an anterior approach51718). Direct removal of the ossified mass with a posterior only approach may be an alternative, but it has been traditionally challenging secondary to associated kyphotic deformities, adhesion of T-OPLL to the dura and a narrow/blind surgical field316). Direct removal of T-OPLL mass was associated with a high neurological complication rate; neurological deficit occurred when T-OPLL was excised in 7/48 (14.2%), thinned and floated in 7/25 (28%), and left untouched in 4/81 (4.9%)13). The rate of neurologic deficit was especially high for patients with beak-type T-OPLL (30%)11152628). Therefore indirect decompression through instrumented correction of thoracic kyphosis after posterior decompression was suggested as a safe alternative to allow for floating back of the spinal cord132830). However, postoperative magnetic resonance imaging (MRI) demonstrated that indirect decompression was not sufficient after correction of kyphosis alone in 13 out of 15 patients, and 11 patients underwent a secondary procedure for anterior decompression8). Matsuyama et al.16) showed that neurological deterioration occurred in 5/21 patients with beak-type T-OPLL after posterior indirect decompression because of persistent ventral compression. In addition, growth of beak-type T-OPLL was observed 3 years after laminectomy and corrected fusion of thoracic kyphosis25). Although indirect decompression through instrumented correction of kyphsosis was an alternative, considering those results together, direct removal of T-OPLL, especially for patients with beak-type T-OPLL, seems to be an appropriate surgical option.
Ultrasonic osteotome
Neurological deficits usually occurred immediately after surgery in cases of T-OPLL. Therefore, surgical insult to the neural tissue must not be disregarded111226). During surgery, the T-OPLL mass is traditionally removed with a high-speed drill and curette. Neurologic injury may occur during removal of T-OPLL just beneath dura with high-speed drill11). When there are strong adhesions of T-OPLL mass to the dura, use of high-speed drill for removal of T-OPLL may be dangerous secondary to rotatory-motion of the drill6). Ultrasonic osteotome has been used in various surgeries such as plastic surgery, but the usage was not widely spread in spine surgery267202324). Ultrasonic osteotome utilize back and forth micro-motion rather than rotatory-motion, thus energy from the cutting edges of these devises is preferentially transmitted to hard structures, such as lamina27202324). The dura can bend, vibrate and deform to vibratory micromotion with minimal transmission of energy27202324). Moreover, the safety of surgical procedure may be enhanced, because movement of its tip is limited to a fine vibration without problem of bounce of rotatory drill6). This features enable selective removal of beak type OPLL with minimal injury to the dura and spinal cord. The relative tissue selectivity allowed for brief contact with the dura, and thin shaving of T-OPLL and preservation of nerve root were possible (Fig. 2B)27202324). The ultrasonic osteotome may be preferable for removal of T-OPLL over a high-speed drill in this regards27202324). However, the laminotomy with ultrasonic osteotome is performed without direct visualization of dura, and spinal cord injury may occur by insertion of blade beyond the inner cortex of lamina, if penetration of lamina is not felt. Moreover, the pressure of irrigation fluid may injure spinal cord. These shortcomings should be noticed before utilizing ultrasonic osteotome.
CONCLUSION
We have shown the feasibility of an ultrasonic osteotome for thoracic beak-type OPLL. We hope that surgical difficulties might be overcome by utilizing this technique. However, a study with a longer follow-up and a larger number of patients is required to show effectiveness of the present surgical technique.




 XML Download
XML Download