

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Medulloblastoma (MB) is the most common malignant tumor in children, accounting for 15 to 25% of all childhood brain tumors192021). Occurrence in the adult population is also well documented, but only accounts for 1% of adult tumors11). Treatment includes surgical resection followed by radiotherapy of the entire neuro-axis and chemotherapy451923).
Recurrence of this tumor is well recognized and may require salvage therapy. Time to recurrence typically occurs within two years of initial diagnosis in the pediatric population. Tumors that follow Collin's Law (tumor free period of 9 months plus the age at diagnosis) are considered to be cured11920). However, late recurrence of MB has been documented in the pediatric population23121323).
CASE REPORT
History
A 22-year-old male with a history of a medulloblastoma at 9 years of age, removed surgically and treated with adjuvant craniospinal irradiation and chemotherapy presented with 2.5 weeks of progressive gait ataxia and headache.
Examination
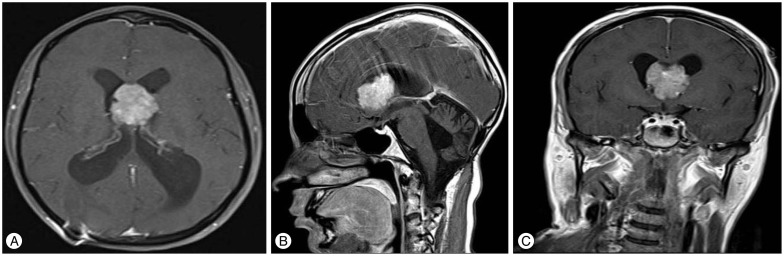
Patient was alert and oriented. The right pupil was sluggish. The left pupil was reactive and the left eye deviated uncontrollably on exam. The left upper extremity had 4/5 strength. CT scan showed an anterior septum pellucidum mass at the foramen of Monro with secondary obstructive hydrocephalus (Fig. 1).
DISCUSSION
Medulloblastoma, a malignant tumor typically arising from the cerebellar vermis in young children and lobes in older children, represents 4–8% of all intracranial tumors, and is the most common malignant central nervous system tumor of childhood192021), with approximately 80% occurring in patients under 15 years of age21). It accounts for 15–25% of all childhood brain tumors in comparison with only 1% of adult intracranial neoplasms, with a slight male predominance in both groups1920212324).
Presenting features of medulloblastoma are generally related to hydrocephalus (found radiographically in 97% of patients) and cerebellar dysfunction which include : headache, nausea/vomiting, truncal ataxia, and unsteady gait23). Approximately 83% are found in the midline in children, while 49% of adult tumors are lateral21).
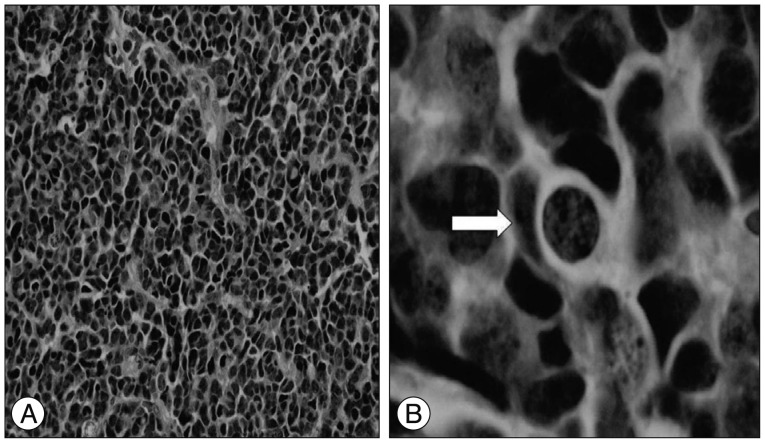
Differences in childhood and adult tumors can also be observed in terms of histologic variant. Classical histologic presentation of medulloblastoma includes densely-packed primitive cells with hyperchromatic nuclei, scant cytoplasm, and nuclear molding120). This classical tumor histology is more common in children821). Homer-Wright rosettes may be seen10). Adults are more likely to have laterally-located tumors, which more often desmoplastic51021). Both tumor types include markers of neuronal lineage, such as class III beta tubulin and MAP-2 neurofilaments, whereas more adult tumors will express GFAP1020). The anaplastic/ large cell variant is more frequently seen in older children and adults.
MB tends to seed the cerebrospinal fluid resulting in extensive leptomeningeal involvement, and treatment therefore requires surgical resection followed by neuro-axis radiotherapy and chemotherapy7171923). Recurrence in the pediatric population differs from that seen in adults. Age at diagnosis has been shown to be a significant predictor of time until relapse24). The majorities of pediatric recurrences are within two years of initial diagnosis, and are in the posterior fossa192024). Those with tumor-free period equal to the age at diagnosis plus nine months may be considered cured (Collin's Law)14181920). While a good predictor of many childhood tumors, there are known exceptions to Collins law for MB1269131822). However, a recent review of 125 patients by Massimino et al.1415), gender, age at diagnosis, metastases, and therapeutic protocol were shown to have no prognostic impact.
In the event of recurrence, relapse at a single site and further out from initial time of diagnosis is considered a more favorable prognostic indicator15). Recurrences are most common in the posterior fossa, followed by spinal, supratentorial and boney metastases23). Supratentorial dissemination is often found in the subfrontal area and may be due to overly generous radiation protection of the orbital roof to prevent irradiation of the cribiform plate, allowing for a nidus of recurrence16). Late recurrence of MB in the supratentorial ventricular compartment is uncommon. We present a case of late recurrent MB 13 years after initial diagnosis, again validating the need for long term follow-up in the pediatric population following diagnosis of MB.
CONCLUSION
Recurrence of MB is common and often occurs in the posterior fossa. Supratentorial dissemination of MB is more common in the subfrontal region. Supratentorial recurrence of MB not following Collin's Law is extremely uncommon, especially within the supratentorial ventricular system. We present a case of a 22 years old male who presented 13 years following his initial diagnosis of MB with symptoms of obstructive hydrocephalus from a septum pellucidum recurrence. Continued close follow-up is need in pediatric patients after resection and radiation for MB given their unexpected recurrence pattern.

 XML Download
XML Download