

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is a rare tumor in Western countries, accounting for less than 2% of all neoplasms in United States. In contrast, HCC is relatively common in Asian countries, where the hepatitis B virus is endemic27). The survival of patients with HCC has been prolonged with improvements in various diagnostic tools and treatment modalities1023). HCC has been also reported to metastasize frequently to the skeletal system-vertebrae, pelvis, ribs, etc.-with an incidence ranging from 2% to 16%122226). It is estimated that 40% of bone metastases are spinal metastases15). Consequently, spinal metastases from HCC are diagnosed more frequently.
The treatment of metastatic spine disease has evolved significantly in the past decade with the advancements in surgical and radiation techniques2). As surgical techniques and instruments improve, surgical treatment followed by adjuvant radiotherapy is affording a longer survival period and better quality of life than radiotherapy alone92128). Recently, a minimally invasive surgical technique, spine radiosurgery, and new targeted chemotherapy have been introduced. These treatment modalities are being applied clinically4813172435). If a patient experiences neurologic deterioration or loss of stability, surgical decompression and stabilization with instrumentation may be a better option than radiotherapy, considering the delayed response of solid tumors to radiotherapy692834).
The aim of the study was to determine the long-term surgical treatment outcomes associated with the systemic condition of HCC presenting with spine metastases, and to figure-out the survival-related factors.
MATERIALS AND METHODS
Patient selection
Patients who underwent an operation for spinal HCC metastases from February 2005 to December 2013 in the Spine Center of the authors' institute were enrolled in this study. All patients complained of neck pain or back pain. Some patients had neurologic symptoms, including lower extremity weakness or urinary retention. Patients with susceptive instability, spinal instability neoplastic score (SINS) over score of 6, and/or patients who already received radiotherapy, or stereotactic radiosurgery, underwent operation. Patients who underwent a vertebroplasty or Kyphoplasty procedure were not included in this study
Patient demographics and clinical characteristics were obtained from the patients' electronic medical records. We evaluated the patients' predisposing factors for primary HCC. The general condition of patients, including liver function, was evaluated using the Child-Pugh classification29). To evaluate instability of tumor SINS was calculated11). To evaluate a condition of tumor the Tokuhashi scoring system (general condition, number of extraspinal bone metastases foci, number of metastases in the vertebral body, metaseses to the major internal organs, primary site of the cancer, and palsy)31), and the Tomita scoring system (primary site of the cancer, number of visceral metastases, and number of bone metastases)32) was calculated in all patients. Recently, the authors have proposed revisions, resulting in modified Tomita and Tokuhashi scoring systems for spinal metastasis20). We applied these scoring systems also. Instability was evaluated with SINS11). Ambulatory function was evaluated from medical records. A patient who could walk even with an ambulatory aid was considered as possible, and a patient who could not walk at the out-patient department after the operation was considered as not-possible. Chemotherapy regimen was retrospectively evaluated from prescription of medical records.
Surgical and radiation intervention
Patients with refractory pain, neurological deficit, or the potential for neurological deficit were indicated for surgery. Thirty-three patients with spinal HCC metastases underwent operations. Three patients had two spinal operations each, at different levels, so 36 operations were performed in all. The goals of the metastatic spinal tumor surgery were : to decompress a neural component and/or stabilize the spine to improve neurological deficits and alleviate pain. In most cases, instrumentation was performed for stabilization, by anterior, posterior, or circumferential means.
Preoperatively, conventional radiotherapy to the index spine was performed in 11 cases (total dose range, 20 Gy to 39 Gy). One patient received stereotactic radiosurgery with 20 Gy/1 Fr.
Statistical analyses
Statistical analyses of variables were carried out using commercial software (PASW Statistics, version 22; SPSS Inc., Chicago, IL, USA). The survival rate was estimated by the Kaplan-Meier method, and differences were analyzed by the log-rank test. Comparison between preoperative status and postoperative status was analyzed by a Wilcoxon signed rank test. The results were considered significant for probability values less than 0.05.
RESULTS
Patients and tumor characteristics
Thirty patients were male, and 3 patients were female. The patients' median age at the initial operation was 56 years (range, 28 years to 71 years). Four patients had been diagnosed with spinal metastases simultaneously (within one month) of their primary HCC diagnoses. In the other 29 patients, the spinal metastases occurred more than 6 months after the diagnosis of primary HCC (median interval, 18 months; range, 6-86 months). Twenty-nine patients were hepatitis B viral carriers, one was a hepatitis C viral carrier, and other three patients were non-hepatitis B, non-hepatitis C viral carriers. Among the three patients, one patient had a history of heavy alcoholic consumption. Preoperatively, 29 patients were Child-Pugh class A, 4 were class B, and no patient was class C. Preoperatively, 11 patients lost their ambulatory function, and 25 patients maintained their ambulatory function. Some required ambulatory aids. There was no statistically significant difference between the pre-and post-operative status of Child-Pugh classification and ambulatory function. Spinal metastases were located at the cervical level (n=10), thoracic level (n=15), and lumbar level (n=11). In terms of SINS, 2 patients were score of 6, 29 patients were between 7 and 12, 5 patients were between 13 and 18.
Among the subjects, there were several post-operative complications. One patient died during admission due to pneumonia. There was one case of cerebro-spinal fluid leakage after a dural tear. There was one case of operative site infection.
Survival analysis
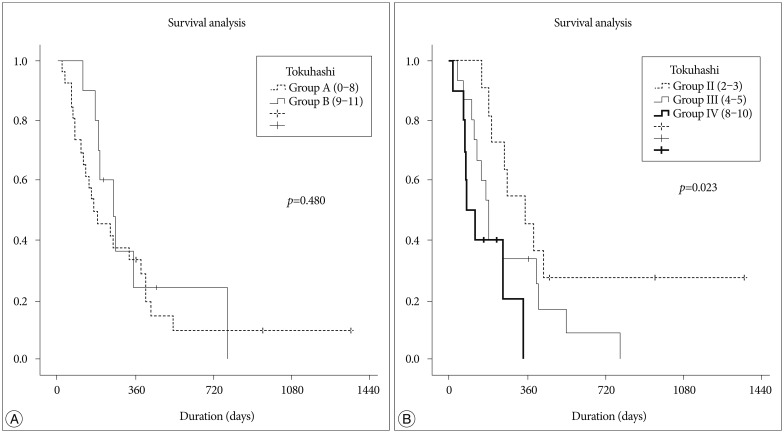
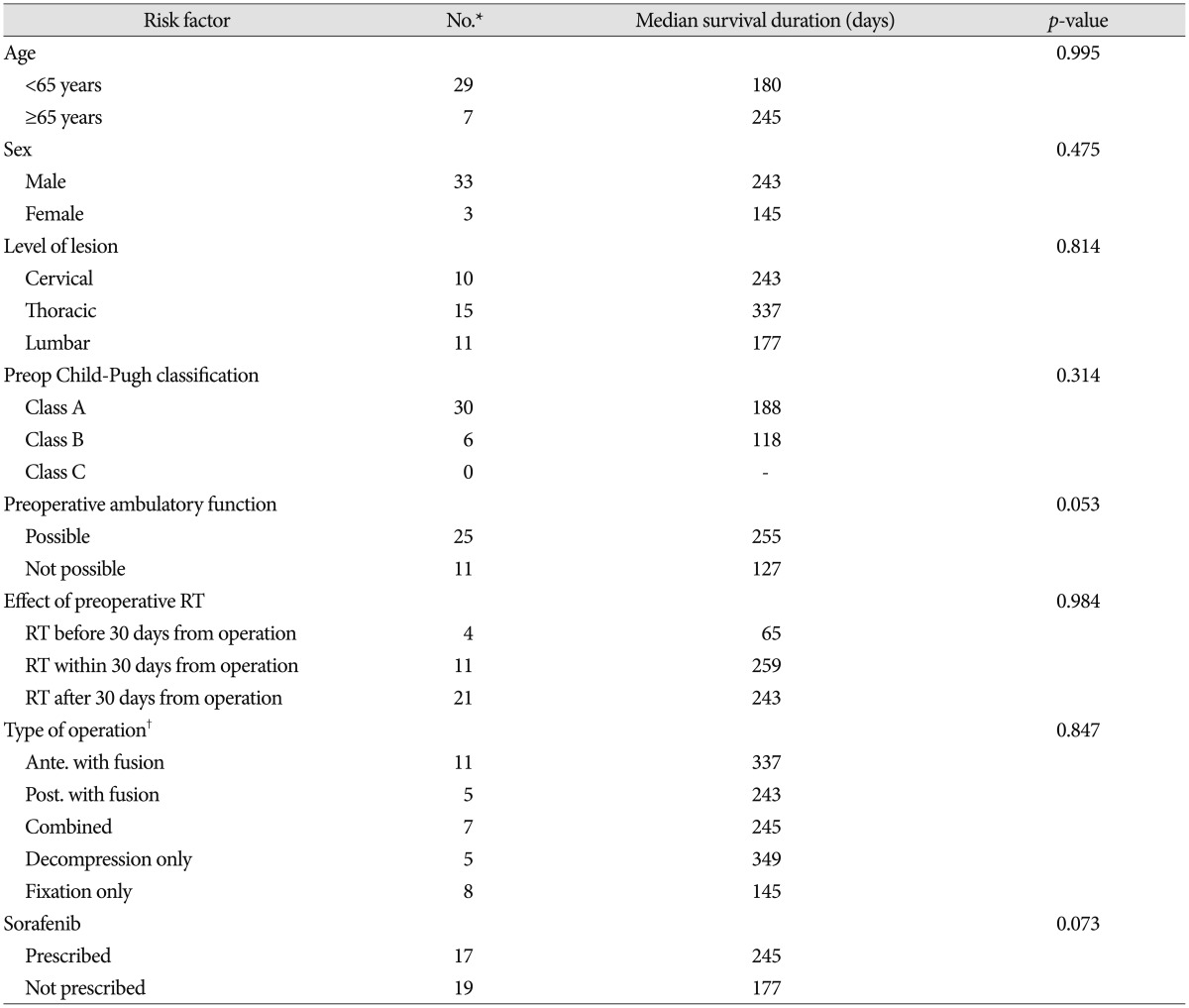
During the follow-up period, 27 patients died, three patients were lost to follow-up, and three patients survived. The median overall survival was 261 days (range, 22-1359 days) after the diagnosis of metastasis, and 180 days (range, 19-1351 days) after the initial operation. As determined by Kaplan-Meier survival analysis, the survival time was not related with age, sex, location of tumor, preoperative Child-Pugh classification, preoperative ambulatory function, preoperative radiotherapy status, type of operation, or the administration of Sorafenib (Table 1).
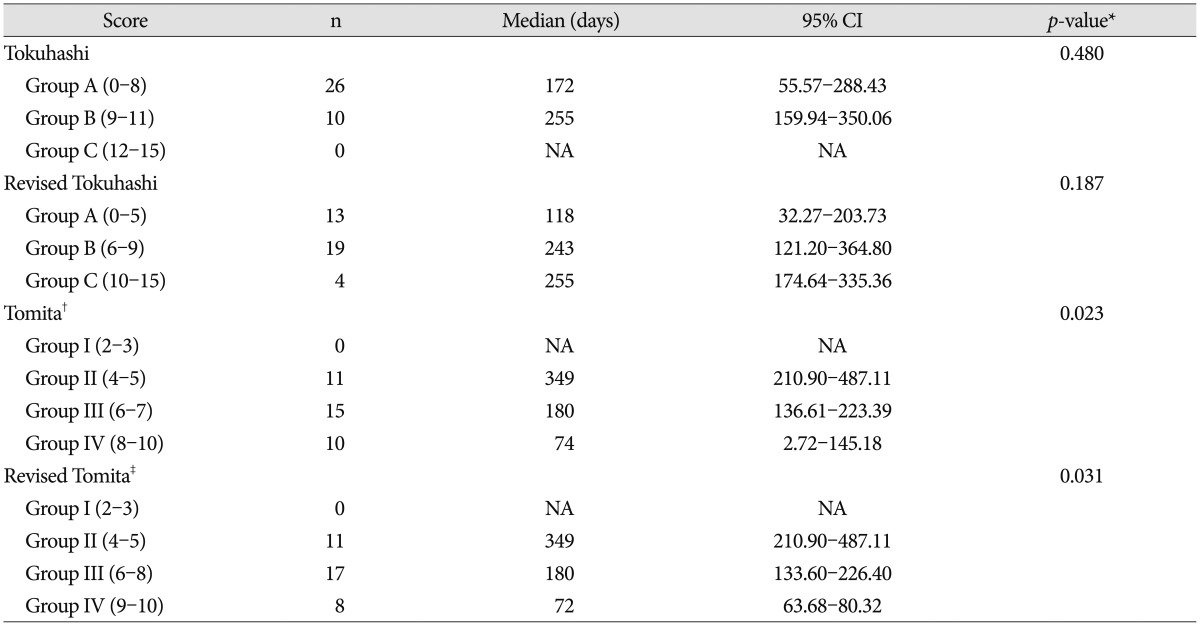
Patients were classified by Tokuhashi but the classifications showed no significant difference between groups. When patients were classified by Tomita score, there was a statistically significant difference between the groups (p=0.023). Applying the revised Tokuhashi and Tomita scoring systems, the results were quite similar (Table 2, Fig. 1).
DISCUSSION
The survival time of patients with HCC has increased to more than 2 years during the past decade33). Hence, it is more common to encounter a patient with spinal metastases. Spinal metastases can cause neurologic deficits with or without compression fractures, and back pain, both of which affect the patient's quality of life and result in poor outcomes1). Recent studies show poor overall survival after a diagnosis of spinal metastasis, usually around a year71936). Therefore, spinal metastasis from HCC is still devastating to patients.
Prognostic factors
There were several studies conducted to estimate prognosis of spinal metastases using different parameters. Chen et al.7) compared the existing preoperative scoring systems-the Tokuhashi scoring system, the Tomita scoring system, the van der Linden scoring system, and the Bauer and Wedin scoring system-to find useful prognostic factors. They found the Tokuhashi scoring system provided statistically significant results. In addition, serum albumin (≥37 g/L) and LDH (<200 U/L) were found to be better prognostic factors. However, our study and a study by Zhang et al.36), show the Tomita scoring system is an independent prognostic factor. These studies show the limitations of the existing preoperative scoring system, and suggest a need for a new prognostic scoring system. Due to advances in medical treatment and anesthesology, researchers have proposed a new prognostic scoring system by modifying the Tokuhashi and Tomita scoring systems20). The resulting systems seem to be more prognostic than previous scoring systems for patients with tumors of the entire spine. But, with the small number of patients, the validation was limited in this study. Kim et al.19) suggest that preoperative ambulatory status and hepatic function (Child-Pugh classification) were significantly correlated with survival time. But, Child-Pugh classification was not shown to predict the prognosis of HCC patients with spinal metastases in our study.
Treatment strategy
The current recommendation of high-grade spinal cord compression for solid spine metastases is surgical decompression and radiotherapy to achieve local tumor control. Patchell et al.28) in 2005 showed better outcomes for patients undergoing surgery and radiation therapy compared to patients undergoing radiation treatment alone. The optimal interval between surgery and radiotherapy was studied using a systemic review18). They suggested the time interval between treatment modalities should be at least 1 week to minimize wound complications.
Maranzano and Latini25) reported that radioresistant tumors, such as HCC, demonstrated only a 20% response rate in conventional radiotherapy; in contrast, radiosurgery for spine metastases has demonstrated better clinical responses. Yamada et al.35) published a prospective cohort study, regarding treatment with radiosurgery for radioresistant oligometastatic tumors. With dose-escalation from 18 Gy to 24 Gy, local control was 92%. Many other studies reported that radiosurgery for metastatic spine disease is safe and effective with durable symptomatic responses and local control for radioresistant histologies3451430). As confidence and experience with the use of radiosurgery as a postoperative adjuvant grow, surgical resection of metastatic disease has become less aggressive, with the expectation that radiosurgery will control the residual disease. We validated the effect of radiation therapy in our patient cohort. Preoperative radiation therapy was not shown to help prolong the overall survival of the patients. Upfront radiation therapy was also ineffective in prolonging the overall survival of the patients.
Recently, target agents have been suggested to be a promising treatment modality. Sorafenib is an orally active multi-kinase inhibitor that has proven to prolong overall survival and progression-free survival in advanced HCC824). But, the difference of survival time between the group who were prescribed Sorifenib and the group that did not receive it was not significant in the HCC with spinal metastasis patients.
Neurologic restoration
The most important goal of surgical resection in patients with spinal metastases is to preserve or restore neurological function. Kim et al.19) reported a 29% (4/14) rate of restoration of ambulatory function. Preoperative ambulatory ability was significantly correlated with the postoperative ambulation period in their study16). Previously, Chen et al.7) reported a restoration rate of more than 50%. In contrast, our study shows an 18% (2/11) rate of restoration of ambulatory function. In fact, there was no difference of ambulatory ability status between pre- and post-operatively in the present study. Most patients had surgical decompression within a week after visiting the hospital. However, 6 patients visited the hospital more than one week after the symptom occurred, and some came after 20 days. The population of the other study underwent operations within 3 days. This difference might have affected the result.
As this result is based on a retrospective medical record review, the data is limited, and a prospective study should be conducted to further validate its findings.
CONCLUSION
For patients with spinal metastases from HCC, survival time was not correlated with age, sex, level, preoperative Child-Pugh classification, preoperative ambulatory function, preoperative radiotherapy, type of operation, administration of Sorafenib at any point, or the Tokuhashi scoring system. Only the Tomita scoring system was shown to provide practicable and highly predictive prognostic value in patients with spinal metastases from HCC. Considering the other reports, the existing scoring system has limitations for patients with spinal metastses. A new prognostic scoring system should be introduced. Still, surgical treatment is a prerequisite for the restoration of stability or immediate decompression. The technology and other advancements in chemotherapy and radiotherapy are rapidly improving, so target agents or radiosurgery are potentially very promising. With the advent of effective multimodality treatments, the patients' survival and quality of life will be improved.
 XML Download
XML Download