

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Meningioma is the most common primary brain tumor in adults according to the recent population-based data from Korea and the Central Brain Tumor Registry of the United States91623). As brain imaging has become a routine practice nowadays, incidental or asymptomatic meningiomas are seen more frequently than before, and they can be managed successfully by stereotactic radiosurgery (SRS) in selected cases. The excellent long term local tumor control (LTC) rate and greater safety of SRS for meningiomas are well appreciated with the LTC rates at 5 to 10 years of 87 to 98%121326273032).
However, adverse radiation effects such as increased peritumoral brain edema (PTE) may develop after SRS and are not uncommon accounting for 15% to 28% of unselected cases23121417182029), and it has been reported to cause neurological symptoms in 3% to 15%31820262932). Large tumor volume (>4.2 cc to 10 cc), hemispheric tumor location, higher prescription dose (>15 Gy to 16 Gy), and pre-treatment PTE have been associated with an increased risk of the development of PTE after SRS1112141720262832). Meanwhile, the risks and the clinical course of PTE after primary SRS for asymptomatic intracranial meningiomas are not clearly elucidated without being based on clinical data on large homogenous cohort of asymptomatic tumors. Herein, we did a retrospective study on 320 patients with asymptomatic meningiomas treated with SRS as a primary modality and investigated the incidence, risk factors, and pattern of evolution of PTE after SRS using a serial volumetric analysis of magnetic resonance images (MRIs).
Go to : 
MATERIALS AND METHODS
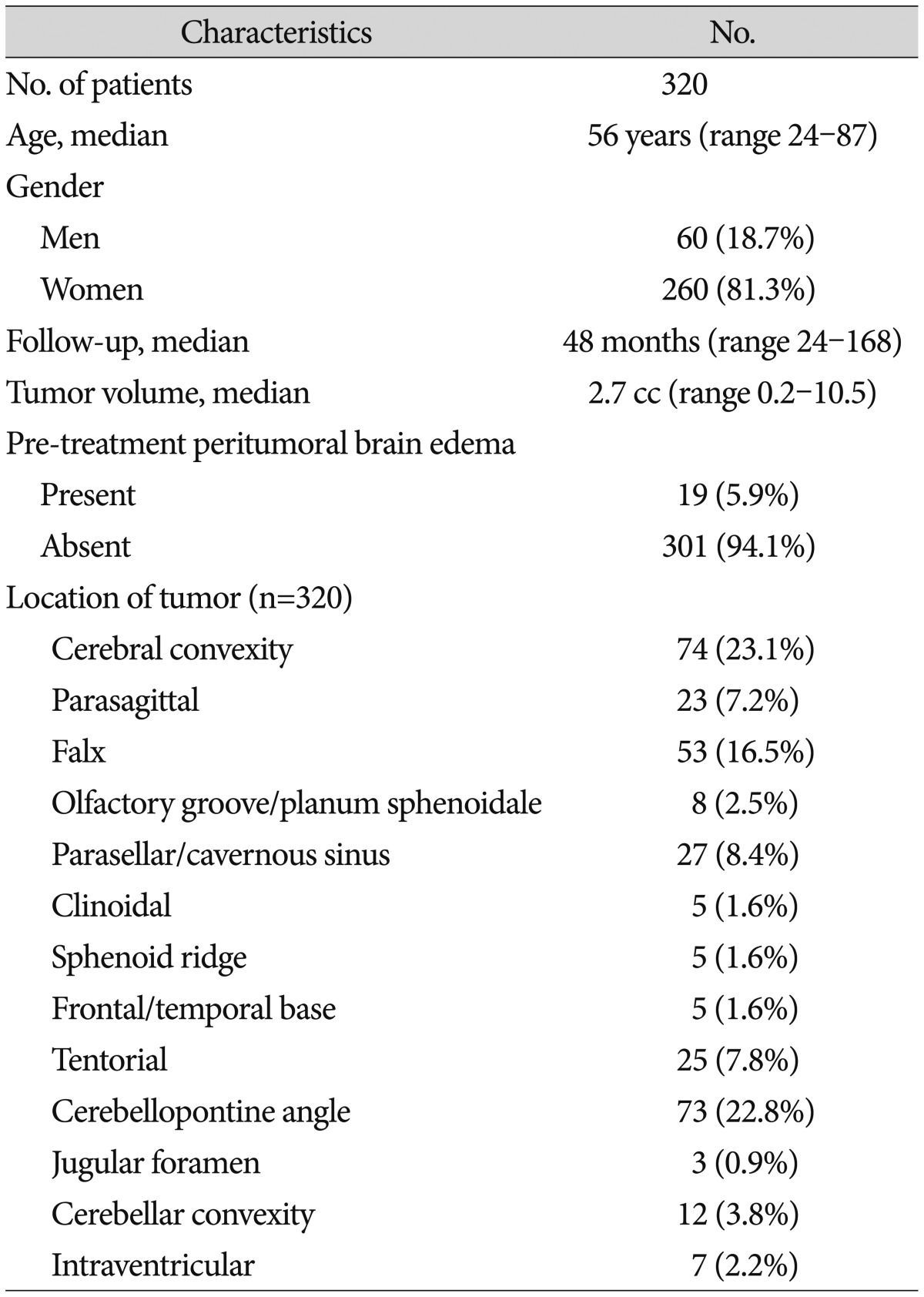
Patient and tumor characteristics (Table 1)
This study was approved by our institutional review board. Among a total of 857 consecutive patients who underwent SRS using Gamma Knife (Elekta AB, Stockholm, Sweden) for intracranial meningiomas at our department between 1998 and 2012, those with asymptomatic tumors who had been followed up a minimum two years using MRI after SRS were included, and those with multiple meningiomas or who received a prior surgical resection or any form of cranial irradiation were excluded. By these criteria, a retrospective cohort of 320 patients harboring 320 meningiomas was identified. The follow-up duration ranged from 24 months to 168 months (median 48 months). There were 260 women (81.3%) and 60 men with the median age of 56 years (range 24-87 years). The median tumor volume was 2.7 cc (range 0.2-10.5 cc) and the location of tumor varied as shown in Table 1. Pre-treatment PTE was present in 19 tumors (5.9%).
Stereotactic radiosurgery and radiosurgical parameters
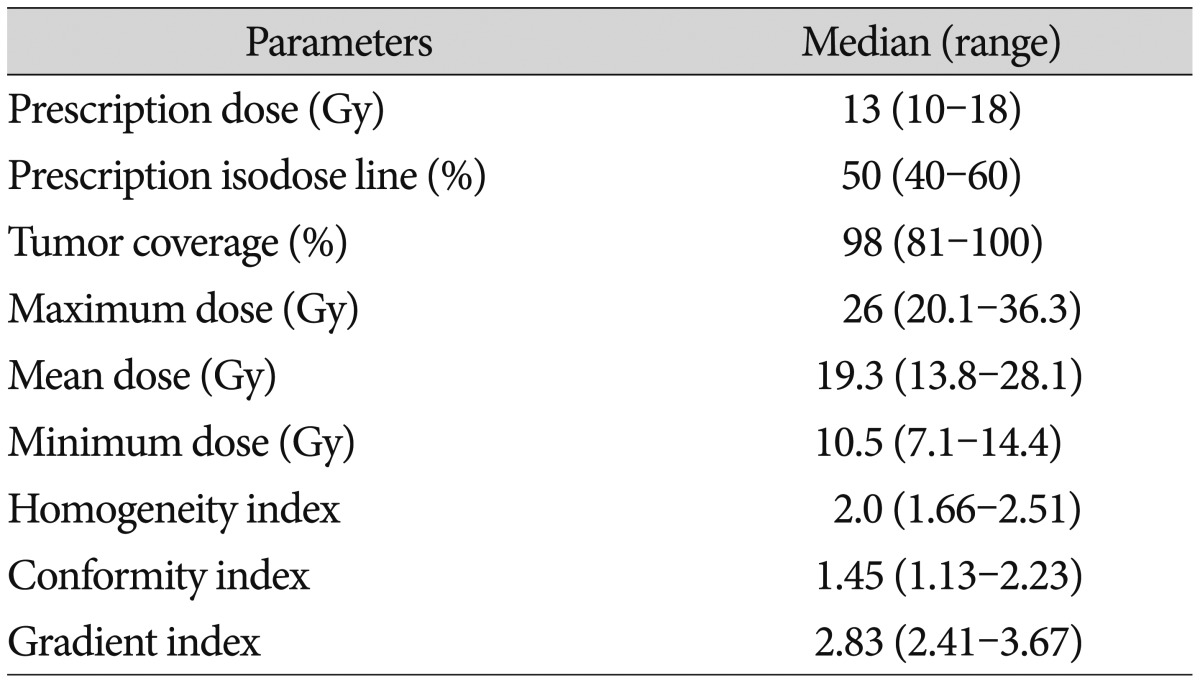
All patients were treated using one of Leksell Gamma Knife units B, C, or Perfexion. Treatment plans were generated using the Elekta GammaPlan system based on gadolinium-enhanced axial 3-dimensional T1-magnetization-prepared rapid acquisition gradient echo MR images (1.5 mm slice thickness) fused with CT images (1.25 mm slice). The optimal plan was produced by adjustment of the collimators and sectors such that optimal dose coverage of the target was achieved while minimizing dose to the surrounding normal tissues. The median prescription dose was 13 Gy (range 10-18 Gy; mean±SD=13.0±1.3 Gy) with the median prescription isodose line of 50% (range 40-60%). The quality of each radiosurgical plan was assessed using tumor coverage, the maximum, mean, and minimum doses, the homogeneity index (HI), the conformity index (CI), and the gradient index (GI). HI was measured as the ratio of the maximum dose over the prescription dose. CI was defined as the ratio of prescription isodose volume to the volume of tumor receiving the prescription dose or more. GI was the ratio of the isodose volume receiving 50% of the prescription dose to prescription isodose volume. The median tumor coverage was 98% (range 81-100%). The median maximum dose was 26 Gy (range 20-36 Gy). The median values (ranges) of HI, CI, and GI were 2.0 (1.66-2.51), 1.45 (1.13-2.23), and 2.83 (2.41-3.67), respectively (Table 2).
Follow-up examination and serial volumetric analysis of MRI
Clinical examination and MRI after SRS were performed at 3-months to 6-month intervals during the first year, annually for two years, and biennially thereafter. If patients exhibited any relevant symptoms or signs, more frequent follow-up was carried as needed.
Volumetric data sets for tumors and PTE on serial MRIs were obtained using the in-house software based on the ImageJ, a java-based image processing program developed at the National Institutes of Health (http://rsbweb.nih.gov/ij/). Each image slice was cropped at the margin of the target area (either tumor or PTE), and the target volume was calculated as the sum of the areas multiplied by the slice thickness. Treatment failure or tumor progression was defined either as an increase of tumor volume ≥15% compared with the baseline tumor volume or as marginal tumor growth, and stable disease was designated for tumor volume changes within the range of ±15%. The edema index (EI) was defined as the ratio of peritumoral high signal intensity volume including tumor volume on T2-weighted or fluid-attenuated inversion recovery MRI to tumor volume on T1-weighted gadolinium-enhanced MRI. In each tumor, serial EIs were measured on follow-up MRIs after SRS, and the relative edema indices (rEIs) were calculated from these values normalized against the baseline EI. Any neurological symptom that matched increased PTE on MRI was regarded as symptomatic PTE.
Statistical analysis
LTC was estimated using the Kaplan-Meier method calculated from the treatment start date to the date of events or the last follow-up. Factors possibly affecting the development of PTE including age, gender, tumor volume (≥4.2 cc vs. <4.2 cc; the volume equivalent to a diameter 2 cm) and location, pre-treatment PTE, prescription dose, prescription isodose line, tumor coverage, the maximum, mean and minimum doses, HI, CI, and GI were tested using logistic regression for univariate analysis. Tumor location was grouped into two categories : category 1 (mostly of hemispheric location, 64.1%) where tumors maintaining a scant intervening cerebrospinal fluid (CSF) space in between the tumor and the adjacent brain included cerebral convexity, parasagittal, falx, olfactory groove/planum sphenoidale, sphenoid ridge, frontal/temporal base, tentorial, and cerebellar convexity locations vs. category 2 (mostly of skull base, 35.9%) where tumors possessing a relatively sufficient CSF space in between included clinoidal, parasellar/cavernous sinus, cerebellopontine angle, jugular foramen, and intraventricular locations. Factors with p values of 0.05 or less in univariate analysis were accepted as statistically significant and then included in multivariate logistic regression model. All statistical tests were conducted using the SPSS Version 21.0 (SPSS, Chicago, IL, USA) and the R software Version 3.1.1.
Go to :
RESULTS
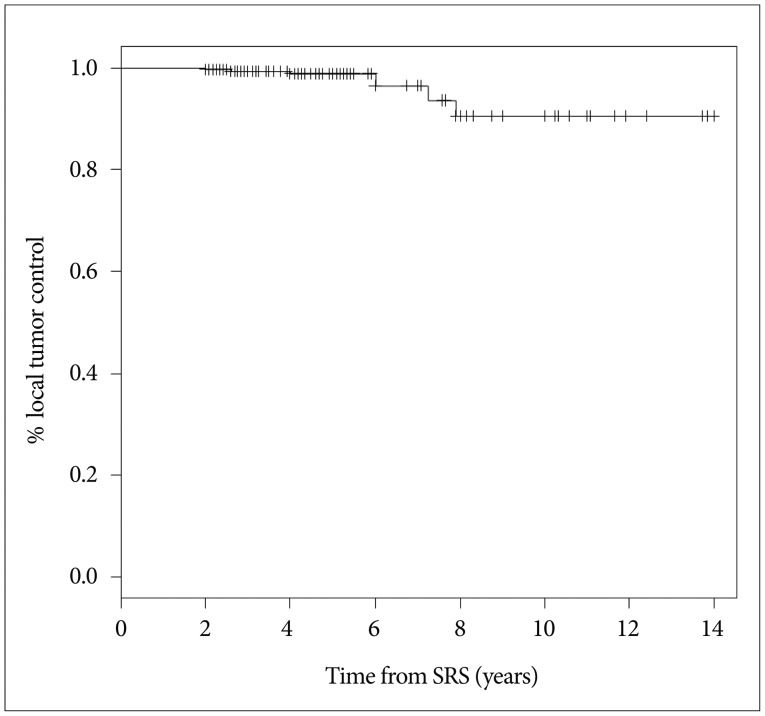
Local tumor control was achieved in 313 of 320 patients (97.8%). The estimated LTC rates at 5 and 10 years were 98.8% and 90.5%, respectively (Fig. 1). Tumor volume decreased in 191 patients (59.7%), remained unchanged in 122 (38.1%), and increased in 7 (2.2 %).
Newly developed or increased PTE on MRI (defined as rEI ≥1.25) was noted in 49 patients (15.3%), among whom it was symptomatic in 28 patients (57.1%; 8.8% of the entire cohort) causing seizure (n=13, 46.4%), aggravating headache (n=12, 42.9%), or hemiparesis (n=6, 21.4%). Those patients with symptoms were medicated with a temporary course of steroids, and none of them underwent a craniotomy.
Risk factors for peritumoral brain edema after SRS
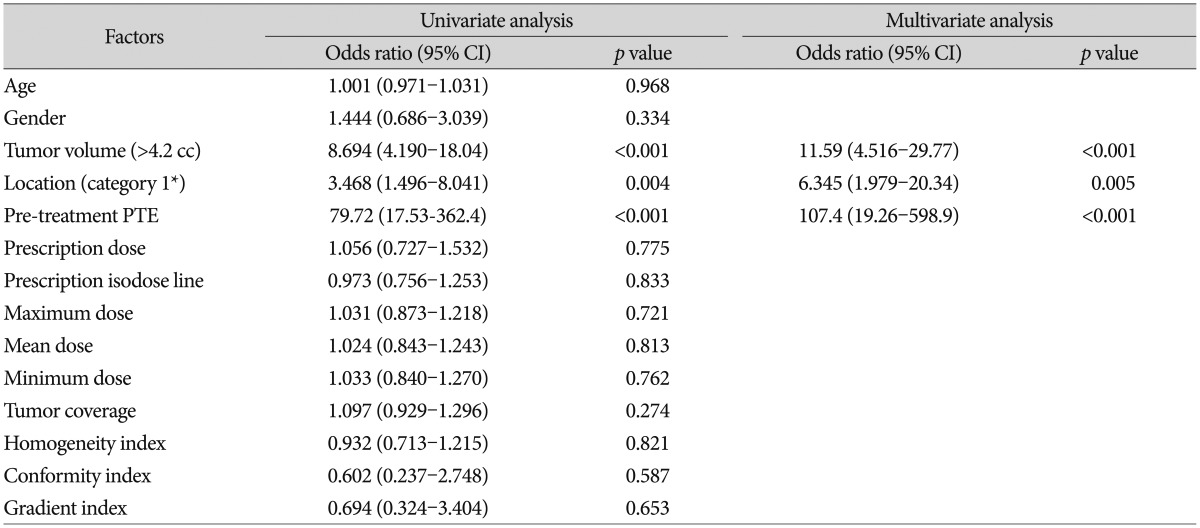
In both univariate and multivariate analyses, tumor volume larger than 4.2 cc (p<0.001 in multivariate analysis), tumor location of category 1 (p=0.005), and the presence of pre-treatment PTE (p<0.001) were associated with an increased risk of the development of PTE after SRS (Table 3). Radiosurgical parameters did not affect the development of PTE.
Pattern of evolution of peritumoral brain edema after SRS
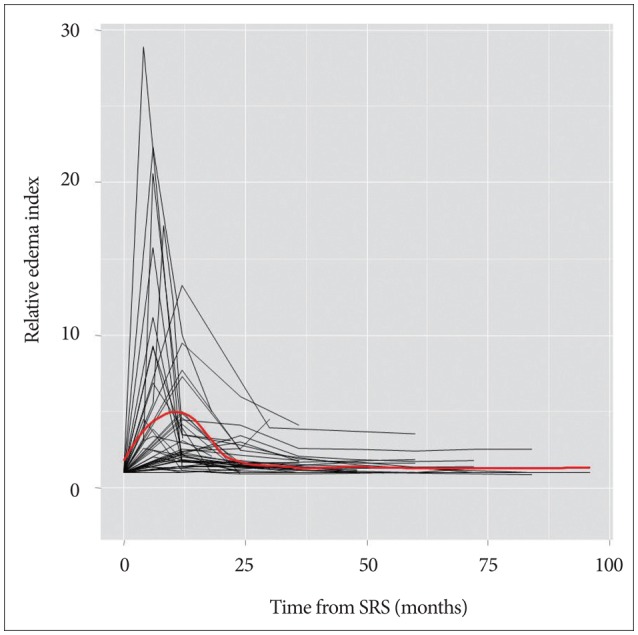
rEIs in tumors with increased PTE were plotted over the time after SRS and fitted to a LOESS curve (Fig. 2). The maximum value of rEI was 4.96±0.45 (mean±SEM) at 11 months after SRS. The time window for three-fold (halfway between the baseline and the maximum rEIs) or more increase of PTE was 15 months starting from 3 months and ending at 18 months after SRS. rEIs decreased to 1.70±0.50 at 24 months after SRS.
In 28 patients who developed symptomatic PTE, the maximum value of rEI was 4.99±4.20 (mean±SD) at the time of median 12 months (range 4-48 months) after SRS. The median time to symptom onset was 6 months (range 3-18 months), and the median duration of symptoms was 6 months (range 3-78 months). A representative case is illustrated in Fig. 3. In most patients (24 of 28 patients, 85.7%), symptoms were transient and resolved completely within 24 months, but were sustained for more than 24 months (24, 33, 71, and 81 months) in 4 patients.
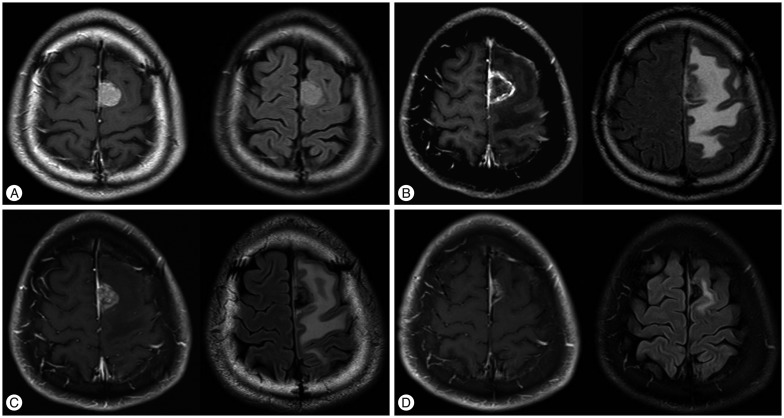 | Fig. 3A 38-year-old man with asymptomatic parasagittal meningioma. Each pair of gadolinium-enhanced T1-weighted MRI and fluid-attenuated inversion recovery MRI is presented before (A), 6 months (B), 10 months (C), and 13 months (D) after Gamma Knife (GK) with a marginal dose of 13 Gy. A : The tumor volume was 6.1 cc and no peritumoral edema is seen before GK. B : He developed seizure and hemiparesis 6 months after GK. Note the internal necrotic change of tumor combined with a substantial amount of peritumoral edema. C and D : Edema decreased at 10 months (C) and nearly disappeared at 13 months (D) after GK. His symptoms resolved completely.
|
Go to :
DISCUSSION
Treatment options for asymptomatic intracranial meningiomas include observation, surgery, and radiotherapy including SRS. Because many of these tumors are small in size, SRS which is less invasive and safer than but comparably effective as open surgery is often a preferred option when treatment is considered and as such, is increasingly used in this subgroup of meningiomas. Nevertheless, the prophylactic use of SRS for the purposes of tumor control and prevention of symptom development must be carefully balanced against the indolent natural history of benign meningiomas and potential risks of adverse radiation effects. According to studies on the natural history of meningiomas in the literature, tumor growth has been demonstrated in 22% to 63% of tumors during the mean (or median) follow-up of 2.5 to 4.2 years8151921243334), and 13% to 26% of cases eventually developed symptoms or required treatment192433). With the median follow-up of 48 months in the present study, only 7 of 320 tumors (2.2%) increased in volume >15%, and tumor volume decreased in 59.7% of cases, demonstrating that SRS significantly altered tumor growth patterns. On the other hand, 49 tumors (15.3%) developed an increased PTE on MRI after SRS, and it caused neurological symptoms in 28 patients (8.8%) probably affecting the activities of daily living adversely, emphasizing the importance of better understanding the risk factors to avoid this potentially serious complication.
Among various factors that have been reported to be associated with an increased risk of the development PTE after SRS, factors such as large tumor volume, hemispheric tumor location, higher prescription dose, and pre-treatment PTE are commonly appreciated based on large clinical studies37121420252632), which is almost consistent with the present study. Cai et al.2) suggested the tumor-brain contact interface area as a strong predictor for the development of PTE and proposed a mechanistic relationship of the tumor-brain interface disruption by virtue of tumor growth (large tumor volume) and SRS treatment to the consequent formation and/or aggravation of PTE after SRS. In addition to this concept, we focused on the amount of intervening CSF in between tumor and the brain, which may act as a mechanical and biochemical buffer against mediators released from tumor. As expected, tumor location where tumors maintaining a scant amount of intervening CSF (mostly hemispheric vs. skull base) was independently associated with a significantly increased risk of PTE. Lines of evidence support that PTE in meningiomas is vasogenic, not cytotoxic and associated with increased vascular permeability of meningioma tissue, not surrounding normal tissue1531). Intrinsic tumor factors that have been implicated in the development of PTE include certain histological subtypes (angiomatous, microcystic, and secretory), higher histological grade, high proliferation index, and expression of the markers of angiogenesis and hypoxia (vascular endothelial growth factor and hypoxia-inducible factor-1)1022). Considering these facts, it is not surprising that radiosurgical parameters other than dose to tumor (prescription dose and maximum dose) are not associated with the development of PTE612172028). The present study did not found prescription dose as a significant risk factor, because most patients had been treated with prescription dose <15 Gy (13.0±1.3 Gy).
Similar to the results in the present study, PTE and symptoms caused by it after SRS represented a more or less typical course and resolved within 2 years in the majority of cases2310111328), and the chronological patterns of PTE fairly matched the clinical courses of patient symptoms2111225). In our analysis, PTE on MRI developed or increased within months, reached its maximum extent of five-fold over the basal level at 11 months, and decreased thereafter to below two-fold over the basal level until 2 years after SRS, and the time to symptom onset and its duration approximated to this pattern of PTE. Permanent deficits from PTE after SRS have been reported in less than 3% and were rarely disabling41230), although exceptional fatal cases have been also reported26). In the present study, 4 of 320 patients (1.3%) harbored sustaining neurological symptoms beyond 2 years.
This study represents the largest clinical series of asymptomatic meningiomas treated with primary SRS and provides a useful clinical picture on the risks and the chronological course of PTE in this subgroup of meningiomas that will be encountered more frequently henceforth. Careful patient selection is of utmost importance in planning for the safest treatment.
Go to :
CONCLUSION
Although SRS is effective and safe in by far the majority of patients with asymptomatic meningiomas, a small fraction of patients may suffer from the development of PTE after SRS. Caution should be exercised in decision-making on SRS for tumors of large volume (>4.2 cc), of hemispheric location, or with pre-treatment PTE. In case, PTE usually develops within months, reaches its maximum degree until a year, and resolves within 2 years after SRS.
Go to :
 XML Download
XML Download