

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic subdural hematoma (CSDH) is a common disease in the neurosurgical field, particularly in the elderly.
The most common cause of chronic subdural hematoma is head trauma; other causes include coagulopathy, anticoagulant therapy, metastatic tumor, vascular malformations, and alcoholism210). Symptoms vary, including headache, motor weakness, amnestic deficit, and lack of concentration.
Surgical treatment of CSDH in symptomatic patients is still the "gold standard" of therapy because it enables immediate decompression of the space-occupying lesion and significantly improves outcome. Nonsurgical treatment of CSDH could be administered in situations such as poor general condition or elderly patients who favor nonsurgical treatment.
The reasons for spontaneous resolution of CSDH are unclear. Herein, we report on a case that showed spontaneous resolution of a large CSDH and review the literatures on spontaneous resolution and nonsurgical treatment of CSDH.
CASE REPORT
An 87-year-old woman presented with confused mentality and right side weakness of motor grade II for 10 days. She had a history of head trauma one month ago. She had no history of alcoholism or anticoagulant therapy. After visiting a local hospital and undergoing computed tomographic (CT) scan, she was diagnosed as CSDH and transferred to our hospital for surgery.
When she visited our hospital, her Glasgow coma scale score was 14, mental state was light drowsy, motor grade was right hemiparesis of grade II, and Mini-Mental State Examination score was 11/30.
She had no underlying disease and a previously healthy state. Initial laboratory studies and vital signs were all within normal range.
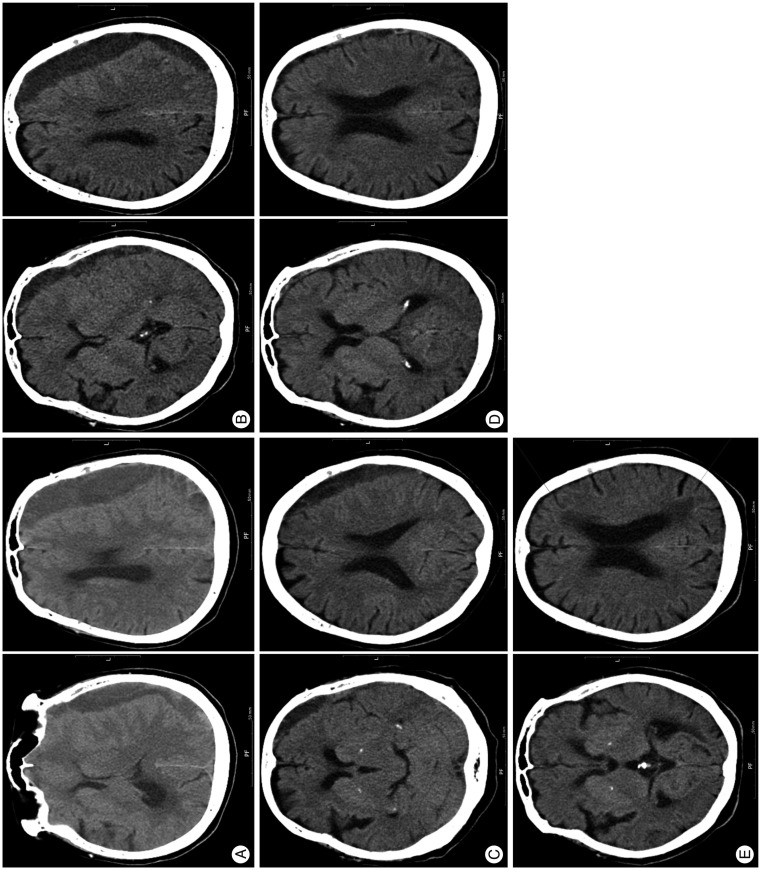
The initial CT scan showed a 22 mm thick low density lesion located in the left fronto-temporo-parietal region with 12 mm midline shift to the right (Fig. 1A). Based on the CT scan and the patient's status, it was a definite indication for surgical treatment. Although we recommended surgical management to the patient's family, they refused because of the patient's old age and the risk of surgery. Therefore, we prescribed anticonvulsant (valproate sodium) only and planned on close observation of the patient with follow up brain CT.
The patient underwent 5 CT scans. Follow up brain CT scan after 1 month showed a decreased amount of hematoma (Fig. 1B). The thickness of SDH in the left fronto-temporo-parietal convexity was 12 mm. The patient's mental status was improved to alert and the right side hemiparesis symptom improved to motor grade 4. The brain CT after 2 and 3 months showed a gradual subsiding of the SDH (Fig. 1C, D). Patient's right hemiparesis had disappeared and self-ambulation was possible. Follow up brain CT scan after 5 months showed disappearance of the CSDH and the patient was neurologically normal (Fig. 1E).
DISCUSSION
In the literature, spontaneous resolution of CSDH has rarely been reported and the reason for spontaneous resolution of CSDH remains unclear. However, several theories have been proposed to explain the mechanisms of resolution of CSDH.
According to Nakamura et al.7), the decreased fibrinolytic activity of the hematoma and its capsule might have caused spontaneous resolution. Kawano and Suzuki6) investigated the possibility that presence of smooth muscle cells in the outer membrane of hematoma might play a role in the resolution of CSDH. Glover and Labadie1) demonstrated a reduced rate of membrane formation in an animal model with corticosteroid treatment in which the effect of dexamethasone was thought to be anti-inflammatory or antiangiogenic3).
Several non-operative treatments have been described, including observation only, mannitol and ACE inhibitors or corticosteroids, however justification for treatment using ACE inhibitors or steroids has mainly been theoretical, and further research is clearly warranted11). In a recent study, Kageyama et al.5) suggested that Tranexamic acid might simultaneously inhibit the fibrinolytic and inflammatory (kinin-kallikrein) systems, which might consequently lead to resolution of CSDH. In our patient, we prescribed only anticonvulsant (valproate sodium) without other medication.
Some case reports on CT characteristics of spontaneous resolution of chronic subdural hematoma showed that the hematoma density becomes low with decreasing size4789). Nakamura et al.7) reported that every CSDH that resolved without surgery showed low density on follow-up CT and these authors also indicated that the fibrinolytic activity of low density hematomas decreased with regression of the thickness of the cavity.
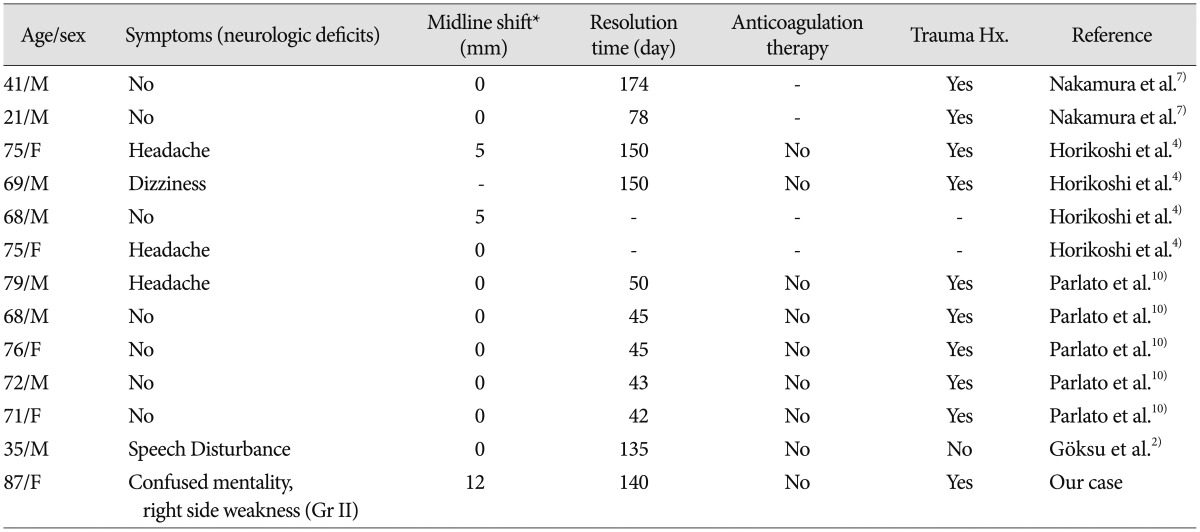
In the previously reported cases, radiologic characteristics of spontaneously resolved CSDH were small size of subdural hematoma, low or iso density of hematoma7), and absence of mid-line shifting or severe mass effect4), and its clinical characteristics were asymptomatic and mild transient headache410). The radiologic and clinical characteristics of our case are completely different from those of the previously reported cases. In our case, the subdural hematomas were large and the midline shifting was more than 12 mm. In addition, the patient showed severe hemiparesis clinically (Table 1).
CONCLUSION
This is a previously unreported rare case of spontaneous resolution of a large CSDH which required surgical decompression with hemiparesis and severe midline shift. Surgical treatment is still the gold standard and the first option in large CSDH with ventricular compression with mid-line shift having a distinct neurologic deficit. The possibility of conservative treatment is not indicated, however, there is probably another chance of spontaneous recovery as in our case. Persistent and close follow up of the patient is required in such CSDH cases.
 XML Download
XML Download