

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As of the year 2007, trauma was the fifth leading cause of death in all age groups and the ninth leading cause of death those older than 65 years in America. Head injury is the most common fatal organ system injury2). Multiple previous studies have suggested that intracerebral changes and atrophy in the elderly makes this population more susceptible to injury. These changes induce additional bleeding and intracranial swelling.
Long-term oral anticoagulation with warfarin or antiplatelet (aspirin, clopidogrel, and cilostazol) therapy has been used with increasing frequency, especially in the elderly, in order to prevent venous thromboembolism and subsequent pulmonary embolism, clot formation in patients with atrial fibrillation and mechanical heart valves, and coronary thrombosis in patients with atherosclerotic disease and those with coronary artery stents. Historically, these patients are at increased risk of morbidity and mortality from expansion of intracranial hemorrhage (ICH) due to the use of preinjury anticoagulation agents or antiplatelet agents 1367). Hence, the authors conducted a single-center retrospective case-control study to evaluate risk factors associated with outcome.
MATERIALS AND METHODS
Patients who underwent craniotomy or craniectomy for acute cases of subdural hematoma, epidural hematoma, or intracerebral hemorrhage between January 2005 and December 2014 were included. All of the patients were from a single institute. According to computed tomographic (CT) results, all of the patients had confirmed acute hemorrhage, including acute intracerebral, subdural, and epidural hemorrhages. Patients were considered as anticoagulated if they were taking warfarin, low-molecular-weight heparin, aspirin, nonsteroidal anti-inflammatory agents, clopidogrel, dipyridamole, pentoxifylline, or naproxen. The control group, which consisted of patients with intracranial injury as defined earlier but without any form of anticoagulation, were matched for mechanism and severity of injury. The number of patients in the control group was set to equal the size of the anticoagulated group.
Of the patients, 24 with intracranial injuries were identified to receive prehospital anticoagulation. For comparison, a control group consisting 26 patients with head injury but who were not taking any prehospital anticoagulant or antiplatelet agents were randomly selected based on the hospital records in the same period.
According to the classification by the Committee on Trauma of the American College of Surgeon, high-energy trauma refers to penetrating trauma, trauma from motorcycle crashes, and trauma from falling down from a height of more than 1 m. Meanwhile, low-energy trauma refers to trauma from slipping down and falling down from a height of lower than 1 m.
Statistical analysis was performed to identify differences in age, sex, preoperative Glasgow Coma Scale (GCS) score, Glasgow Outcome Scale (GOS) score, length of hospital stay, preoperative transfusion, intraoperative transfusion, postoperative transfusion, initial INR, initial platelet count, duration of intensive care unit (ICU) stay, length of hospital stay, and postoperative bleeding between the group who had and that who had not received antiplatelet agents or anticoagulants. Postoperative bleeding included postoperative epidural hematoma, postoperative subdural hematoma, and postoperative ICH, all were confirmed by performing an immediate postoperative CT examination within 1 hour after operation.
All of the patients had aggressive transfusion to resolve the abnormality in the prothrombin time-international normalized ratio PT-INR and platelet count.
We also performed statistical analysis to identify outcome factors such as neurological outcome, GOS score, and factors attribute to the merge of postoperative acute bleeding. To make statistical analysis easier, GOS scores of 4 and 5 were defined as favorable neurological outcomes, and GOS scores of 1, 2, and 3 were defined as unfavorable neurological outcomes.
Data were statistically analyzed by using the Student t-test, Wilcoxon rank sum test, chi-square test, or Fisher exact test, as appropriate
RESULTS
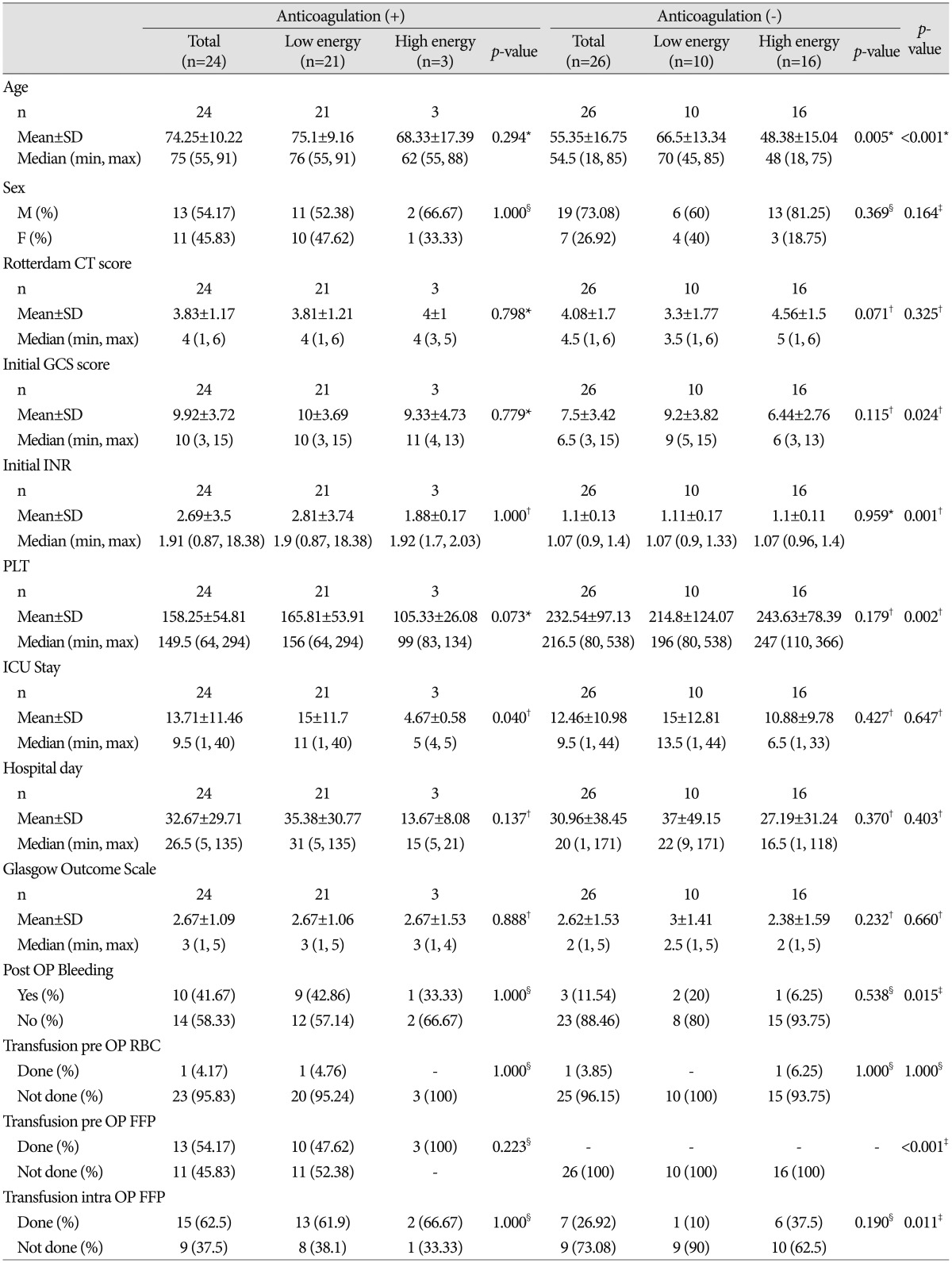
Data from a consecutive series of 50 patients were analyzed (Table 1). Of the patients, 24 were given anticoagulants, 7 had atrial fibrillation, 6 underwent operation for valvular heart disease, 4 had angina, 1 had pulmonary thromboembolism, 2 had hypertension, and 7 had a history of cerebral infarction. One patient had both atrial fibrillation and cerebral infarction, another had both angina and valvular heart disease, and one had angina and cerebral infarction.
Among the patients in the preinjury anticoagulated group, 13 were men and 11 were women, with a mean age of the patients was 74.25±10.22 years (range, 55-91 years). Among the patients without anticoagulation, 19 were men and 7 were women, with a mean age of 55.35±16.75 years (range, 18-85 years). The age difference between the two groups was statistically significant (p<0.001).
In general, among the patients who received preinjury anticoagulation or antiplatelet agents, 3 had high-energy trauma and 21 had low-energy trauma. However, in the non-anticoagulated group, 16 had high-energy trauma and 10 had low-energy trauma.
The initial Prothrombin Time-International Normalized Ratio was 2.69±3.5 (range, 0.87-18.38) in the anticoagulated group. Of those patients who did not received any anticoagulation, the mean PT-INR was 1.1±0.13 (p=0.001).
The initial platelet count was 158.25±54.81 (range, 130-400 ×103/µL) in the anticoagulated group and 232.54±97.13 (range, 80-538) in the non-anticoagulated group (p=0.002). The lengths of ICU stay were 13.71±11.46 days (range, 1-40 days) and 12.46±10.98 days (range, 1-44 days), respectively (p=0.647). The lengths of hospital stay was 32.67±29.71 days (range, 5-135 days) and 30.96±38.45 days (range, 1-171 days), respectively (p=0.403).
The mean initial GCS score was 9.92±3.72 (range, 3-15) in the anticoagulated group and 7.5±3.42 (range, 3-15) in the non-anticoagulated group (p=0.024). The mean GOS scores were 2.69±1.09 and 2.62±1.53, respectively (p=0.660).
In terms of preoperative, intraoperative, and postoperative transfusions, the antithrombotic group received more transfusions of fresh frozen plasma preoperatively. In the preinjury anticoagulated group, 13 patients (54.17%) received transfusion of fresh frozen plasma preoperatively, whereas none received such transfusions in the non-anticoagulated group. In transfusion of red blood cells or platelet concentrates, no significant difference was found between the preinjury anticoagulated and non-anticoagulated groups. Postoperative bleeding was observed in 10 patients (41.67%) in the preinjury anticoagulated group and in 3 patients (11.54%) in the anticoagulated group (p=0.015).
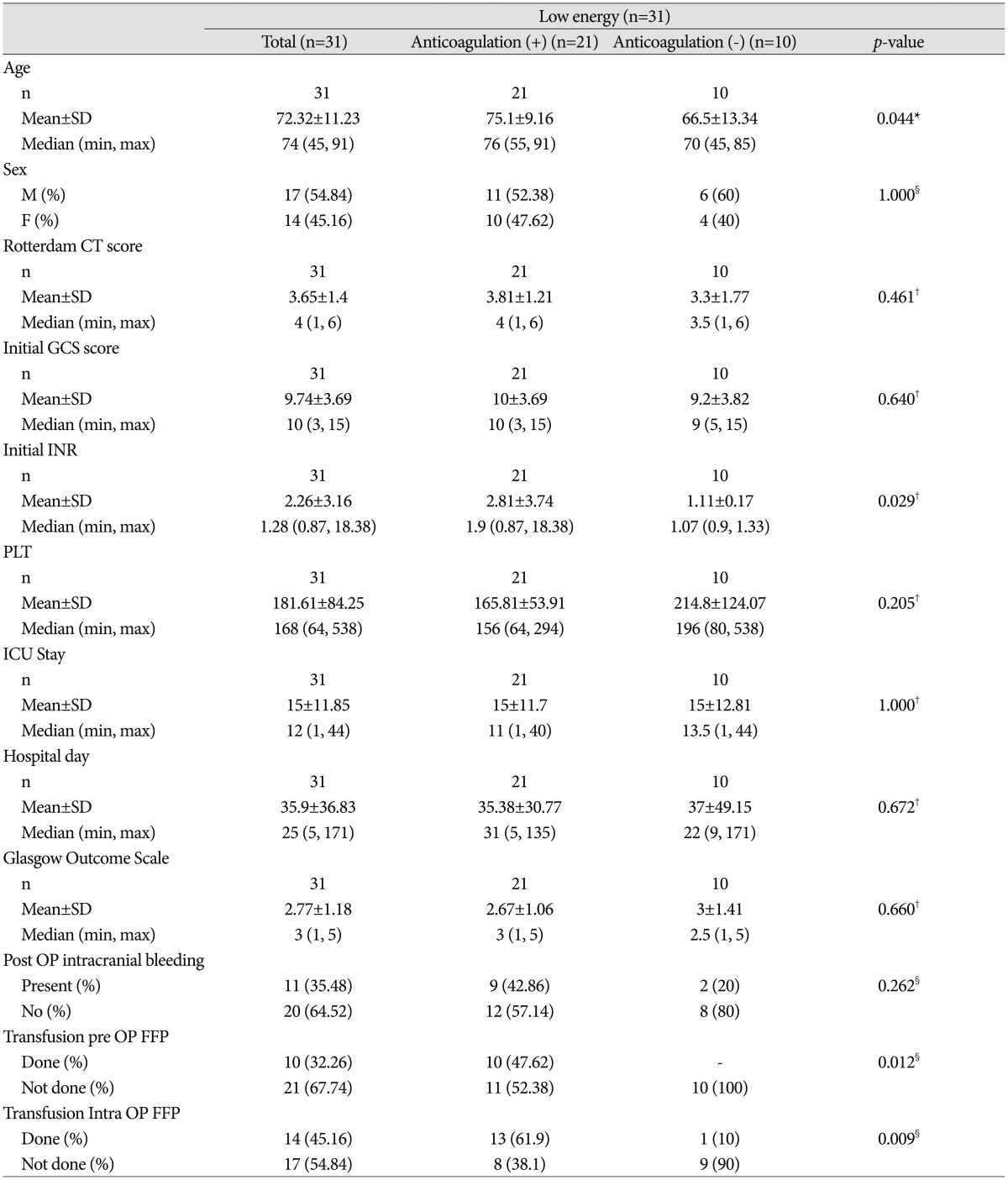
Comparative analysis of patients with low-energy trauma only (Table 2)
Among the patients in the preinjury anticoagulated group with low-energy trauma, 11 were men and 10 were women, with a mean age of 75.10±9.16 years (range, 55-91 years). Meanwhile, among the patients in the non-anticoagulated group with low-energy trauma only, 6 were men and 4 were women, with a mean age of 66.5±13.34 years (range, 45-85 years; p=0.044).
The initial PT-INR was 2.81±3.74 (range, 0.87-18.38) in the preinjury anticoagulated group with low-energy trauma and 1.11±0.17 (range, 0.9-1.33) in the non-anticoagulated group with low-energy trauma (p=0.029). The initial GCS scores were 10±3.69 (range, 3-15) and 9.2±3.82 (range, 5-15 years), respectively (p=0.640). The mean GOS scores were 2.67±1.06 and 3±1.41, respectively
(p=0.660).
Postoperative bleeding was observed in 9 patients (42.86) in the preinjury anticoagulated group with low-energy trauma and in 2 patients (20%) in the non-anticoagulated group with low-energy trauma (p=0.262).
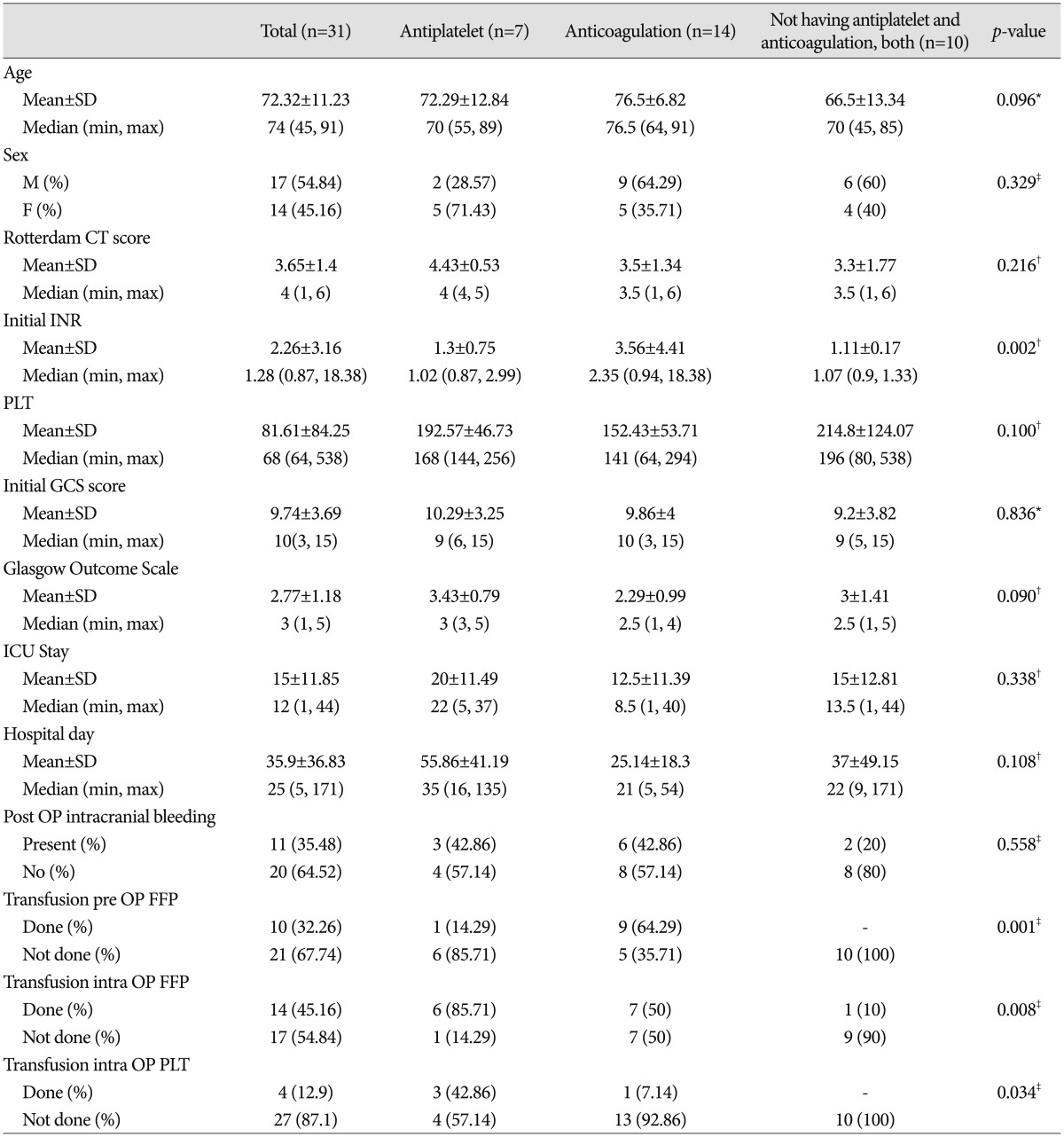
The effect of the preinjury anticoagulation and antiplatelet medications (Table 3, 4)
The antiplatelet medications such as aspirin, clopidogrel and cilostazol, and the anticoagulation medications such as warfarin and heparin have different effect. So we conduct comparative analysis to find out differences between the group of preinjury antiplatelet medication, the group of preinjury anticoagulation medication, and the group not having any medication in low energy trauma patients.
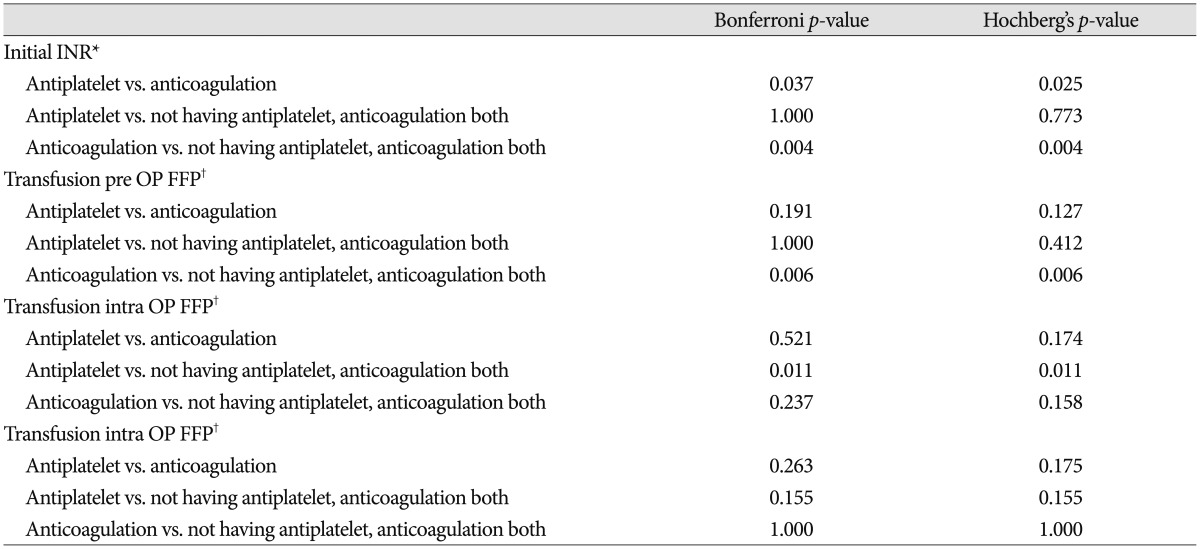
Consequently we could find significant differences in the initial INR, pre OP FFP transfusion, intra OP FFP transfusion and intra OP platelet medication between three groups. And other factors, such as age, sex, Rotterdam CT score, initial platelet count, initial GCS score, GOS score, post OP intracranial bleeding, hospital stay and ICU stay, showed no significant differences. To correct type I error emerged by using the Bonferroni and the Hochberg's method, we could find out that initial INR was higher in preinjury anticoagulation medication group compared with the group not having any antiplatelet and anticoagulation medication (p=0.04), have significantly higher rate of preoperative FFP transfusion and in anticoagulation group compared with the group not having any antiplatelet and anticoagulation medication (p=0.060).
Analysis to determine unfavorable outcomes (Table 5,6,7,8)
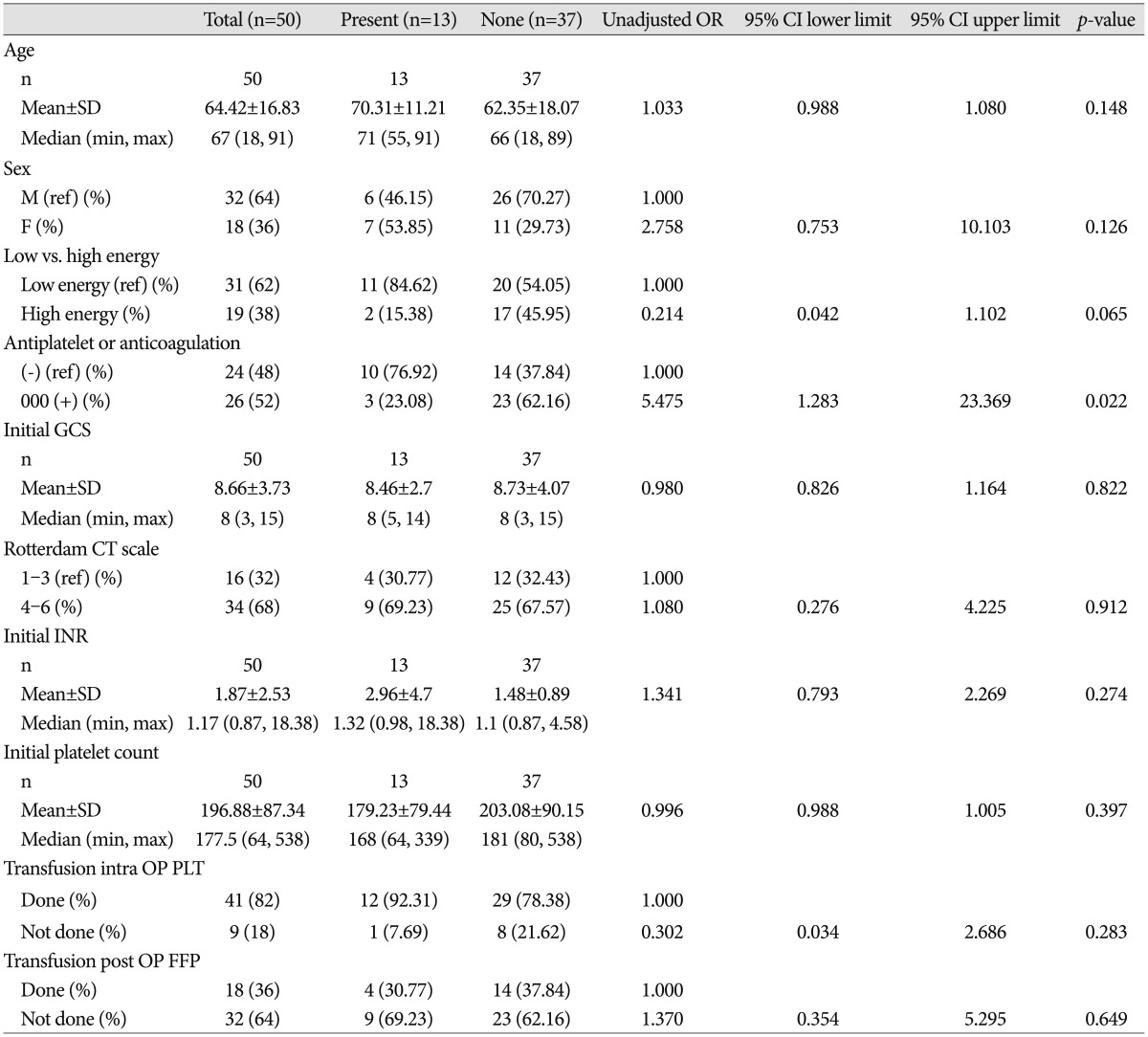
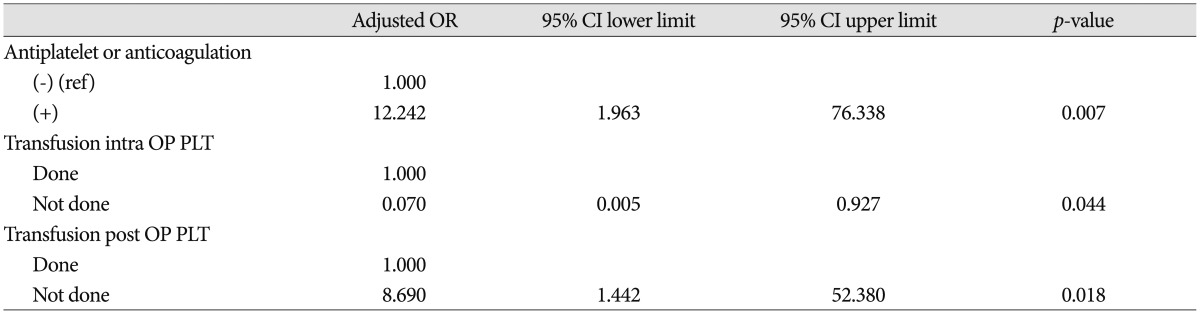
We performed a logistic regression analysis to determine the contributing factors to postoperative bleeding (Table 5). In a multifactorial analysis, to control for multicolinearity, we performed stepwise selection and created a final model, with variables considered significant at a 5% significance level (Table 6). In conclusion, the significant contributing factors to postoperative bleeding were preinjury use of anticoagulation agents [adjusted odds ratio (OR), 12.242; p=0.0070], transfusion of intraoperative platelet concentrates (adjusted OR, 0.070; p=0.044), and transfusion of postoperative platelet concentrates (adjusted OR, 8.690; p=0.018).
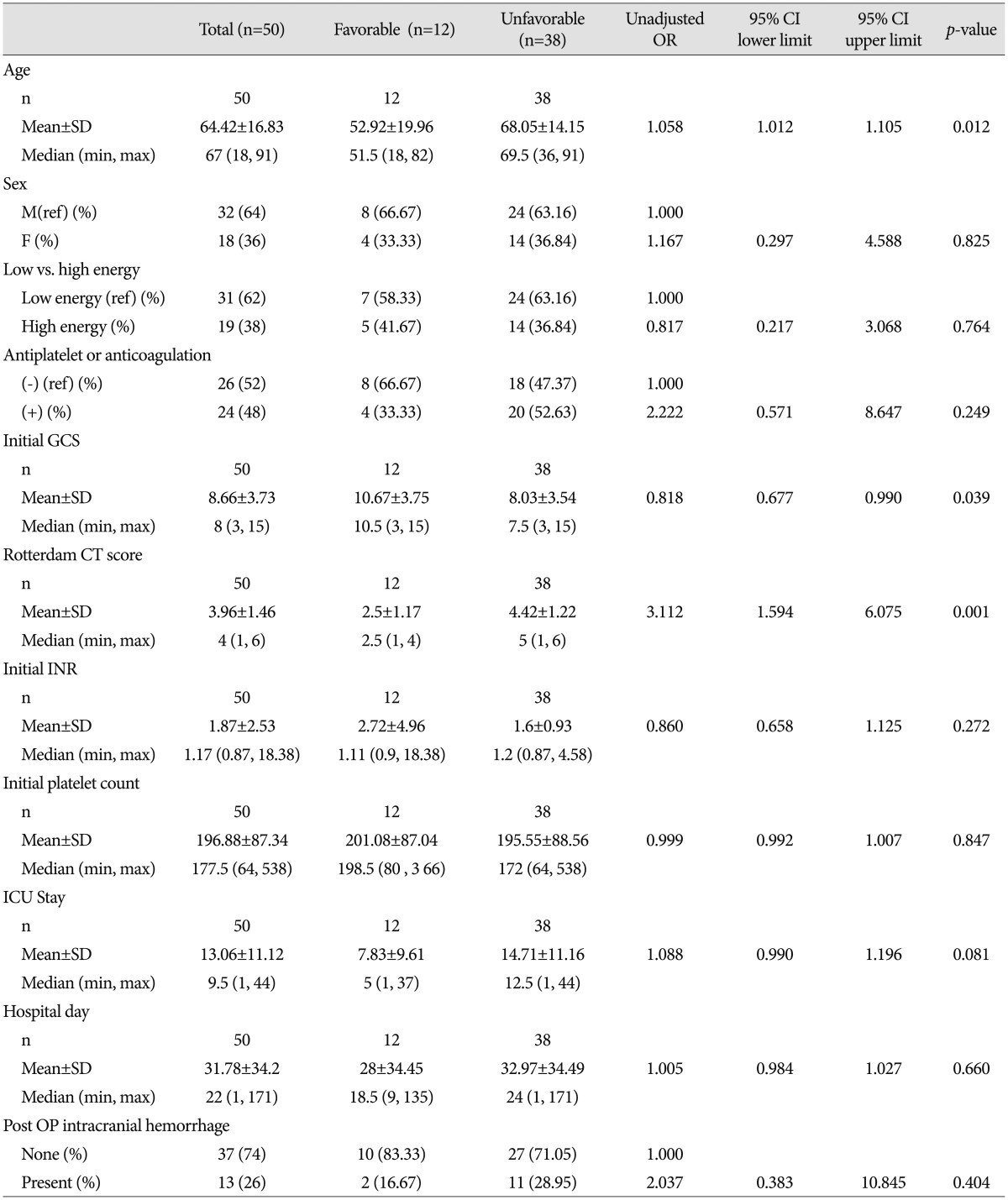
We performed a logistic regression analysis to determine contributing factors to GOS score (Table 7). In a multifactorial analysis, to control for multicolinearity, we performed stepwise selection and created a final model, with variables considered significant at a 5% significance level (Table 8). The contributing factors to unfavorable outcome were age (adjusted OR, 1.073; p=0.039) and Rotterdam scale score for CT scans (adjusted OR, 3.123; p=0.0020), at a significance level of 5%.
DISCUSSION
In this study, we conducted a retrospective study of a consecutive series of 50 patients who underwent craniotomy or craniectomy under general anesthesia. As age increases, the risk of coronary heart disease, valvular heart disease, or cerebral infarction also increases. Patients with such diseases require long-term oral anticoagulation4). Our data show that the patients in the anticoagulated group were older than those in the non-anticoagulated group.
Mina et al.8) evaluated 380 anticoagulated patients admitted to trauma service centers in their hospital from January 1997 to December 1998. They compared the results with those from 37 patients identified as having similar intracranial injuries but who were not anticoagulated. Preinjury anticoagulation therapy contributes significantly to the mortality from intracranial head injuries, with a fourfold to fivefold higher risk than without anticoagulation. But they didn't evaluated the efficacy of reversing anticoagulation effect8). Stein et al.9) reviewed fall-related injuries in anticoagulated stroke patients during inpatient rehabilitation and concluded that the risk of minor injury did not differ between anticoagulated and non-anticoagulated patients. And the risk of hemorrhagic injuries caused by falls among anticoagulated stroke patient in that setting was low9).
Contrary to suggestions that the use of antiplatelet or anticoagulant medication might increase the rate of poor clinical outcomes, our study showed no neurological differences in GOS score in the patients with low-energy trauma only. And it may be contributed by our best management for all the patient.
Clinical factors associated with poor outcomes
Preinjury anticoagulation therapy has been revealed to predict the occurrence of postoperative bleeding (adjusted OR, 12.242; p=0.0070). Evaluating brain conditions on initial brain CT by using the Rotterdam scale for CT scans has been revealed to predict prognosis of patients with traumatic brain injury. Huang et al.5) evaluated 127 patients from January 2007 to December 2008 retrospectively and find that higher Rotterdam CT scores were accompanied by higher rates of poor prognosis. In our study, Rotterdam scale scores for CT scans had proven to predict poor neurological outcomes in terms of GOS score. Thus, when patients with traumatic brain injury arrive at the emergency department, CT must be performed immediately in order to evaluate brain condition and predict patient outcome.
Age was a statistically significant predictor of neurological outcome. Thus, older patients require more careful management.
Limitations of the study
The present study had a retrospective design, which typically produces less accurate results than those with a prospective, randomized, multicenter design. And there were only small number of patients in the high-energy trauma group, especially preinjury anticoagulated patients.
CONCLUSION
Preinjury anticoagulation therapy contributed significantly to the occurrence of postoperative bleeding. However, preinjury anticoagulation therapy in the patients with low-energy trauma did not contribute to the poor clinical outcomes.
Careful attention should be given to older patients and severity of hemorrhage on initial brain CT because these factors predict poor outcomes. In particular, low Rotterdam scale scores contribute significantly to poor neurological outcomes, with a threefold higher risk than high Rotterdam scale scores.

 XML Download
XML Download