

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The cervicothoracic junction (CTJ) has anatomical and clinical peculiarities, as a reversal of lordosis to kyphosis occurs at this location. Although CTJ pathology is infrequent, most CTJ lesions affect the anterior column, leading to instability and spinal cord compression with a high rate of neurological compromise17). The anterior approach enables direct decompression by removing the pathology and provides efficient stabilization without damaging the posterior element, but anterior surgical approach to the CTJ is still challenging due to the anatomical structure and complex regional biomechanics11). Although several methods are available to help the spine surgeon decide whether do perform a manubriotomy, some remain controversial247816). We report on the technical feasibility and limitations of the transmanubrial approach for CTJ lesions and emphasize the advantage of bisecting the upper part of the manubrium in an inverted Y-shape.
MATERIALS AND METHODS
Patient population and evaluation
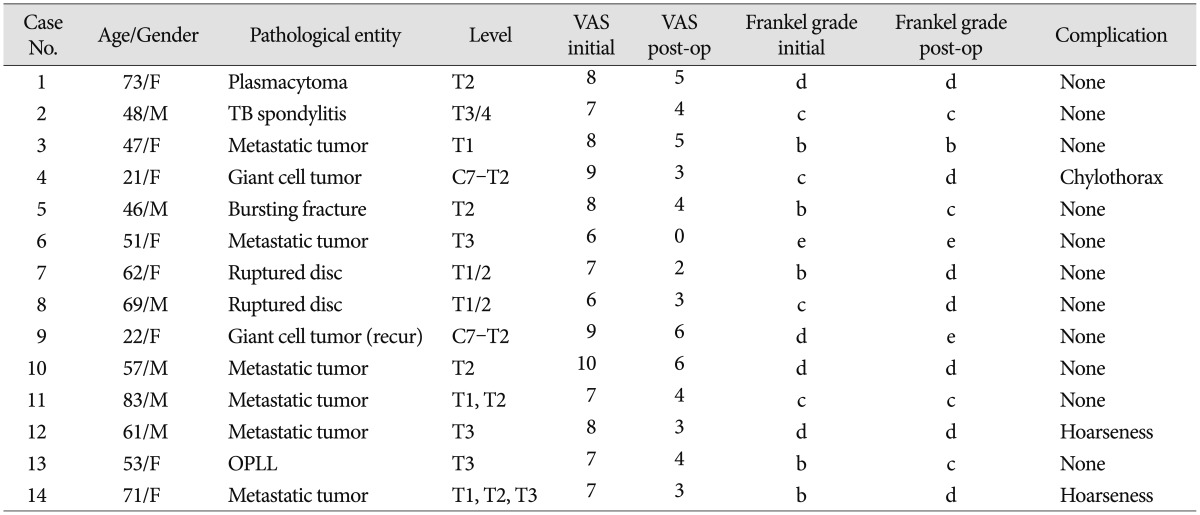
A series of 13 patients who underwent the manubrium splitting method for 14 CTJ lesions between April 2005 and December 2014 in a single institution were enrolled in this study. The patients had disabling symptoms caused by lesions between C7 and T3 with cord compression. The decision to surgically treat a CTJ metastatic lesion was made, when the patient was expected to survive >6 months, and the patient had a single unstable lesion on the spinal column with a neural compression. The following data were collected retrospectively : age, sex, lesion level, pathological entity, preoperative and postoperative neurological status, and complication. Pain score was measured by Visual analogue scale (VAS), preoperatively and postoperatively 2 weeks that was enough periods for resolution of operation site pain. Frankel scores were assigned to assess neurological status. The mean follow-up duration was 1.8 years.
Preoperative evaluation using magnetic resonance imaging for surgical accessibility
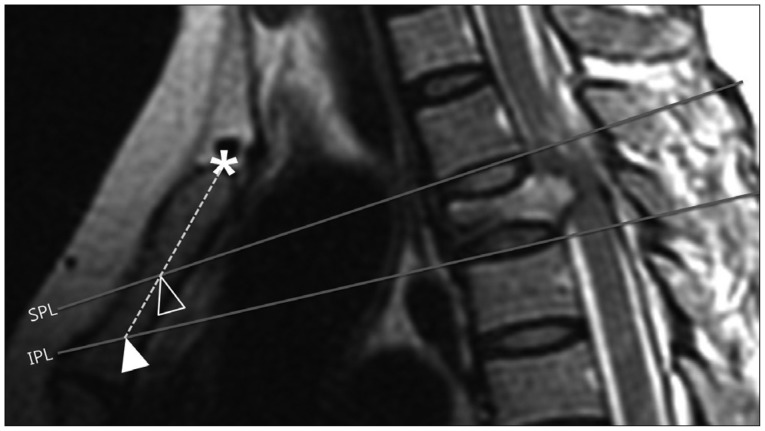
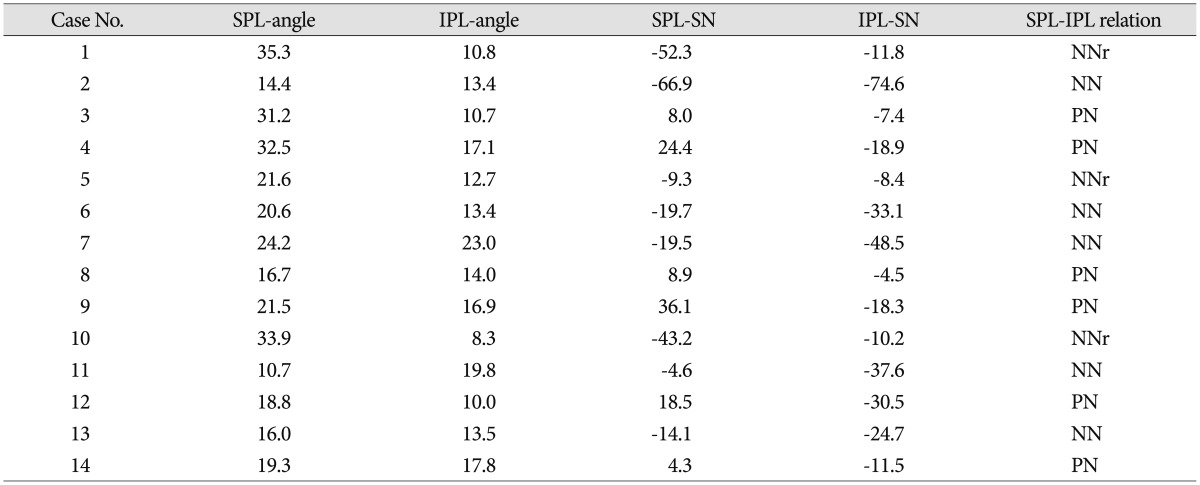
Preoperative MRI was used to evaluate the feasibility of the transmanubrial approach. In this study, MR imaging used rather than CT scanning, because MR imaging have better visualization of soft tissue structures including great vessels by flow void effect as well as osseous structures. Two lines were drawn from the spinal lesion to the sternum on a mid-sagittal MRI. The superior parallel line (SPL) was defined as a straight line passing through and parallel to the inferior plateau of the superior healthy vertebrae. The inferior parallel line (IPL) was defined as a straight line to the superior plateau of the inferior healthy vertebrae. The angles that met at the SPL and IPL were the SPL-angle and IPL-angle for each horizontal plane. The distances between the sternal notch to the SPL and IPL on the longitudinal axis of the sternum were measured. The value of a line placed superior to the sternal notch was positive and that for a line place inferior was negative (Fig. 1). If the both of SPL-sternal notch and IPL-sternal notch negative, a manubriotomy is inevitable. If the SPL passes through the great vessel or the heart deeply, the lesion considered to be approached by midline transmanubrial approach. If only the IPL is below the sternal notch, a manubriotomy is relatively indicated.
Operation method and technical considerations
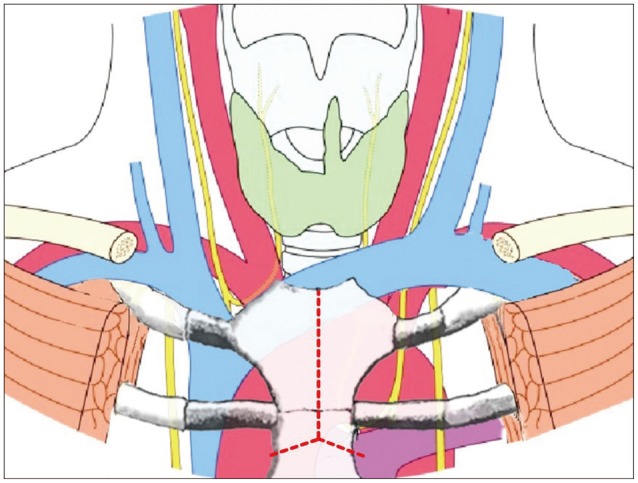
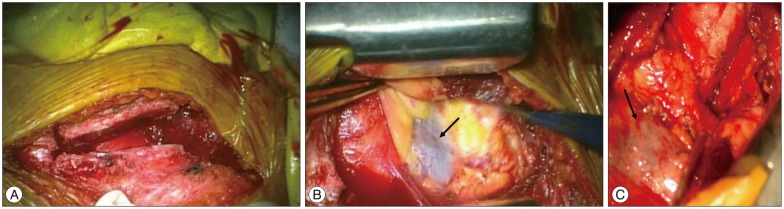
The patient was placed in a supine position under general anesthesia with a roll pad on the posterior of the back at the axis of spine. Thus, both shoulders extended the posture, which spread bisected the manubrium well. After routine surgical field preparation, an extended curvilinear incision was made from the cervical to the manubriosternal junction. The manubriotomy was performed in an inverted Y-shape with an oscillating saw after finger dissection of the posterior surface of the manubrium to avoid the injury to the innominate vein, which is the most superficial mediastinal vascular structure. The manubrium was bisected at the level of second intercostal space, which was palpable with a finger (Fig. 2). A strong short retractor was inserted between the bisected manubrium with care of the innominate vein crossing superficial to the arteries. For the approach through the soft tissue to anterior aspect of vertebral column, we performed using similar compartmental dissection to that used in the usual anterior cervical approach. Identifying the vertebral level might be difficult because the fluoroscopic image was obscured by the shoulder. Direct observing the anterior surface of the vertebral body is helpful after peeling off the anterior longitudinal ligament especially in metastatic infection cases. The great vessels can be retracted gently downward during the standard discectomy and corpectomy using a chisel and high-speed drill. However, extreme care must be taken not too much retract which may lead disastrous tear of innominate vein. The anterior decompression and spinal column were reconstructed with a mesh cage filled with autologous bone or demineralized bone matrix. The manubrium was re-approximated using sternal wire (Fig. 3).
Illustrative case
Case 10
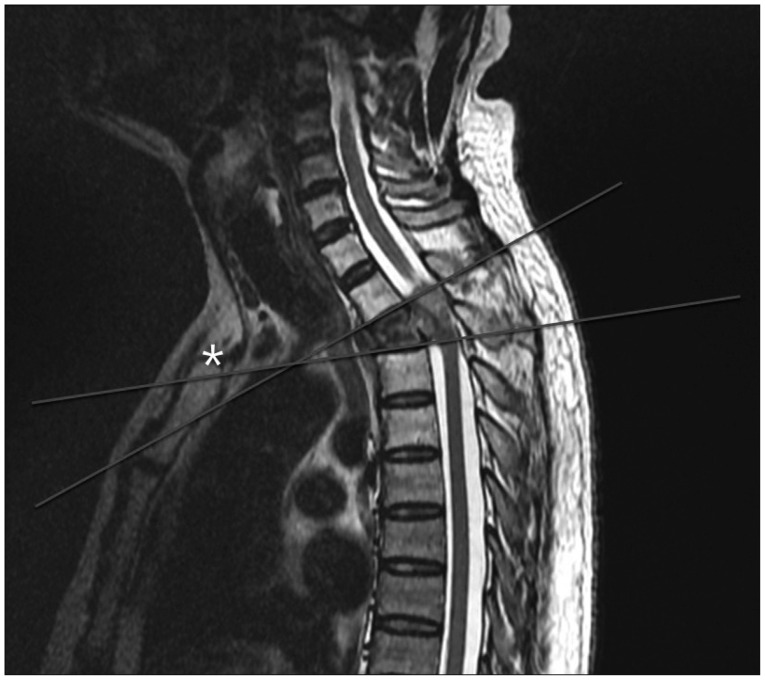
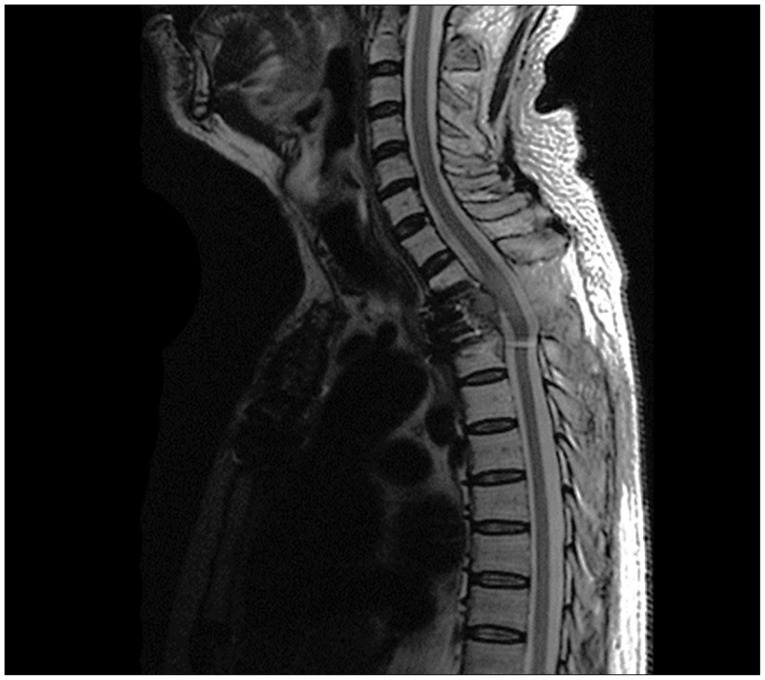
A 57-years-old male with hepatocellular carcinoma was referred from oncology due to impending paraplegia. He had complained of severe upper back pain with progressive weakness in the lower extremities for >3 months. A neurological examination revealed decreased senses of touch, pain, and changes in proprioception. Motor weakness of grade 3 with clonus and hypereflexia were present in the lower extremities. MRI of the cervicothoracic spine showed a fungating tumor within the T2 vertebral body extending to the pedicle and lamina. The SPL was -43.2 mm from the sternal notch and the IPL was -10.2 mm. The SPL-angle was 33.9°, and the IPL-angle was 8.3°. As the angle of SPL was steeper than IPL due to kyphotic deformity of lesion, two lines were crossing in the mediastinum (Fig. 4). This deformation makes difficulty of visualization and manipulation at the posterior superior corner of the T2 vertebrae during the operation, despite sufficient length of the manubriotomy. The main barriers were anterior lower corner of the T1 vertebra and great vein not the osseous window. This case well illustrates that the SPL is more important than the IPL. Decompression with corpectomy and reconstruction with a titanium mesh cage was done. The remaining tumor in the posterior column was removed through the second posterior approach 1 week later, and the pedicle screw was augmented. The patient's pain and neurological symptoms was improved markedly after surgery and postoperative MRI shows decompression of cord (Fig. 5).
RESULTS
The mean age of the patients was 55 years (range, 21-83 years). Eight patients were females. The majority of the patients had metastatic disease (six cases) : three primary tumors, two herniated discs, and one each tuberculous spondylitis, bursting fracture with syrinx formation, and ossification of the posterior longitudinal ligament. All patients presented with severe local pain, and 10 of the 13 patients showed signs of progressive myelopathy. Three patients each had involvement of T2, T3, and T1-2, two patients had C7-T2 involvement, and one each had T1-3, T3-4, and T1 involvement (Table 1). The mean SPL-angle was 22.6° (range, 10.7-35.3°) and the mean IPL-angle was 14.4° (range, 8.3-23.3°). The distances from the sternal notch to the SPL and IPL were -9.2 mm (range, -66.9-36.1 mm) and -24.3 mm (range, -4.5 to -74.6 mm). Distance from sternal notch to IPL was negative in all cases and distance from sternal notch to SPL was positive in six and negative in eight. Among the eight cases of both negative values, three cases showed more negative values in SPL than IPL and that mean two lines is crossing behind the sternum, which is shown in illustrated case (Table 2).
Neurological outcomes
Preoperative local pain and pain radiating to the chest or shoulder decreased in every case. The mean preoperative VAS score was 8 (range, 5-10), which improved to 4 (range, 0-6) postoperatively. Seven cases showed an increase in Frankel score postoperatively and the scores of seven cases remained unchanged (Table 1).
Complications
Three complications were detected for an overall rate of 21.4%. A thoracic duct injury occurred in a huge giant cell tumor case that extended to the first rib. The thoracic duct injury and chylothorax was managed with chest tube drainage and a lipid free diet for 2 weeks. Two patients with the lesion on T3 level developed temporary hoarseness, which resolved within several weeks after administering steroid. Most patients achieved bony fusion, except one with multi-drug resistant tuberculous spondylitis. One patient underwent revision surgery due to a recurred huge giant cell tumor, which was removed using the same approach. There was no nonunion or persistent pain at the bisected manubrium.
DISCUSSION
The anterior surgical approach to the CTJ is limited by the sternum, clavicle, and other vital structures, such as the trachea, esophagus, great vessels, thoracic duct, lung apex, and recurrent laryngeal nerves, which make the surgery treacherous6). The CTJ or upper thoracic spine causes more strain on the post-fusional segment postoperatively because of the transition area from a mobile, lordortic cervical to a rigid, kyphotic thoracic spine. Since the midline full sternotomy was described by Cauchoix and Binnet in 1957, various modified approaches for CTJ lesions have been tried1345781012131416).
According to Kaya et al.9) the approaches can be categorized into four groups of posterior, posterolateral, anterior, and anterolateral approaches. The posterior approach appears to be simple and familiar but is less logical because the majority of lesions are situated in anterior column. A laminectomy is inadequate or has a risk of neural damage for ventral decompression. Although the posterolateral approach improves visualization compared to that of the posterior approach, it is still limited to ventral access. The anterolateral thoracotomy introduced in 1960 assures a wide opening of the chest cavity. This approach to the CTJ includes clavicle resection or separation of the sternoclavicular joint and has a risk of nonunion. The anterior midline approach is the best option from the perspective of effective decompression and direct stabilization and the low morbidity rate15). The midline full sternotomy approach, which is commonly applied in cardiac surgery, provides a wide bony window but the lower extent of the surgical field at the CTJ would not be extended because the main barrier to the anterior vertebral aspect is the great vessels not the osseous window. A full sternotomy for a CTJ spinal lesion appears to have unnecessary exposure. The transmanubrial approach, which only bisects the upper part of the manubriosternum, allows sufficient exposure of the CTJ but the caudal limitation due to the innominate vein and aortic arch should be evaluated by careful preoperative planning. Kaya et al.9) suggested using the vertebral level as a landmark for the transmanubrial approach. They recommended the transmanubrial approach for T3, and a lateral transthoracic approach for areas below T3. Our results indicate that there is considerable variation in the sternal notch level and angle.
We applied two lines parallel to the vertebral body endplate near the lesion on preoperative MRI to determine the feasibility of manubriotomy. These angles had a wide range of value due to personal variation and kyphotic deformation from a pathological fracture of the lesion. If the SPL is lower than the sternal notch, a manubriotomy is inevitable. Moreover, if the two lines cross behind the sternum at the mediastinum, the difficulty of manipulation at the upper posterior part of the lesion is anticipated. If the SPL passes through deeper than heart apex, the lesion cannot be approached by midline transmanubrial approach. If only the IPL is below the sternal notch, a manubriotomy is relatively indicated. In this situation, a manubriotomy can be performed after careful evaluation of viewing angle and the level of IPL line on the sternum. Because the viewing angle can occasionally be obtained by corpectomy of lesion, the manubriotomy is not mandatory. If both lines are above the sternal notch, manubriotomy is not necessary and the suprasternal approach should be considered. The proposed indication was summarized Table 3.
The obstacles of anterior midline access to the CTJ can be classified by two categories. One is osseous structures, such as the manubrium, sternum and clavicle and the other is visceral structures, such as the innominate vein and aortic arch, trachea, esophagus, recurrent laryngeal nerve, etc. As the caudal extent of anterior spinal surface is mainly limited by the visceral structure, which lies at the first or second costosternal junction rather than osseous structure, an inverted Y-shape manubriotomy at the second intercostal space appears to be optimal. Performing the manubriotomy using the angle of the two parallel lines and the distance from sternal notch to the line at the axis of the sternum is more rational rather than deciding using the number of vertebrae.
CONCLUSION
The anterior approach for CTJ lesions is challenging but achieves favorable clinical outcomes by bisecting the transmanubrial approach. The decision to perform a manubriotomy for a CTJ lesion can be made by carefully evaluating the preoperative lesion regarding two parallel lines and the distance from the sternal notch. An inverted Y-shaped manubriotomy at the second intercostal space appears to be optimal for a variety of CTJ lesions.

 XML Download
XML Download