

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) with autologous bone graft and anterior plating has been the standard procedure for single level cervical disc disease121522). To reduce post-operative complications, such as post-operative iliac pain and dysphagia, the stand-alone cage was developed2341127). Compared to the traditional procedure, multiple studies have argued that the stand-alone cage produces more subsidence and local kyphosis at the index level, however no difference in clinical outcome has been proven246112127). Because of its advantages (convenience of use and decreased complications, as noted above) and less evidence of disadvantages relative to the standard procedure, the stand-alone cage is widely used for ACDF.
The Zero-Profile anchored spacer (Zero-P; Synthes GmbH, Oberdorf, Switzerland) is an instrument developed to integrate the stand-alone cage and the fixating screws. Using this instrument for ACDF has potential strengths compared with the anterior plating method. First, Zero-P could reduce the volume of the anterior plate, which might reduce post-operative dysphagia and simultaneously fix the cage strongly between the segments. Several published studies support this hypothesis without any significant disadvantage in clinical and radiographic results1678101416172021222526). However, most of the studies compared Zero-P with the anterior plate method alone. Only one published study has compared Zero-P with the stand-alone cage without the anterior plate system, and this study only presented the short-term outcome21).
Clarifying the efficacy of Zero-P compared with the stand-alone cage is important to the practice of spine surgery overall. Spine surgeons commonly use the stand-alone cage to avoid the discomfort of the anterior plate and autologous bone graft. However, if the Zero-P shows a superior outcome over the stand-alone cage and a similar outcome to the anterior plate system, this technique could be a good alternative. In this study, we followed patients for more than 2 years to compare radiographic and clinical outcomes of the Zero-P and the stand-alone polyetheretherketone (PEEK) cage (Cervios; Synthes GmbH, Oberdorf, Switzerland) packed with demineralized bone matrix (DBM; Musculoskeletal Transplant Foundation, Edison, NJ, USA).
Go to : 
MATERIALS AND METHODS
Patients
Total 121 patients underwent single-level ACDF for cervical disc herniation accompanied by radiculopathy or myelopathy between January 2011 and January 2013 in our hospital. Among them, we excluded the patients who had any history of 1) previous cervical spine surgery, 2) other cervical disease including ossification of posterior longitudinal ligament, 3) systemic infection or malignancy, and 4) a follow-up period shorter than 2 years. We finally reviewed 50 patients retrospectively.
All operations were performed by one neurosurgeon. Twenty-nine of these procedures were performed with the stand-alone PEEK cage (cage group) packed with DBM, and the other 21 were performed with Zero-P (Zero-P group), within the same period. All patients were performed ACDF under the same operation indication and the device used for the operation was selected randomly.
Operative techniques
A standard anterior Smith-Robinson approach was performed in both groups. The discectomy was performed with pituitary forceps after confirmation of the surgical level. The marginal areas of each vertebral body were prepared with a high speed drill and curettes. Subsequently, the posterior longitudinal ligament was removed, and neural decompression was confirmed. A stand-alone PEEK cage packed with DBM was inserted for the cage group, and Zero-P packed with the same DBM was inserted for the Zero-P group. Four screws were inserted for the Zero-P group under C-arm guidance. Then, the wound was closed in a layer-by-layer fashion after drainage insertion.
Radiographic evaluations
All patients were routinely examined with cervical spine plain X-ray images with an antero-posterior, lateral, both obliques, and excessive flexion and extension series. Additionally, the cases included pre-operative computed tomography (CT) or magnetic resonance imaging (MRI). All patients were followed with cervical spine plain X-ray images with antero-posterior and lateral views at the outpatient clinic. The follow-up time points were immediately post-operative, 3 months, 6 months, 12 months, and 24 months. We measured the Cobb angle of segmental area (Cobb-s) and Cobb angle of global cervical spine (Cobb-c) in the cervical spine plain X-ray lateral view to evaluate the aggravation of kyphosis (Fig. 1). Initially, we planned to evaluate bone fusion, but because of a lack of CT data (post-operative CT is not a standard procedure because of radiation hazard), we evaluated bone fusion through X-ray lateral view. Bone fusion was judged by 2 spine surgeons on radiographs by 1) less than 10 degree movement on lateral flexion/extension views, 2) presence of bridging trabecular bone between the endplates on anteroposterior and lateral views, 3) less than 50% radiolucency in the perimeter surrounding the cage, and 4) no evidence of pull out of the device. We compared the bone fusion rate of the each group on post-operative 3 months, 6 months, 12 months, and 24 months. The kappa coefficients for hinge status at each observation were 0.69, 0.71, 0.68, and 0.77, respectively. Kappa coefficients of 0.68-0.77 suggest good agreement among the observers. Also, we compared pre- and post-operative disc height (DH) and vertebral height (VH) in the plain X-ray images to evaluate the degree of subsidence to estimate the spinal alignment state indirectly. We measured the anterior-posterior length of the superior vertebrae at operation level in the X-ray18) and in the pre-operative CT scan or MRI, which demonstrate actual length (aAP). These data were used for the calculation of actual length of DH (aDH; DH×aAP/AP) and VH (aVH; VH×aAP/AP)11).
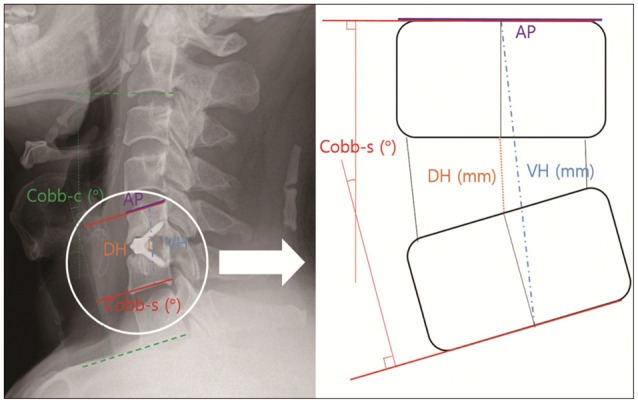 | Fig. 1Simple X-ray lateral view of patient operated with Zero-P anchored spacer. Cobb-c indicates the angle (°) between the lower margin of C2 and C7 vertebral bodies, Cobb-s indicates the angle (°) between upper margin of cranial vertebral body and the lower margin of caudal vertebral body of operated level, VH indicates the length (mm) between the midline of upper margin of cranial vertebral body and the lower margin of caudal vertebral body of operated level, DH indicates the length (mm) between the midline of upper and lower margin of disc space at operated level, and AP indicates the length (mm) of upper margin at the cranial vertebral body for operated level. Zero-P : Zero-Profile, VH : vertebral height, DH : disc height, AP : anterior-posterior.
|
Clinical outcomes
Clinical outcomes were evaluated with the neck disability index (NDI) and the visual analogue scale of the patients' necks (VASn) and arms (VASa). These indexes were checked pre-operatively and at 24 months post-operatively. The operation time and estimated blood loss (EBL) were also checked.
Statistical analysis
Statistical analyses were performed using the SPSS 21.0 statistical software (SPSS Inc., Chicago, IL, USA). The radiological and clinical values were expressed as means±standard deviations. The data were analyzed using the Mann-Whitney U test for the quantitative data and the chi-squared test for the qualitative data. A p-value<0.05 was considered statistically significant.
Go to :
RESULTS
Demographics
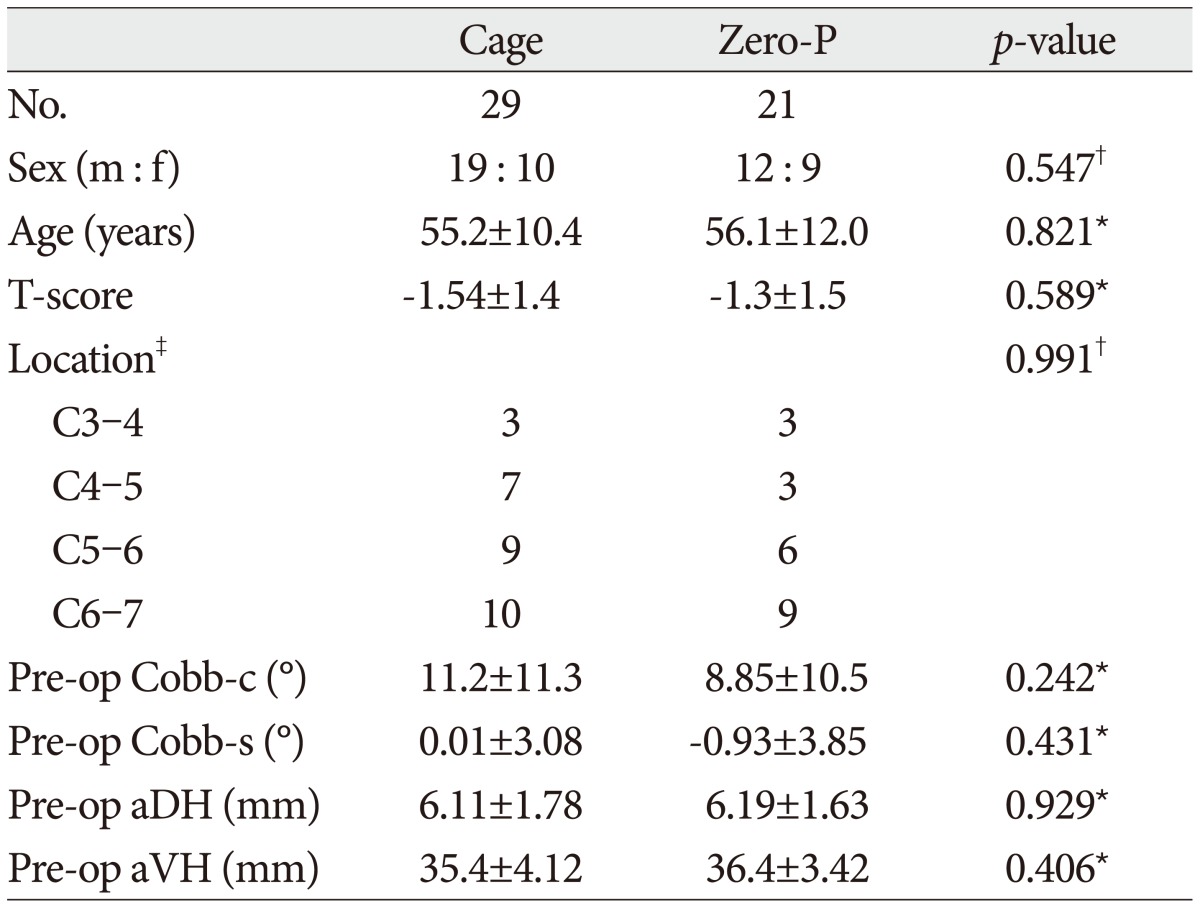
The number of patients in each group was 29 in the cage group and 21 in the Zero-P group. The age (p=0.821) and sex (p=0.547) were not significantly different between the two groups. The surgical level was evaluated as C6-7 or not, with no significant difference between the groups (p=0.991)21124). The pre-operative Cobb-c and the pre-operative Cobb-s were not statistically significant (p=0.242 and p=0.431, respectively). The aDH (p=0.929) and aVH (p=0.406) also did not differ significantly between groups. The data are shown in Table 1.
Clinical outcomes
Pre-operative NDI, VASn, and VASa showed no significant difference between the two groups (p>0.05). These results did not change after 24 months (p>0.05). Further, the group differences between pre-operative and 24 months post-operative were estimated, and the results showed no significant difference between the two groups (p>0.05). Finally, the average operation time (p=0.296) and the EBL (p=0.420) were not significantly different between the two groups. Details are shown in Table 2.
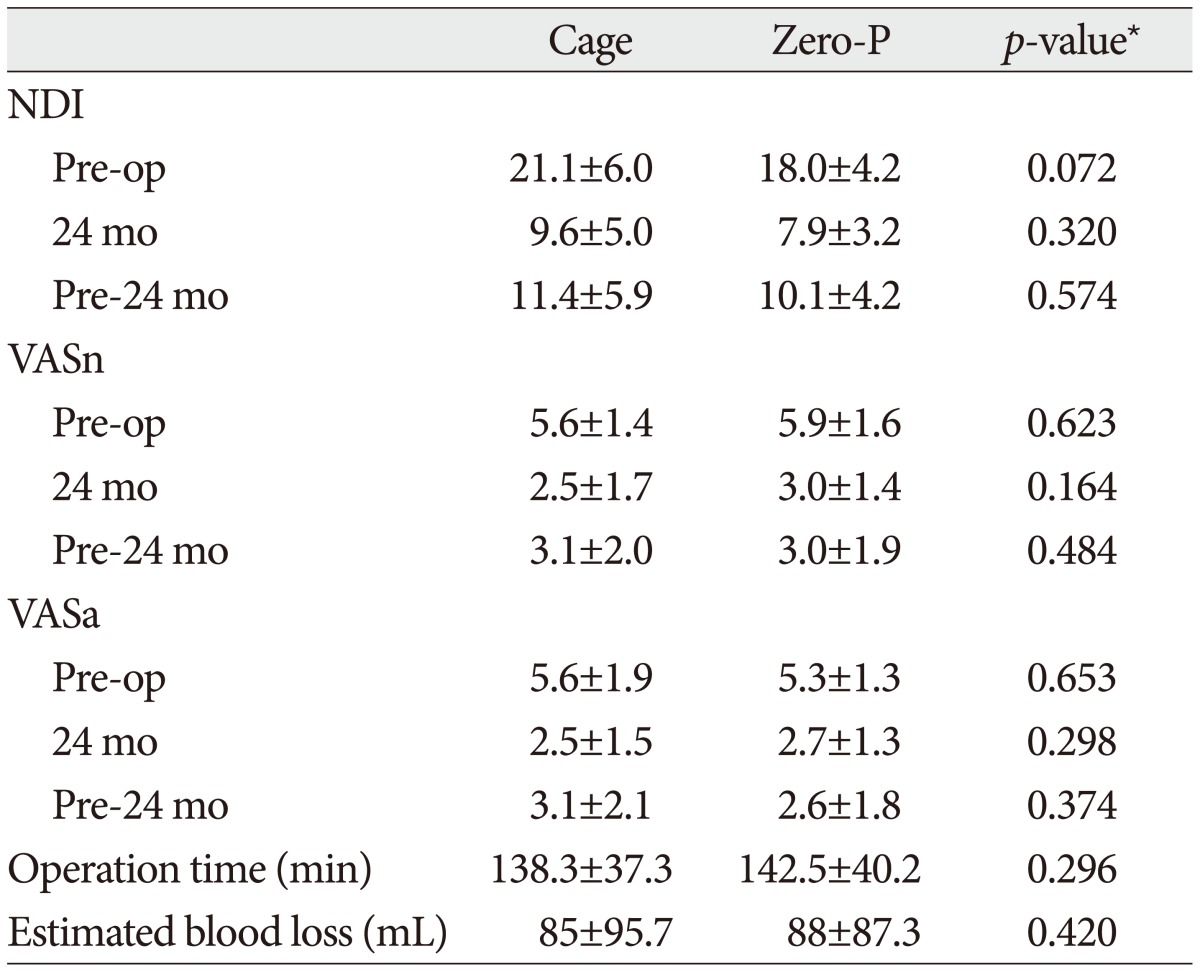
Table 2
Clinical parameters
dA-B=the difference between the value of A and B. For example, dPre-24 mo NDI means the difference between the value of pre-operative and post-operative 24 month NDI. *Mann-Whitney U test. Zero-P : Zero-Profile, NDI : neck disability index, VASn : visual analogue scale of the patients' necks, VASa : visual analogue scale of the patients' arms
![]()
Radiographic outcomes
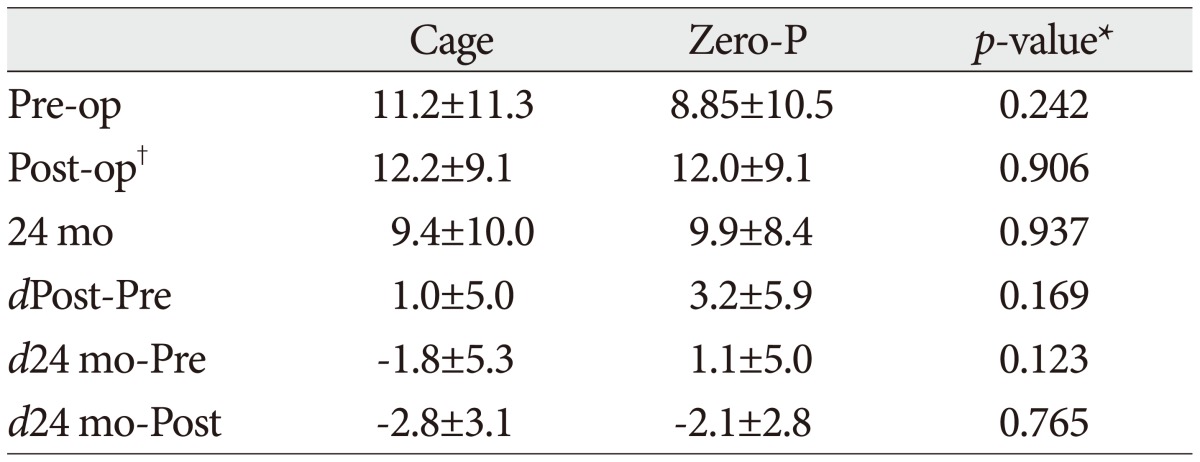
The Cobb-c scores at the immediate post-operative time point were 12.2±9.1 for the cage group and 12.0±9.1 for the Zero-P group (p=0.906). Both groups showed loss of lordosis in the 24 month follow-up X-ray without significant differences between the two groups (p=0.937). The difference between the immediate post-operative Cobb-c and pre-operative Cobb-c, post-operative 24-month and immediate post-operative, and difference cage group and -2.1±2.8 at the Zero-P group (p=0.765). Additional data are shown in Table 3.
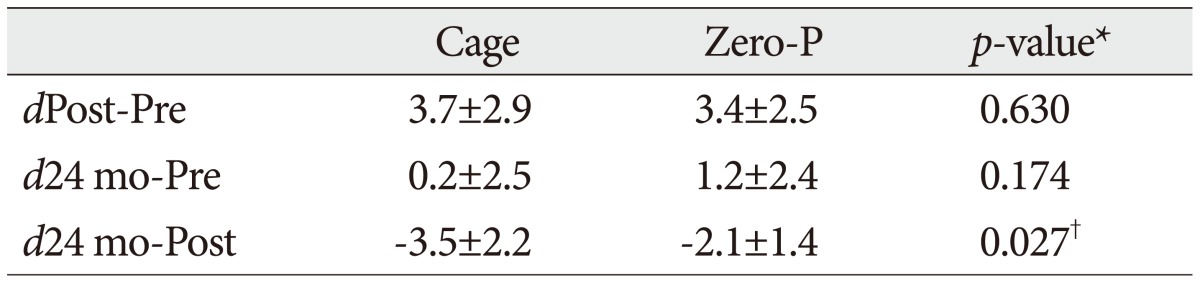
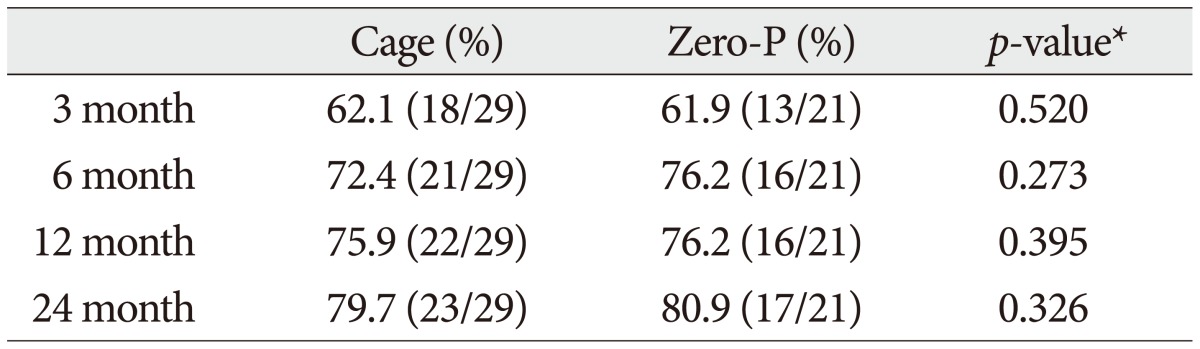
The Cobb-s immediately after the surgery was 3.7±2.8 for the cage group and 2.4±3.4 for the Zero-P group (p=0.221). These values worsened gradually, and the 24-month follow-up values were 0.2±2.5 and 0.3±3.2, respectively (p=0.812) (Fig. 2). The changes in Cobb-s between the immediately post-operative and pre-operative time points and between the 24-month post-operative and pre-operative time points were not significantly different between the groups (p>0.05). However, the difference between the 24-month post-operative and the immediately post-operative Cobb-s was significantly different between the two groups (p=0.027) (Table 4). Comparing the bone fusion rate, there were no statistical differences between two groups at any periods (p>0.05) (Table 5).
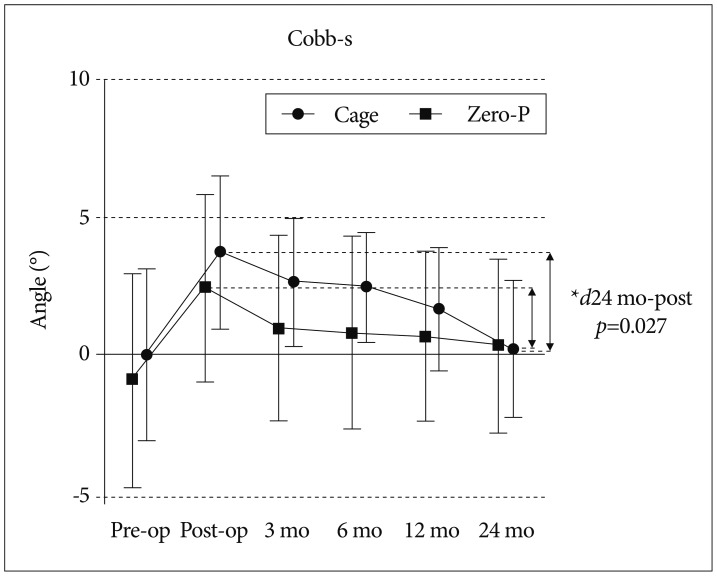 | Fig. 2Serial follow up graph for Cobb-s angle (°). The Cobb-s angle shows improvement after immediate post-op and declines as time pass for both group. Change after immediate post-op and post-op 24-month shows significant difference between two groups (*p=0.027), the Zero-P group has lesser decline. Zero-P : Zero-Profile.
|
The aDH was improved immediately after surgery for both groups; 8.1±1.3 in the cage group and 8.3±1.3 in the Zero-P group. The post-operative aDH of each group worsened to 6.5±1.5 and 7.1±1.5 at the 12 month follow-up, respectively (p=0.061). At the final follow-up, the two groups showed a significant difference (5.5±1.3 and 6.8±1.5, respectively, p=0.001), and the cage group was even worse than at the pre-operative evaluation. Compared to the immediately post-operative examination, aDH worsened over time for both groups. At the final follow-up, the differences between the immediately post-operative follow-up and 24 month post-operative aDH significantly different between the two groups, with the Zero-P group showing a better result (p=0.002) (Table 6, Fig. 3, 4).
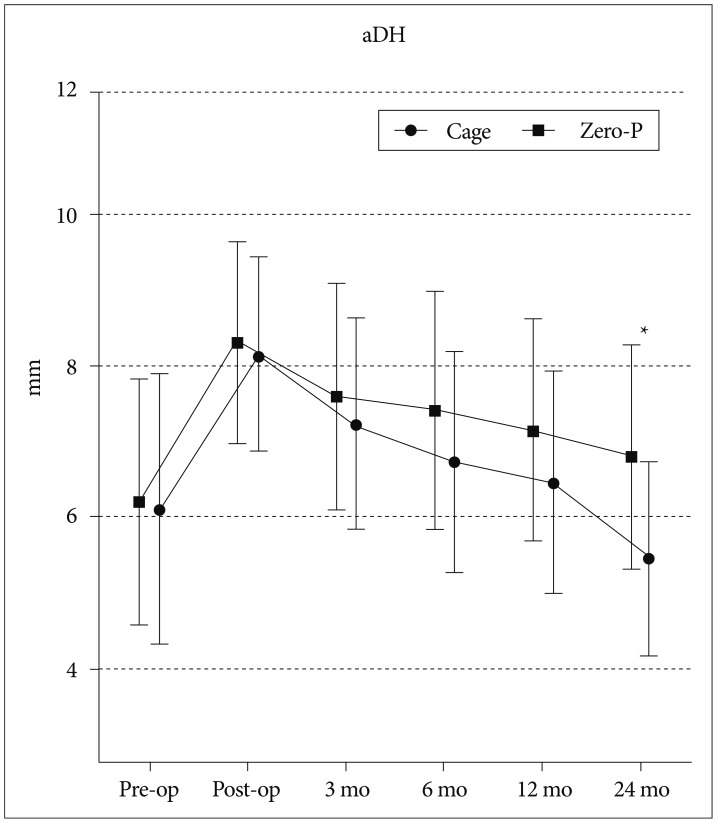 | Fig. 3Serial follow up graph for aDH. The aDH shows immediate improval after surgery but aggravates as follow up. At final follow up, cage group showed significantly shorter aDH than Zero-P group (*p=0.001). Zero-P : Zero-Profile, aVH : actual length of vertebral height.
|
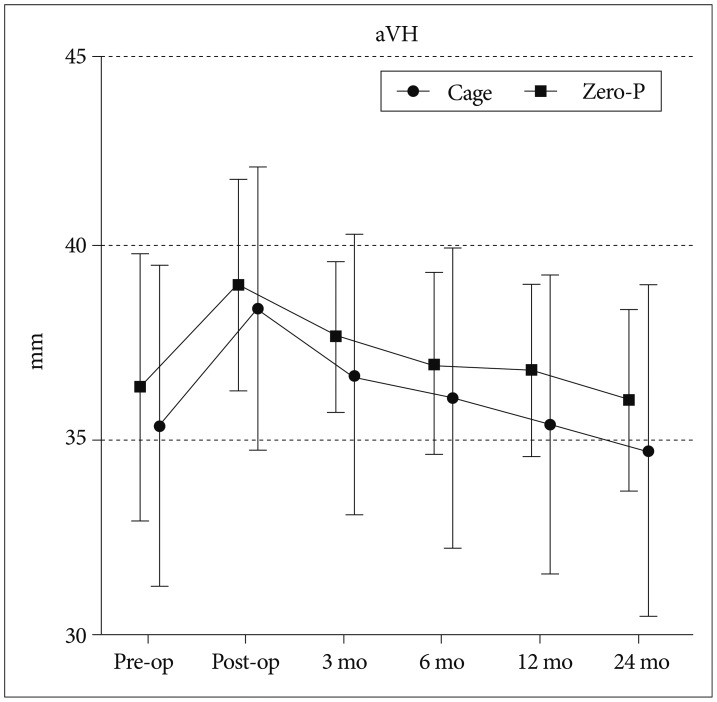
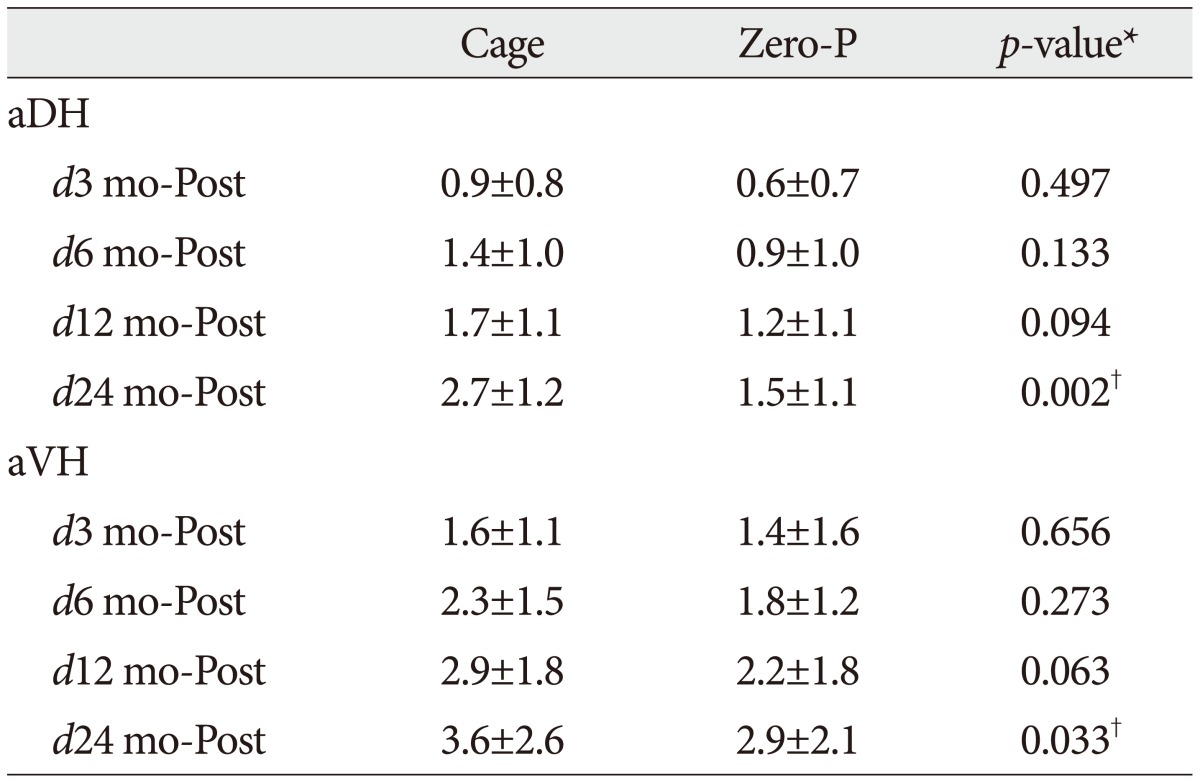
The aVH measure had a similar tendency to the aDH scores. The VH was also improved right after the surgery; 38.4±3.6 in the cage group and 39.0±2.7 in the Zero-P group (p=0.442). These scores also worsened over time : 35.4±3.8 and 36.8±2.2 at the 12-month follow-up (p=0.165), respectively, and 34.7±4.3 and 36.0±2.3 at the 24 month follow-up (p=0.070), respectively. The difference between the immediate post-operative time point and the later follow-up results revealed a gradual worsening. Similar to aDH, the gap between the two groups widened as time passed, and the results of the last follow-up (the difference between the immediate post-operative and 24 month post-operative follow-ups) showed significant differences between the two groups, with a better outcome for the Zero-P group (p=0.033) (Table 6).
Go to :
DISCUSSION
Cervical degenerative disease is defined as a chronic degenerative process of the cervical spine23). The category includes clinical syndromes such as radiculopathy or myelopathy, and sometimes requires surgical intervention23). ACDF is one of the most common surgical interventions performed by neurosurgeons. Overall complication rates reported for ACDF vary from 5% to 15% according to published studies513). ACDF with autologous bone graft and anterior plating has been the gold-standard operation for cervical degenerative spondylosis, including herniated nucleus pulposus121522). Because of problems associated with the operation, such as autologous bone graft subsidence, donor site pain, dysphagia due to anterior plate and screw failure, stand-alone cages were developed2341127). The Cervios cage is one of these devices; it is designed to provide a scaffold for bony fusion and stability. The apparatus also restores the height of the disc space24691127). According to recent studies, stand-alone cages have shown equally good clinical output as the previous method691921).
However, the stand-alone cages have issues of subsidence and local kyphosis at the index level2611). The kyphosis at the index level may aggravate the degenerative change in adjacent levels1011). Kim et al.11) reported that even though the subsidence does not affect short-term outcome, it may be associated with the acceleration of the degenerative change. 77% of the patients with kyphosis at the fused segment showed a degenerative change in a long-term study. To minimize these problems, the Zero-P was produced. This method reduces the volume of the anterior plate so that it can decrease dysphagia while maintaining the benefits of anterior cervical plating.
In this study, we compared the bone fusion rate of the both groups; it was not significantly different between the two groups. Then we compared the Cobb's angle of the whole cervical spine and the segmental area between the stand-alone cage group and the Zero-P group. The initial Cobb-c was not significantly different. The immediately post-operative Cobb-c was improved in both groups, showing no significant difference between the groups. The lordotic curve of both groups was improved temporarily, but it worsened as time passed. The 24 month post-operative Cobb-c of the cage group was even worse than the pre-operative Cobb-c, while the Zero-P group maintained a somewhat improved value compared the pre-operative Cobb-c value. However, the two groups were not statistically different.
When we compared the tendency of the Cobb-s between the two groups, it showed similar results to the Cobb-c : lordosis was improved temporarily and then gradually worsened. The difference between the 24 month post-operative and the immediately post-operative time points were significant, representing that the Zero-P group displayed significantly less aggravation of the segmental Cobb-s angle than the cage group. In some long-term studies, degenerative changes of adjacent levels were observed in 77% of the patients with kyphosis1011). Taking this into consideration, the restoration of the lordotic angle may be beneficial to prevent the aggravation of degenerative changes. In this aspect, Zero-P seems to better maintain the normal curvature of the cervical spine than the stand-alone cage.
From these results, we can suppose that if we follow the patients for a longer time or study a larger population, the global lordosis may also show a statistically significant value. As noted earlier, the kyphosis of the segmental area affects the degenerative change of the whole cervical spine according to several previous studies. In our study, even though the Cobb-s showed statistically similar results in both groups, the groups became more different as time passed. Combining these studies, a longer follow-up time may show a statistically significant result in the Cobb-s measure.
We measured aDH and aVH to evaluate the subsidence rate and post-operative spinal alignment for the groups. Both aDH and aVH showed similar results; the difference between the 24 month post-operative and the immediately post-operative examinations was significantly higher in the cage group. We inferred from these results that the subsidence of the cage group was higher than that of the Zero-P group. Although these results were not directly related to the clinical outcomes, higher subsidence could worsen degenerative changes of the cervical spine, which might eventually affect cervical spondylotic symptoms.
This study is the first long-term study (more than 2 years) to compare the clinical and radiological outcomes of the Zero-P and the stand-alone cage. The results were mostly similar to those of the previous short-term studies; however, we found that longer-follow-up study could reveal more statistically significant results.
Go to :
CONCLUSION
For one-level anterior cervical discectomy and fusion surgery, the Zero-Profile anchored spacer has advantages for maintaining segmental lordosis and lowering the subsidence rate in long-term follow-up, compared to the stand-alone PEEK cage. The clinical outcomes between the two devices are similar. We suggest the Zero-P anchored spacer as a good substitute for the stand-alone cage in one-level anterior cervical discectomy and fusion.
Go to :
 XML Download
XML Download