

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ossification of the ligamentum flavum (OLF) was first reported by Polgar26) and is characterized by replacement of the ligamentum flavum (LF) with mature and hypertrophic lamina bone20). OLF is commonly detected in the lower thoracic spine181721) where it is a primary cause of slowly progressive myeloradiculopathy13). While patients with thoracic OLF usually have the typical signs and symptoms of myelopathy, many also have coexisting diseases such as cervical ossification of the posterior longitudinal ligament (OPLL), lumbar degenerative diseases, or both172425).
Owing to ambiguous clinical symptoms that are difficult to distinguish from these coexisting spinal diseases, early diagnosis and subsequent treatment can be delayed, despite the increased detection of OLF with the development of radiographic diagnostic technology303236). In patients with compression-related cervical myelopathy and concurrent compressive thoracic or lumbar lesions, long tract signs such as exaggerated deep tendon reflexes at the lower extremities tend to be masked, making the precise identification of the responsible lesion difficult32).
Currently, the few etiologic and epidemiologic studies of OLF are ambiguous and have been mainly reported in East Asia, in particular, China, Japan, and Korea. Recently, epidemiologic investigations of OLF using computed tomography (CT) and magnetic resonance imaging (MRI) have been published, with reported prevalence rates of thoracic OLF ranging from 3.8% to 71.8% in China and Japan71721).
In this study, we assessed the prevalence and distribution of thoracic OLF in 2134 consecutive patients with back or leg pain using lumbar MRI with whole spine sagittal images. Additionally, we examined the presence of coexisting lumbar and cervical disease.
Go to : 
MATERIALS AND METHODS
Subjects
Patients with lower back or leg pain who subsequently underwent lumbar MRI with whole sagittal T2-weighted imaging for the examination of lumbar disease in our hospital between January 2011 and December 2011 were eligible. Of the eligible 2172 patients, 38 patients who had undergone lumbar spinal MRI twice as part of postoperative check-ups were excluded. The presence of OLF as well as clinical parameters such as age, sex, and surgery were retrospectively reviewed. This study has been approved by an institutional review board.
Radiologic assessment
The patients were examined using a 1.5 T MR imaging scanner (MAGNETOM Avanto, Siemens Healthcare, Erlangen, Germany) with spine matrix coils. Whole spine sagittal T2-weighted sequence has routinely been included in our hospital protocol. The imaging parameters were as follows : TR, 4000 ms; TE, 120 ms; and slice thickness, 3.3 mm. Using T2-weighted sagittal imaging from the midline with right or left lateral cuts, we defined OLF as a compressed spinal cord with a midline hypointense signal mass at the posterior margin of the spinal canal. As the LF is thinnest in the midline, OLF is usually more evident on parasagittal MRI31). The severity of thoracic OLF was classified into four grades (0-3) according to the degree of spinal canal compression identified on the whole spine sagittal T2-weighted images and based on the criteria of Han et al.9), which were modified and adopted for this purpose (Fig. 1) : grade 0, no cord compression; grade 1, minimal subarachnoid space compression on the midline image or moderate subarachnoid space compression on the right or left lateral cut image from the midline (off-center image); grade 2, mild cord compression; and grade 3, moderate cord compression or cord signal change. We also examined the distribution of OLF and coexisting lumbar, thoracic, or cervical disease. The diagnosis of OLF and coexisting diseases were read by spine radiologist professor Kim. To test intra- and interobserver reliability, in 30 cases, the severity of thoracic OLF were graded at 2 separate times by fellowship-trained spine surgeon radiologist professor. The intra- and interobserver reliability (mean kappa) for the grade was 0.85 and 0.77, respectively.
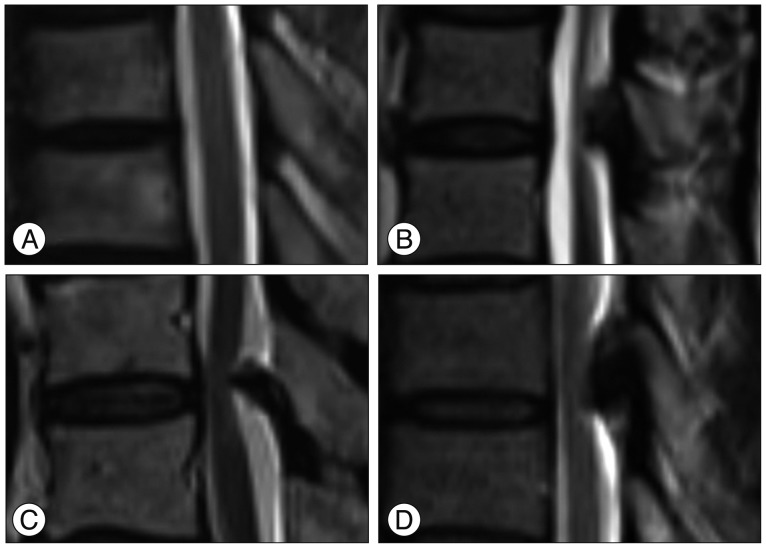 | Fig. 1Grades of thoracic ossification of the ligamentum flavum on whole spine sagittal T2 magnetic resonance imaging. A : Grade 0, no cord compression. B : Grade 1, minimal subarachnoid space compression on the midline image or moderate subarachnoid space compression on the offset image (this image is of the left side). C : Grade 2, mild compression on the midline image. D : Grade 3, moderate cord compression or cord signal change.
|
Statistical analysis
SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. Chi-square tests were conducted to compare ordinal variables. Pearson correlation analysis was conducted to assess the relationship between age and prevalence. Statistical significance was set at p<0.05.
Go to :
RESULTS
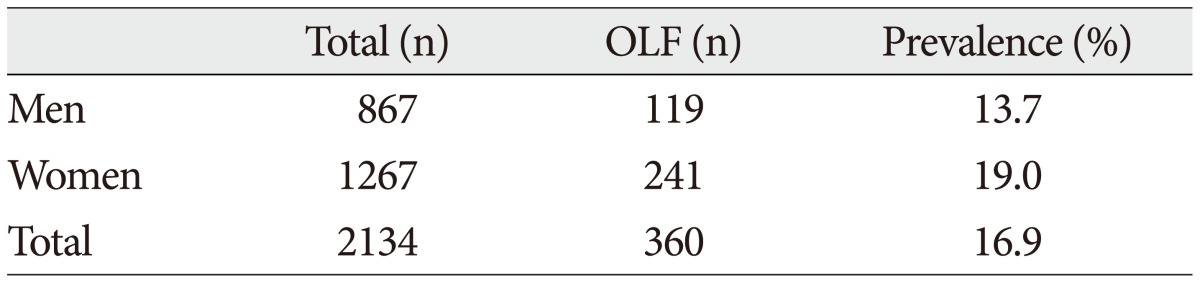
The mean age of the 2134 participants (867 men, 1267 women) was 56 years (range, 11-90 years). The prevalence of OLF was 16.9% (360/2134; 119 men, 241 women) (Table 1). The prevalence of thoracic OLF in women was significantly higher than that in men (19.0% and 13.7%, respectively, p=0.001). The mean age of the patients with OLF was 64 years (range, 20-90 years).
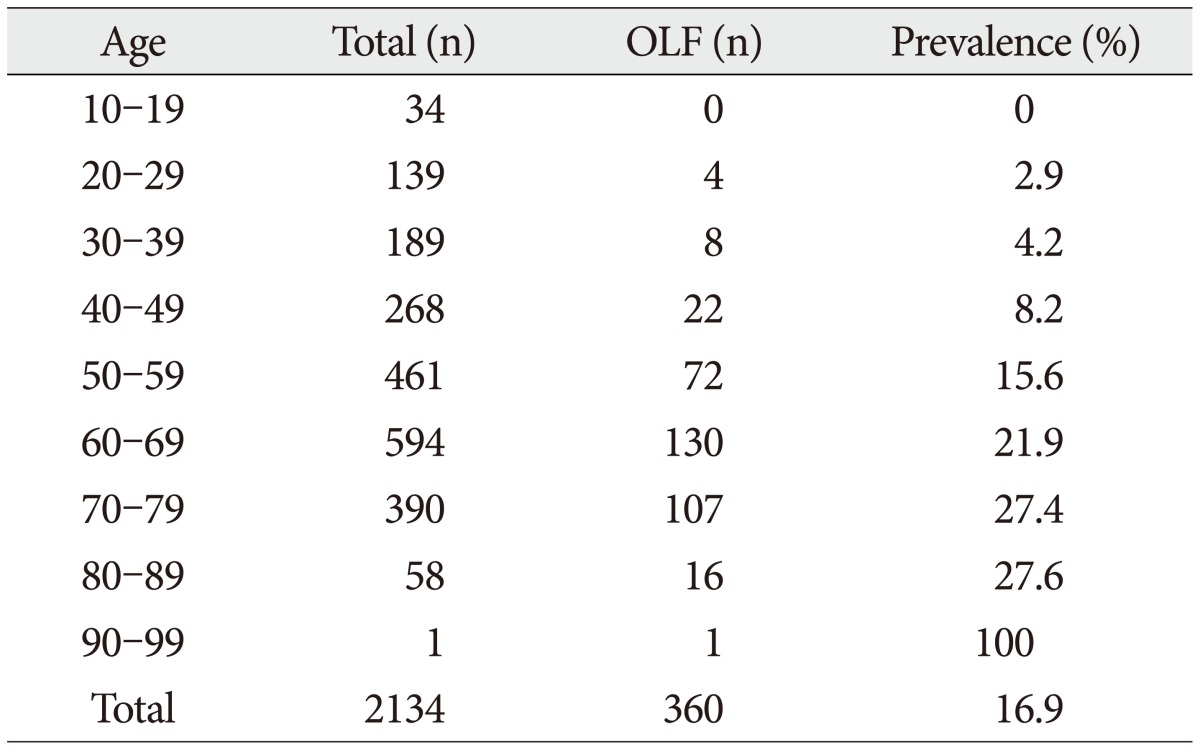
OLF did not occur in patients aged 10-19 years (Table 2), whereas the prevalences in patients aged 20-49 years ranged from 2.9 to 8.2% and from 15.6 to 27.6% in the patients aged 50-89 years. There was a positive correlation between age and OLF prevalence (rs=0.795, p=0.01) (Table 2).
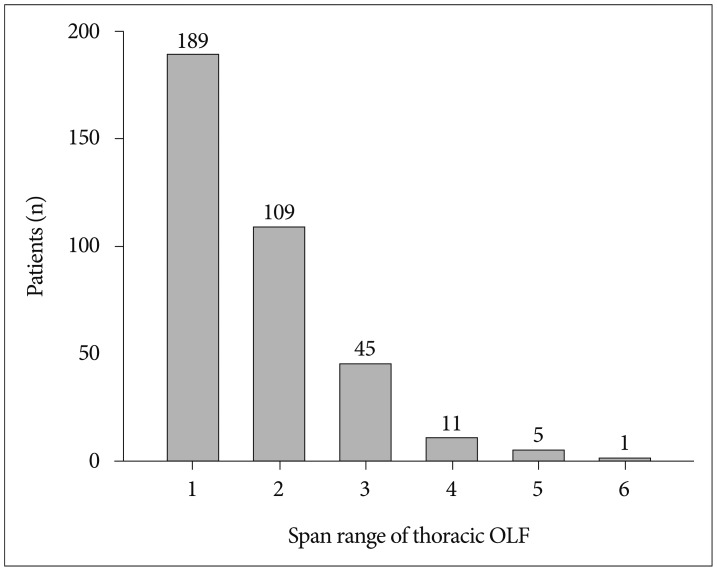
Of all patients with OLF, 189 (52.5%) had a single segment affected (Fig. 3), and 2, 3, 4, 5, and ≥6 segments were affected in 109 (30.3%), 45 (12.5%), 11 (3.1%), 5 (1.4%), and 1 (0.3%) patients with continuous OLF. The lower one-third of the thoracic spine was the most common location overall for OLF.
There were a total of 619 thoracic segments with OLF. The most frequently affected level was T10-11 (207 segments in 57.5% of patients), the second frequently affected level was T9-10 (126 segments in 35.0% of patients), and third frequently affected level was T11-12 (96 segments in 26.7% of patients) (Fig. 2). In the upper thoracic region, T3-4 was the most common level with thoracic OLF. The prevalence was higher in men than in women at T3-4 (p<0.003) and higher in women than in men at T11-12 (p<0.014).
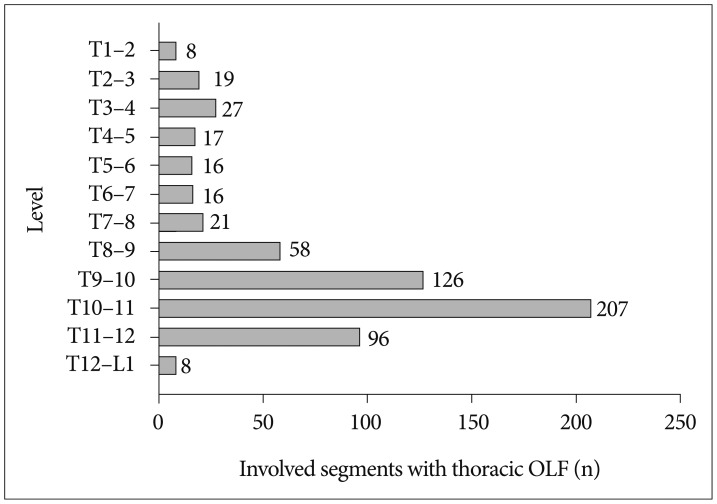
Fig. 4 shows the coexisting lumbar and cervical diseases with thoracic OLF. Herniated thoracic discs (HTD) at the same level as thoracic OLF were detected in 115 (31.9%) of the 360 thoracic OLF patients. At the lumbar level in the 360 thoracic OLF patients, 258 (71.7%) patients had lumbar stenosis, 93 (25.8%) patients had herniated lumbar discs (HLD), and 9 (2.5%) patients had a lumbar spine compression fracture. Of the 258 patients with lumbar stenosis and thoracic OLF, 97 (37.6%) patients also had herniated cervical discs (HCD), 104 (40.3%) patients had cervical stenosis, 5 (5.4%) patients had cervical ossification diseases, and 1 (1.1%) patient had an Arnold-Chiari malformation. Of the 93 patients with HLD and thoracic OLF, 41 (44.1%) patients had HCD, whereas 45 (48.4%) had no cervical disease. Of the 9 patients with lumbar spine compression fractures and thoracic OLF, 3 patients had HCD, whereas 4 patients had no cervical disease.
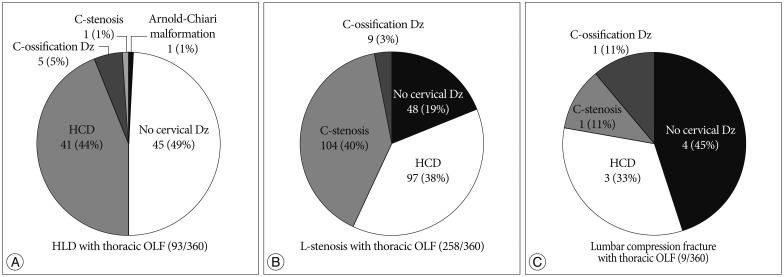 | Fig. 4Distribution of coexisting cervical and lumbar diseases in patients with thoracic ossification of the ligamentum flavum (OLF). Of the 360 patients with thoracic OLF, 93 patients had herniated lumbar discs (HLD) (A), 259 patients had lumbar stenosis (B), and 9 patients had lumbar compression fracture (C). HLD : herniated lumbar disc, HCD : herniated cervical disc, OLF : ossification of the ligamentum flavum, Dz : disease, C-ossification Dz : cervical ossification disease, L-stenosis : lumbar stenosis, C-stenosis : cervical stenosis.
|
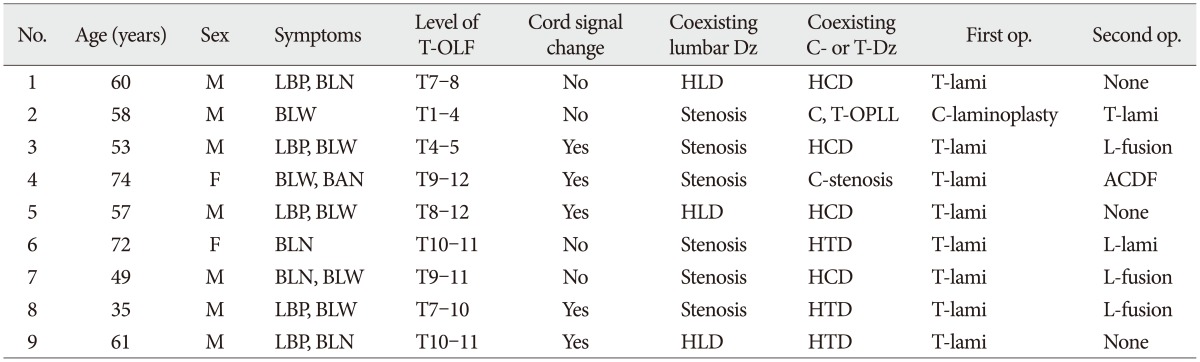
Of the 360 patients, grade 1 thoracic OLF was detected in 300 patients (83%) (Fig. 5). Grades 2 and 3 were detected in 47 (13%) and 13 (4%) patients, respectively. Nine (2.5%, all grade 3 severity) of the 360 patients underwent surgery for thoracic OLF (Table 3, Fig. 5), 8 among whom underwent thoracic decompressive laminectomy as the first operation for thoracic OLF, and 1 patient underwent a second surgery for thoracic OLF after a cervical laminoplasty as the first operation. Of these 9 patients, 6 patients had cord signal changes on T2-weighted sagittal MRI and complained of weakness in both legs, diagnosed as myelopathy. Representative case of thoracic OLF was shown in Fig. 6.
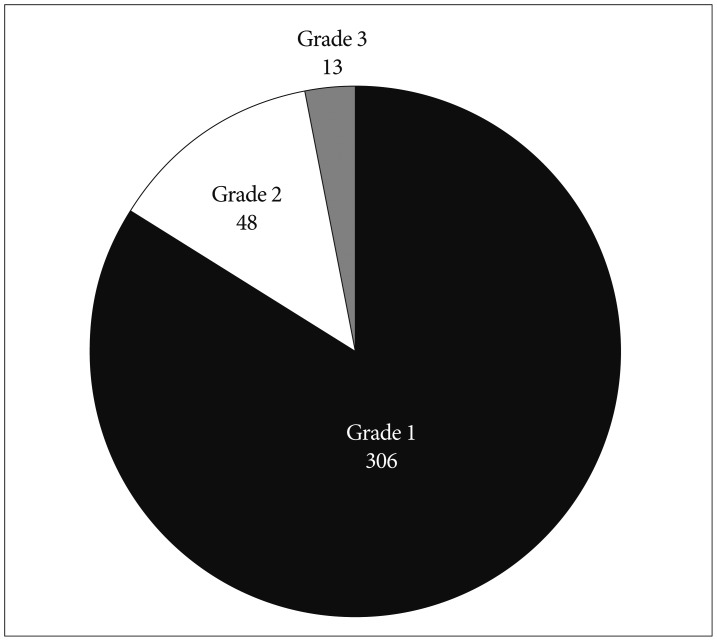 | Fig. 5Distribution of the grades of thoracic ossification of the ligamentum flavum in 360 patients with back pain. Grade 1 : minimal arachnoid space compression, Grade 2 : mild cord compression, Grade 3 : moderate cord compression or cord signal change.
|
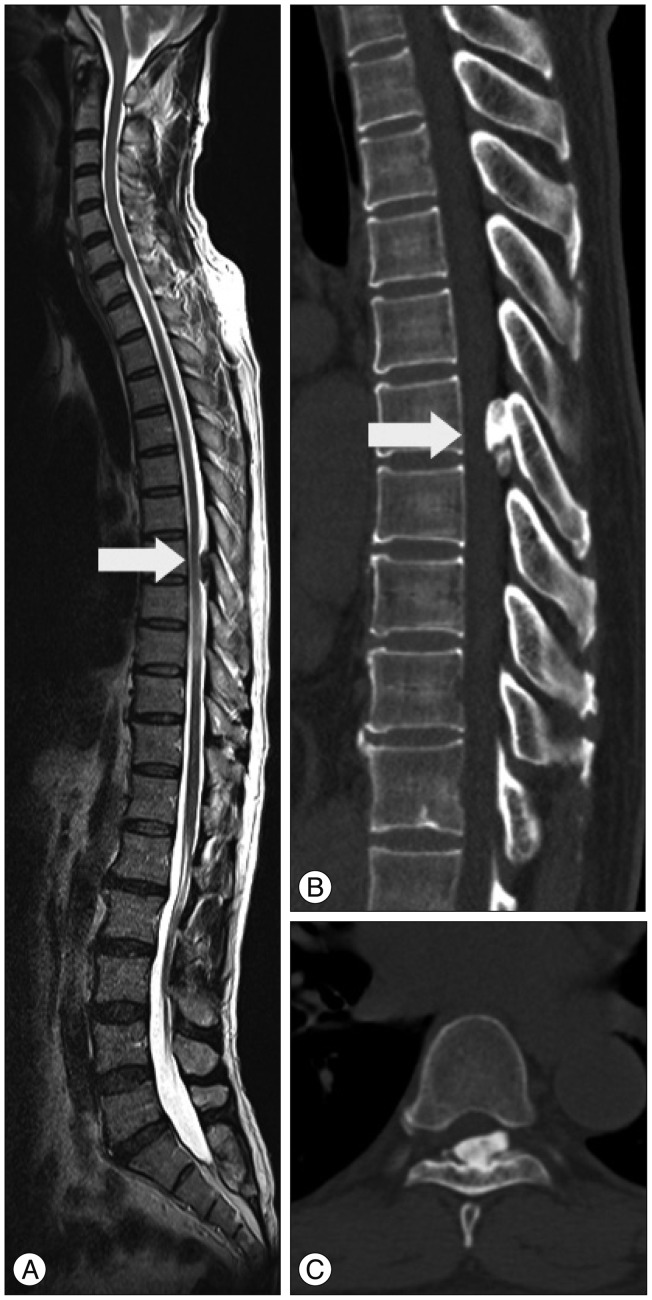 | Fig. 6Representative case of a patient with thoracic OLF; a 60-year-old patient complained of lower back pain and numbness in both legs. A : Whole spine sagittal T2-weighted magnetic resonance imaging showing thoracic OLF, which compresses the spinal cord at the T8 level. B and C : Computed tomography showing a large section of thoracic OLF in the sagittal and axial views, with >50% of the spinal cord compressed by the thoracic OLF. The patient underwent decompressive surgery with removal of the thoracic OLF.
|
Table 3
Patients with thoracic ossification of the ligamentum flavum who required surgery
M : male, F : female, T-OLF : thoracic ossification of the ligamentum flavum, LBP : lower back pain, BLN : numbness in both legs, BLW : weakness in both legs, BAN : numbness in both arms, Dz : disease, HLD : herniated lumbar disc, HCD : herniated cervical disc, OPLL : ossification of the posterior longitudinal ligament, op. : operation, lami : laminectomy, ACDF : anterior cervical discectomy and fusion, C : cervical, T : thoracic, L : lumbar
![]()
Go to :
DISCUSSION
In this study, the prevalence of thoracic OLF with lumbar disease was 16.9%, which differs from that reported by previous studies conducted in other countries using various imaging modalities : 3.8% in the general Chinese population using spinal MRI7), 63.9% in Chinese patients with chest symptoms using chest CT17), and 36% in Japanese patients with no spinal problems using chest CT21). Our findings are higher than those using MRI and lower than those using chest CT. These differences likely resulted from the diversity of participants and different imaging modalities. The patients in the present study, with lumbar disease, had a greater level of spinal degeneration than those in the other studies, which included the general population and patients with chest symptoms and no spinal problems. Furthermore, MRI is a less sensitive modality than CT for the detection of OLF. As a result, the investigation of OLF using CT is more precise, leading to a higher prevalence.
Although CT is an excellent choice for detecting the local extent of OLF and axial morphology of the spinal canal, MRI provides useful information concerning the specific segmental involvement, coexisting diseases such as HTD and OPLL, and the effects on the underlying spinal cord. Furthermore, Xiong et al.34) reported a good correlation between CT and MRI findings regarding the level, side, and general degree of severity of central spinal canal stenosis by thoracic OLF. On T2-weighted MRI, OLF appears as a hypointense signal at the level of the posterior margin of the spinal canal, which is comprised of the spinal canal and spinal cord.
In addition, T2-weighted MRI of the whole sagittal spine provides information about disc herniation, stenosis, and ligament ossification of other spinal regions beside the surgical site of interest9). Using whole spine sagittal T2-weighted MRI, Han et al.9) detected meaningful coexisting spine lesions in other spinal regions in 31.1% of patients who required surgical intervention for degenerative spinal diseases, and Park et al.25) reported a high prevalence of symptomatic thoracic ligament ossification in patients who underwent surgery for cervical OPLL (33.8%) and defined this phenomenon as tandem ossification. This high prevalence of compressive spinal lesions associated with ligament ossification disease may be related with genetic effects in addition to multiple occurrences of OPLL or OLF on different spinal columns. Therefore, whole spine sagittal T2-weighted MRI is highly recommended for elderly patients or those with ligament ossification diseases915).
The present results support this recommendation; it was not uncommon to find patients who had lumbar disease with concurrent thoracic OLF that was found coincidently. Furthermore, a large number of lumbar and cervical disease patients with coexisting OLF were found in the present study, including those with lumbar stenosis (n=258, 71.7%), disc herniation (n=93, 25.8%), and lumbar fracture (n=9, 2.5%). Unnoticed multiple level lesions can have serious consequences; the development of thoracic paraplegia owing to missed OLF in the thoracic spine after lumbar decompressive surgery for stenosis and spinal cord compression has been reported32). Moreover, OLF is frequently misdiagnosed and treated inappropriately owing to the presence of other spinal diseases15).
The pathophysiology of OLF is similar to that of LF hypertrophy. Degeneration of the LF is due to hypermobility of the posterior column, which results in collagen hyperplasia and hypertrophy of the LF. Subsequent deposition of calcium pyrophosphate dehydrate and calcium hydroxyapatite occurs in the ligament, resulting in OLF5). The pathology of LF hypertrophy includes fibrocartilaginous changes due to proliferation of type II collagen, ossification, calcium crystal deposition, degeneration of collagen and elastic fibers, and chondroid metaplasia of ligament fibroblasts5627). Ossification of the spinal ligament is characterized by heterotopic bone formation in the spinal ligaments, which are normally composed of fibrous tissue10). Chondroid metaplasia in LF hypertrophy appears to play a pivotal role in ligament ossification, as cartilage differentiation, hypertrophy, and cell death are followed by bone formation in the bone morphogenetic pathway4).
OLF is often associated with ossification of the posterior longitudinal ligament, ankylosing spinal hyperostosis, and diffuse idiopathic skeletal hyperostosis232836). Several investigators have postulated that mechanical stress on the spine contributes to accelerated ossification1214). Furthermore, disc degeneration and herniation coincides with OLF were also observed. The present study also showed coexisting HTD at the same level of OLF in 31.9% (n=115/360) of the patients. The association of thoracic OLF with both thoracic OPLL and HTD has also been reported in the literature193335). In contrast, 98 (4.5%) of the total 2134 patients did not have any lumbar spinal diseases or thoracic OLF. These results support the existing evidence that mechanical stress and hypermobility of the spine results in hypertrophy and ossification of the LF subsequent to LF degeneration, disc degeneration, and herniation.
OLF occurred the most frequently in the lower thoracic segments (T9-12)121721). These regions are the transition point between the thoracic and lumbar spine, where there is less anatomic protection from the rib cage. Thus, this area is possibly more prone to degeneration as a result of the high tensile forces present in the posterior column. As a result, collagen hyperplasia and hypertrophy occur with subsequent deposition of calcium pyrophosphate dehydrate and calcium hydroxyapatite in the ligament, leading to OLF5). Alternatively, it has also been suggested that OLF is a degenerative response to microinjury of the LF18).
The prevalenceof OLF gradually increased with age, from the ages of 20 to 90 years, indicating that the development of OLF may be associated with spinal degeneration. The prevalence of OLF was also higher in women (19%) than in men (13.7%). There are conflicting results in previous studies regarding the sex distribution of OLF, with some previous studies reporting a higher prevalence in men1120), potentially owing to greater stress on the LF from higher levels of physical activity in men, and others reporting a higher rate of OLF in women3716). We believe that the higher prevalence in women in the present study may have resulted from the greater enrollment of women than men and a different patient population from those in previous studies.
There were some limitations in the present study. First, we investigated OLF and other spinal diseases using MRI and lateral thoracic spine radiography. It was difficult to clearly distinguish between OLF and LF hypertrophy. Therefore, overestimation or underestimation of OLF may have been due to using only MRI. However, there was a good correlation between CT and MRI findings in previous studies regarding the level, side, and general degree of severity of central spinal canal stenosis caused by thoracic OLF34). Moreover, whole spine MRI made it easier to diagnose OLF in the early stages22). Second, we were unable to evaluate the association between OLF and related clinical manifestations for the whole sample. OLF is usually asymptomatic when the lesions are small, with a reported 25% of thoracic OLF as asymptomatic29). Further studies are required to determine the association between clinical manifestations of lumbar and/or cervical disease and thoracic OLF.
Go to :
CONCLUSION
To the best of our knowledge, this is the first study to report the prevalence rate of thoracic OLF using whole spine MRI in Korean patients with lumbar symptoms, resulting in a prevalence of thoracic OLF of 16.9%. The prevalence was higher in women and tended to increase with age. The lower thoracic segment of T10-11 was the most common segment affected. Approximately one-third of the patients were also diagnosed with coexisting HTD at the same level, and approximately three-quarters of the patients had coexisting lumbar or cervical disease. Nine (2.5%) of 360 thoracic OLF patients underwent surgery for thoracic lesion. Therefore, we should check coexisting spinal diseases and the exact diagnostic localization of ossification besides lumbar disease using whole spine sagittal MRI.
Go to :
 XML Download
XML Download