

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dural arteriovenous fistulas (dAVFs) of the superior sagittal sinus (SSS) account for 8-11% of intracranial dural fistulas1,4). Treatment is often challenging because of multiple and bilateral arterial feeders, most commonly the middle meningeal arteries (MMAs). Transarterial embolization and surgical coagulation of draining vein are preferred treatment options for SSS fistulas, especially in the anterior third of SSS. However, due to the penetration capability of Onyx, transarterial Onyx embolization can result in complete obliteration of dAVF in post-Onyx era. It is important to locate the tip of microcatheter near the fistula as close as possible to obliterate fistula successfully with Onyx. However, superselection of MMA feeders is not always possible when proximal part of MMA is tortuous.
Recently, a combination of surgical and endovascular techniques, including direct-puncture transvenous embolization during surgery or transvenous embolization alone, has been described. And we introduced a case of DAVF within the wall of SSS associated with cortical venous reflux, which was embolized with direct puncture technique after failed initial conventional transarterial endovascular therapy.
Go to : 
CASE REPORT
Case presentation
A-66-year-old woman was transferred to our hospital for the evaluation of intermittent paraparesis. She had a history of head injury, which was acute subdural hematoma managed conservatively 3 years ago in our hospital. She has been doing well without sequale even though she complained of intermittent headache for 2 years.
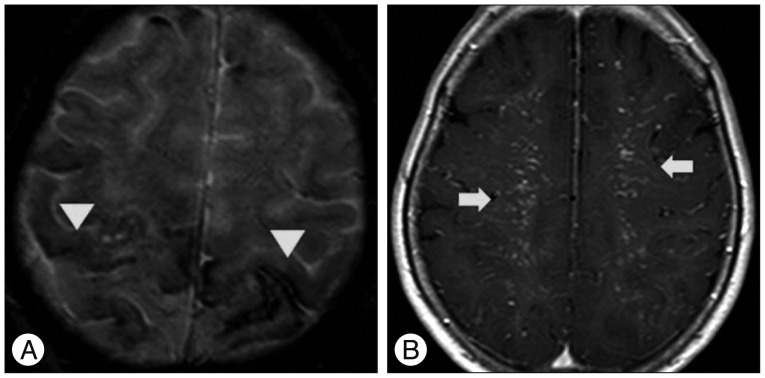
On admission, she complained of gait ataxia because of intermittent paraparesis, which was more severe in the left lower extremity, and left hand tremor for 2 weeks. However, her weakness was not definite on neurologic examination. Whole spine magnetic resonance image (MRI) demonstrated no abnormal findings, but brain MRI revealed multiple signal void lesions on both fronto-parietal convexity suggesting vascular lesion (Fig. 1), which was not visible on previous MRI performed 3 years ago. Before the planned cerebral angiography was done, sudden generalized tonic-clonic seizure was developed.
Angiography depicted a dAVFs on the SSS fed by both MMAs, superficial temporal arteries (STAs) and occipital arteries (OAs) and drained into the occluded SSS retrograde fashion, then mark-ed reflux to bilateral superficial cortical veins. There was no feeder from both internal carotid arteries. Because the SSS was occluded at the posterior one third, most cerebral venous outflow was drained into deep venous system through internal cerebral vein and straight sinus to transverse sigmoid sinus (Fig. 2). These dAVFs were classified as type IIa+IIb according to Cognard et al.1).
 | Fig. 2Angiography depicting dural arteriovenous fistulas on superior saggittal sinus (SSS) fed by both middle meningeal arteries (arrowheads), superficial temporal arteries (arrows) and occipital arteries (A) and draining into the occluded SSS retrograde fashion, then marked reflux to bilateral superficial cortical veins (B). There was no feeder from both internal carotid arteries and most cerebral venous outflow was drained into deep venous system through internal cerebral vein and straight sinus to transverse sigmoid sinus (C).
|
Endovascular embolization
1st embolization
Under the general anesthesia, bilateral femoral arterial punctures were done. Through right femoral artery, a 6 F Envoy (Cordis, Miami, FL, USA) guiding catheter was advanced to the right external carotid artery (ECA). And a 5 F diagnostic catheter was placed to the left common carotid artery to evaluate the degree of dAVFs obliteration during the procedures. Initially, Echelon-10 (ev3 Neurovascular, Irvine, CA, USA) microcatheter was navigated through the 6 F guiding catheter, but it was very difficult to navigate the tortuous turning point beyond the foramen spinosum level (Fig. 3A). Thus, the microcatheter was changed to Marathon (ev3 Neurovascular, Irvine, CA, USA) catheter, however, it was impossible to get access the fistula portion. Thus Onyx injection was done from the proximal frontal branch of MMA, but resulted in the incomplete obliteration.
 | Fig. 3Radiologic images obtained during first embolization session. Lateral view of roadmap image showing the tortuous turning point (arrow) beyond the foramen spinosum level (A). Postoperative skull radiographs showing the Onyx cast after incomplete embolization (B). Postoperative angiogram showing the incomplete obliteration of dAVFs (C). dAVFs : dural arteriovenous fistulas.
|
So, we performed Onyx embolization from the petrosal branch of MMA and the parietal branch of STA. Total of 4 cc Onyx was injected during the first session through right ECA branches. However, the infiltration of Onyx into the fistula was not successful from these vessels (Fig. 3B, C).
2nd embolization
Even though her paraparesis was improved a lot after the first incomplete embolization of dural AVF, 2nd procedure was inevitable to prevent fatal hemorrhage, or seizure.
2nd embolization was composed of direct MMA puncture through the small decortication on the left frontal bone overlying the MMA beyond the turning point. After one week, left transcranial arterial embolization was performed under the general anesthesia in the angiosuite. She was placed on supine position and the head was rotated 60 degree to the opposite side. A 5 F diagnostic catheter was placed to left ECA with continuous heparinized saline irrigation. Under the roadmap guidance, exact location of MMA to be punctured was marked with drill tip (Fig. 4A). After a small semilunar shaped scalp incision was made, decortication of temporal bone using diamond drill was performed on the distal part of turning point of MMA (Fig. 4B). A 10 mg of verapamil was infused through the catheter to dilate the MMA because it was not large enough to puncture successfully.
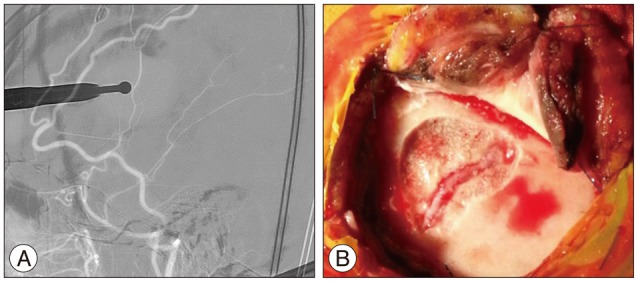
Direct puncture of MMA using 20 G angioneedle was done without difficulty. Hairwire was inserted into the MMA and 5 F micropuncture sheath was placed over the wire. This sheath was fixed with black silk tie to prevent accidental removal during the procedures (Fig. 5). Through the sheath Echelon-10 (ev3 Neurovascular, Irvine, CA, USA) microcatheter was introduced and advanced to the fistula portion near the SSS. Microangiogram demonstrated dAVF clearly. Onyx injection (total 3.9 cc) from this single artery resulted in complete obliteration of AVF without remnant (Fig. 6). And on post operative angiogram, AVF from both STAs and OAs was also completely obliteration.


Postoperatively, she recovered well and her paraparesis was improved to normal. Diffusion weighted image showed no abnormal high signal lesion on brain parenchyma. Computerized tomography (CT) scan showed Onyx cast within the fistula and arterialized cortical veins.
Go to :
DISCUSSION
DAVFs involving the SSS are rare but have aggressive clinical symptom and intracranial hemorrhage due to the venous hypertension. The resultant encephalopathy can be clinically demonstrated on dementia, gait ataxia, seizure, myelopathy, cerebral edema, ischemia, subarachnoid hemorrhage, or any combined of several these signs and symptom12). If the cortical venous reflux persists, annual risk of hemorrhage or non hemorrhagic neurological deficits is known to be 15% along with an annual mortality rate of 10.4%. Cognard et al.1) noted intracranial hemorrhage in 10% of patients with type II, 40% with type III and 65% with type IV DAVFs.
Recently, there are many multimodality treatment modalities including compression, transvenous, transarterial embolization, surgery, and radiosurgery3,6). In addition, especially on DAVFs involving the SSS, a combination of surgical and endovascular techniques, including direct-puncture transvenous embolization during surgery or transvenous alone has been described4,8,10). And, stent placement for occluded sinus is an additional treatment option for DAVFs involving the SSS13).
In this case, we considered many endovascular treatment options including transvenous coil embolization, SSS stenting, and transarterial Onyx embolization5,7,15). Of these, transvenous coil embolization required surgical exposure of SSS, which had a disadvantage of excessive bleeding. Although SSS stenting could convert aggressive type to benign type, it was considered difficult because the length of occlusion was long13).
Therefore, we decide to try transarterial embolization with Onyx. Onyx has an advantage of nonadhesive nature and penetration capability over n-butyl-2-cyanoacrylate. There have been many successful reports on transarterial Onyx embolization of dAVFs2,8).
We tried transarterial Onyx embolization using MMA, however, it was not successful because of proximal tortuousity of MMA. If we can get access to the fistula through MMA, there is a high likelihood of complete obliteration of dAVF with Onyx. To overcome the proximal tortuosity of MMA, we performed direct MMA puncture.
Transcranial combined approach using direct puncture technique is sometimes very useful when a traditional transfemoral transarterial approach was failed. Many neurosurgeons has successfully treated for dAVFs using transcranial approach for venous embolization5,11). We treated this case using transcranial approach for arterial embolization. Koh et al.9) reported transcranial transarterial approach with craniectomy for occlusion of dAVFs combined with SSS. In our case we used diamond drill to decorticate the temporal bone to prevent accidental damage to MMA5,11,14). Decortication is more beneficial in cosmetic aspect and more safe for preserving the MMA, instead of burrhole or craniectomy. Then verapamil injection through the catheter can dilate MMA and prevent the vasospasm.
Go to :
 XML Download
XML Download