

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Schwannoma (neurilemmoma) is a benign tumor that arises mainly in sensory nerve sheaths24). Intraosseous lesions are rare, accounting for less than 0.2% of primary bone tumors3), and the majority are located in the mandible and sacrum68916). Other reported sites include the ulna, humerus, femur, tibia, ribs, patella, scapula, maxilla, the small bones of the hands, and vertebral bodies2). Spinal intraosseous schwannoma (SIS) was first reported in 19645). SIS is an extremely rare lesion, and the diagnosis remains unclear, mostly because of its origin. This is the focus of controversy between some authors, whereas the pathological diagnosis and surgical treatment are quite similar. Correctly diagnosing SIS without resection is difficult given the broad range of symptoms. However, appropriate diagnosis is important to properly plan surgical intervention. Magnetic resonance imaging (MRI) with contrast can be useful in preoperatively diagnosing SIS, and histopathology is very informative for resected specimens. Here, we report two cases of intraosseous schwannoma involving the body of L4 and the posterior structures of T9 that were diagnosed following myelopathic symptoms.
CASE REPORT
Case 1
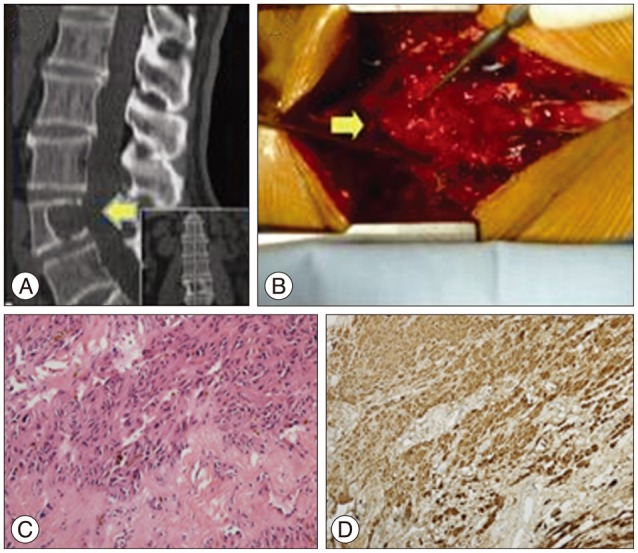
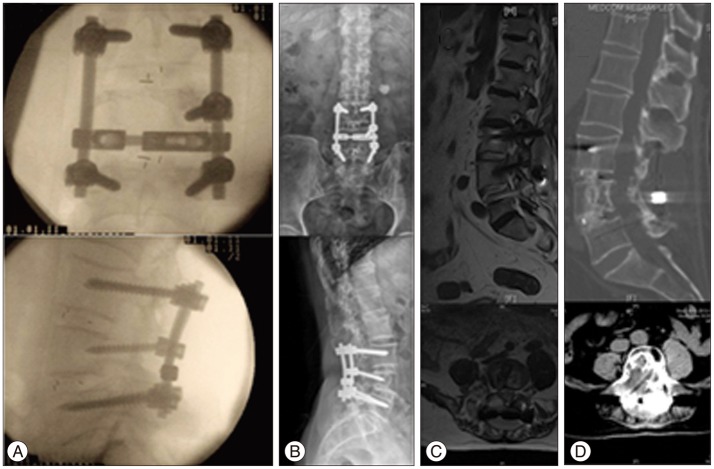
A 71-year-old man experienced right lumbocrural pain and gait disturbance accompanied by paresthesia and right leg weakness for 6 months. Neurologic examination revealed impaired right leg motor function (grade 3/5) with diminished feeling on the right side caudally from the lumbar L4 sensory dermatome; however, his nerve reflexes were normal. Enhanced magnetic resonance imaging (MRI) (Fig. 1) showed a mass with lesions in the vertebral body (L4) and spinal canal compressing the lumbar spinal cord. Computed tomography (CT) scan revealed a slowly growing tumor with severe vertebrae destruction (Fig. 2A, arrow). Piecemeal resection and decompression were performed. After total laminectomy and facetectomy of L3-5, a well-demarcated tumor was exposed extending into the spinal canal (Fig. 2B, arrow) without nerve involvement or dural adhesions. The spine was stabilized with pedicle screws and rods after the tumor was completely resected. Histological characteristic of the tumor revealed Antoni A and B tissue (Fig. 2C) and overexpression of S-100 protein (Fig. 2D), which confirmed a diagnosis of intraosseous schwannoma without originating nerve remnants. Intraoperative fluoroscopy revealed successful internal fixation (Fig. 3A). Postoperative images taken at the 2-year follow-up showed no obvious evidence of recurrence and general bony fusion (Fig. 3B, C, D), and the patient's gait and sensation in the right lower extremity showed good recovery.
Case 2
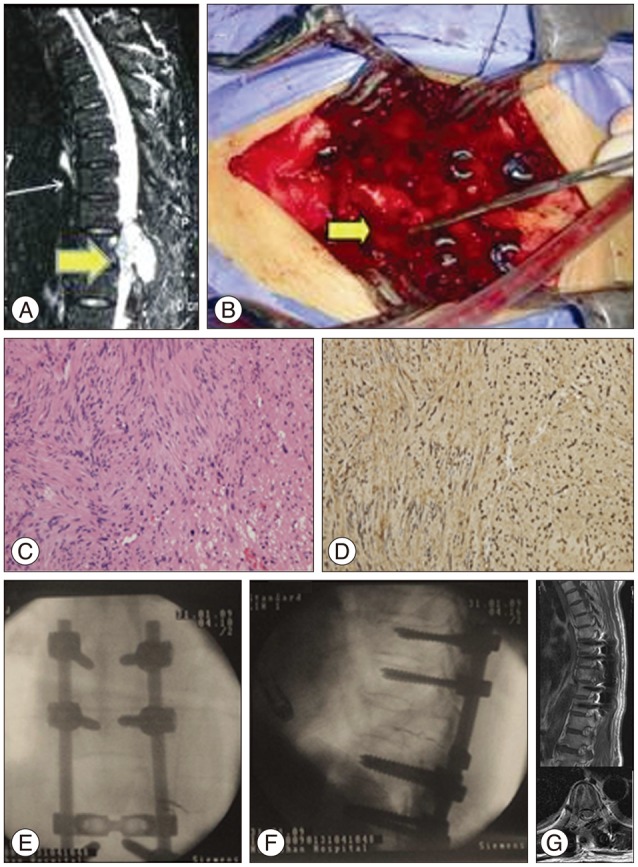
A 54-year-old female reported a 4-month history of gait disturbance and paresthesia of both lower extremities. Physical examination revealed numbness in both legs without obvious weakness (grade 5/5); nerve reflexes were normal. MRI (Fig. 4A) showed a mass (arrow) that appeared to originate from the posterior elements of T9 and extended into the spinal canal and paravertebral areas, extruding the spinal cord. T9 vertebrae bone erosion was observed on CT. The imaging results led to a differential diagnosis of primary benign/malignant bone tumor or metastatic tumor. The tumor was completely separated and surgically resected from the spinal nerve root with a clear border, and a posterior fusion with allograft bone was performed to stabilize the spine. Pathological characteristics of the tumor confirmed a benign schwannoma (Fig. 4C, D). Intraoperative fluoroscopy demonstrated successful internal fixation in the proper position for posterior interbody fusion (Fig. 4E, F). According to the MRI images at the 4-year follow-up, there was no obvious sign of reoccurence with relieved gait and sensation disturbance (Fig. 4G).
DISCUSSION
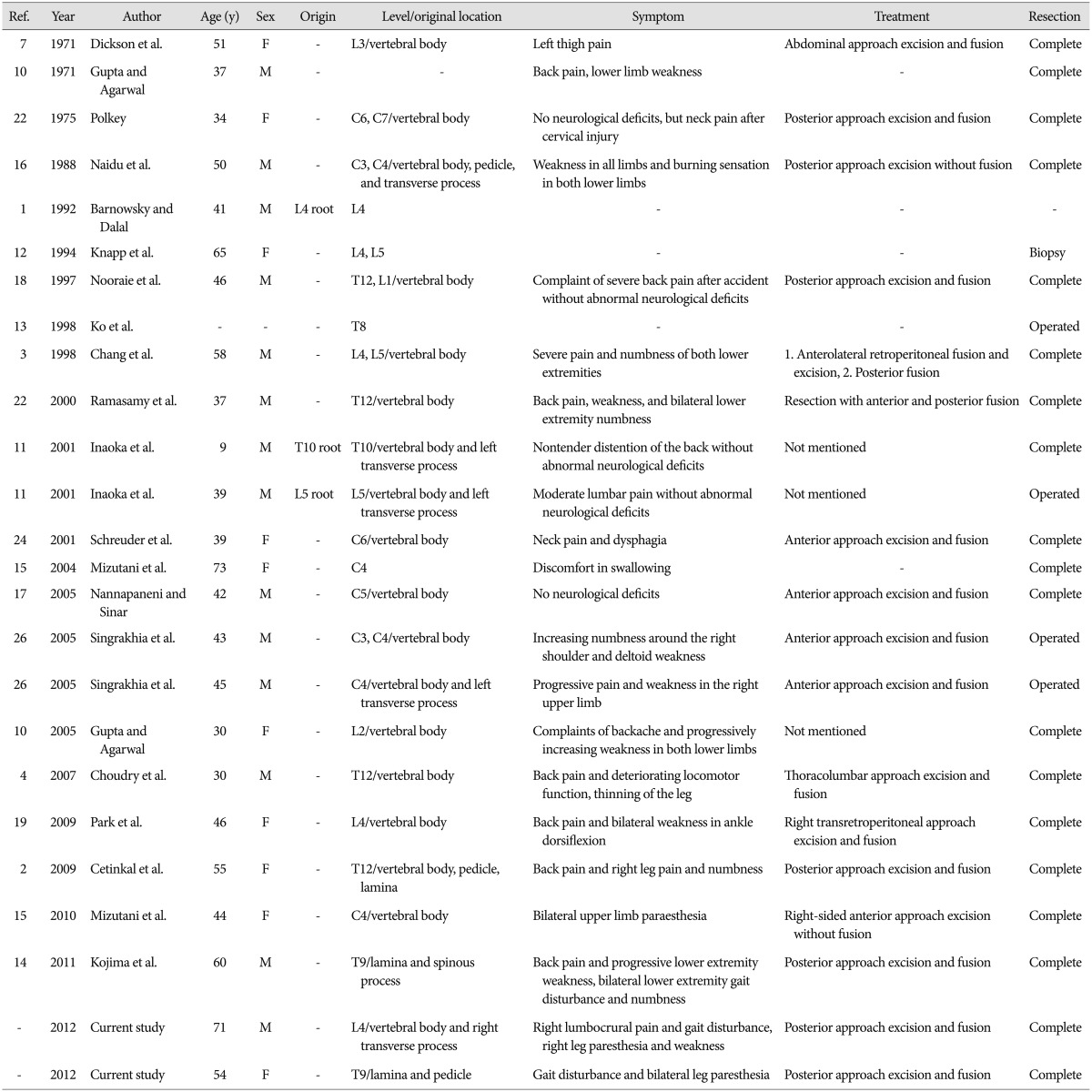
Although SIS is quite rare, a number of cases have been published in the last 30 years123471011121314151617181921222427). We looked at images in the cited articles and found classic pre- and intra-operative images of SIS to ensure that there was no connection between the tumor and nerve tissue, but the photos were not always convincing. Our report aims to provide a clear definition of SIS and a review of this rare disease. Because the symptoms associated with SIS can vary depending on their location in the spinal cord and because they can overlap with those manifested in other conditions, incorrect diagnosis remains a problem. A relatively complete summary of SIS cases described from 1971-2012 is shown in Tables 1, 2. Though the cases reported by Barnowsky and Dalal1) and Inaoka et al.11) showed that Schwannoma originated from nerve root. It was defined as SIS by Park et al.19). The majority of reports do not hold this view, and we determined those cases were probably intraosseous invasions of extraosseous nerve sheath tumors. It is known that neurilemmomas can involve bone by three possible mechanisms : 1) an extraosseous tumor causing secondary bone erosion; 2) a tumor arising centrally within the bone; and 3) tumor origination in the nutrient canal followed by growth into a dumbbell-shape that enlarges the spinal canal36911222324). Of these, only the second mechanism could occur with intraosseous neurilemmoma; the small nerves that give rise to these tumors have been described in the human vertebrae2025). In other words, the intraosseous origin of schwannoma must be nerves within bones that are free from adjacent neural tissue.23) This view is supported by most reports in the SIS literature.211)
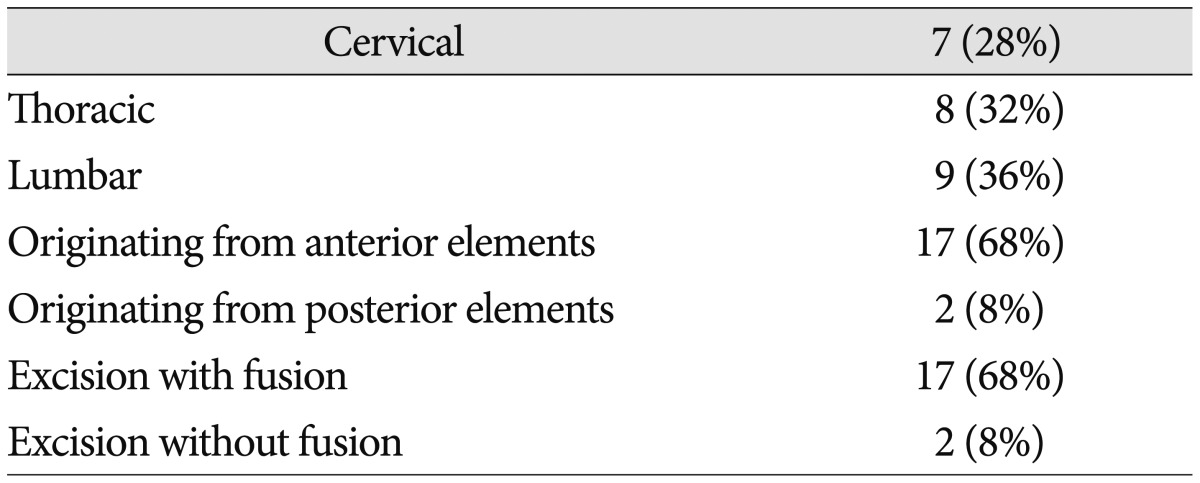
Symptoms vary among SIS patients. Because most of these tumors enlarge slowly,19) the patient's history may be considerably long, and most experience pain (14/25, 56%) depending on the tumor location.24) Neurological compression symptoms develop when the tumor perforates the bone cortex and causes spinal cord protrusion, but specific symptoms can differ depending on the level of the lesion.22) SISs are most commonly found in the lumbar region (38%), followed by thoracic (32%) and cervical (28%), which is different from the results reported by Park et al.19)
Radiological findings in SIS can also vary considerably, and differential diagnosis includes ruling out solitary myeloma, chordoma, chondrosarcoma, giant cell tumor, angioma, and aneurysmal bone cyst. SISs are sometimes found to primarily occupy the intraosseous region with or without extravertebral and spinal canal involvement, and a hollowed out vertebral body with a single, thin, bulging cortex perforation is suggestive of intraosseous origin.3) Generally, intraosseous schwannoma appears on radiological images as a lytic defect with bone erosion lacking new periosteal bone formation and calcification/ossification, although a narrow sclerotic zone may be present between the tumor and bone324). Vertebral intraosseous schwannomas gradually increase in size, resulting in pedicle and vertebral body erosion that widens the foramen and vertebral scalloping.
Histological conformation is mandatory for a diagnosis of SIS. Proliferation of slender spindle cells with oval nuclei and focal palisading nuclei (Antoni A) and degenerated hypocellular areas (Antoni B) with hemosiderin deposition and thrombosed blood vessels are suggestive of schwannoma3). SISs are not histologically different from schwannomas that develop elsewhere, even at the ultrastructural level16), but the histological features of intraosseous neurilemmomas may be obscured in highly cellular lesions with subtle Antoni types A and B patterns11). Both types have long durations16) and similar degenerative characteristics, including perivascular hyalinization, calcification, and cystic degeneration.
The gold standard for benign bone tumors is marginal resection. Unfortunately, this is often difficult to achieve in SISs, which have both intra- and extraosseous components that invade adjacent structures, including nerve roots, spinal cord, and paravertebral tissue16). This is usually addressed with adequate curettage beyond the original margins of the tumor without local adjuvant, which can result in long-term relief without a high recurrence rate24). Despite their tendency to be benign, SISs often result in spinal instability due to severe vertebral body invasion, and fusion with bone graft is required in approximately 68% of cases.
CONCLUSION
We report two cases of SIS, which is a rare differential diagnosis for intraosseous tumor. Proper diagnosis requires radiological tests, gross intraoperative findings, and postoperative histological results. Symptoms vary depending on tumor location, and fusion is necessary to stabilize the spine after the tumor is completely excised.

 XML Download
XML Download