

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The primary epithelial tumors of the lacrimal gland can be generally classified into two groups, benign and malignant lesions. Most of the benign lesions are the pleomorphic adenoma of the lacrimal gland (LGPA)35781319), which is composed of both epithelial and stromal components1419). However, when malignant transformation of LGPA has occurred, most of the reports were the carcinomas, which were malignant changes of the epithelial components1234571112141622). With these characteristics, the American Joint Committee on Cancer (AJCC) called the carcinoma ex pleomorphic adenoma (CEPA)12), which was a carcinoma arising from a preexisting pleomorphic adenoma. Consequently, in according to the previous reviews1234571112141622), the sarcoma arising in a LGPA with malignant changes of the stromal components is very rare. We described a rare case of the sarcomatous lesion of the LGPA.
CASE REPORT
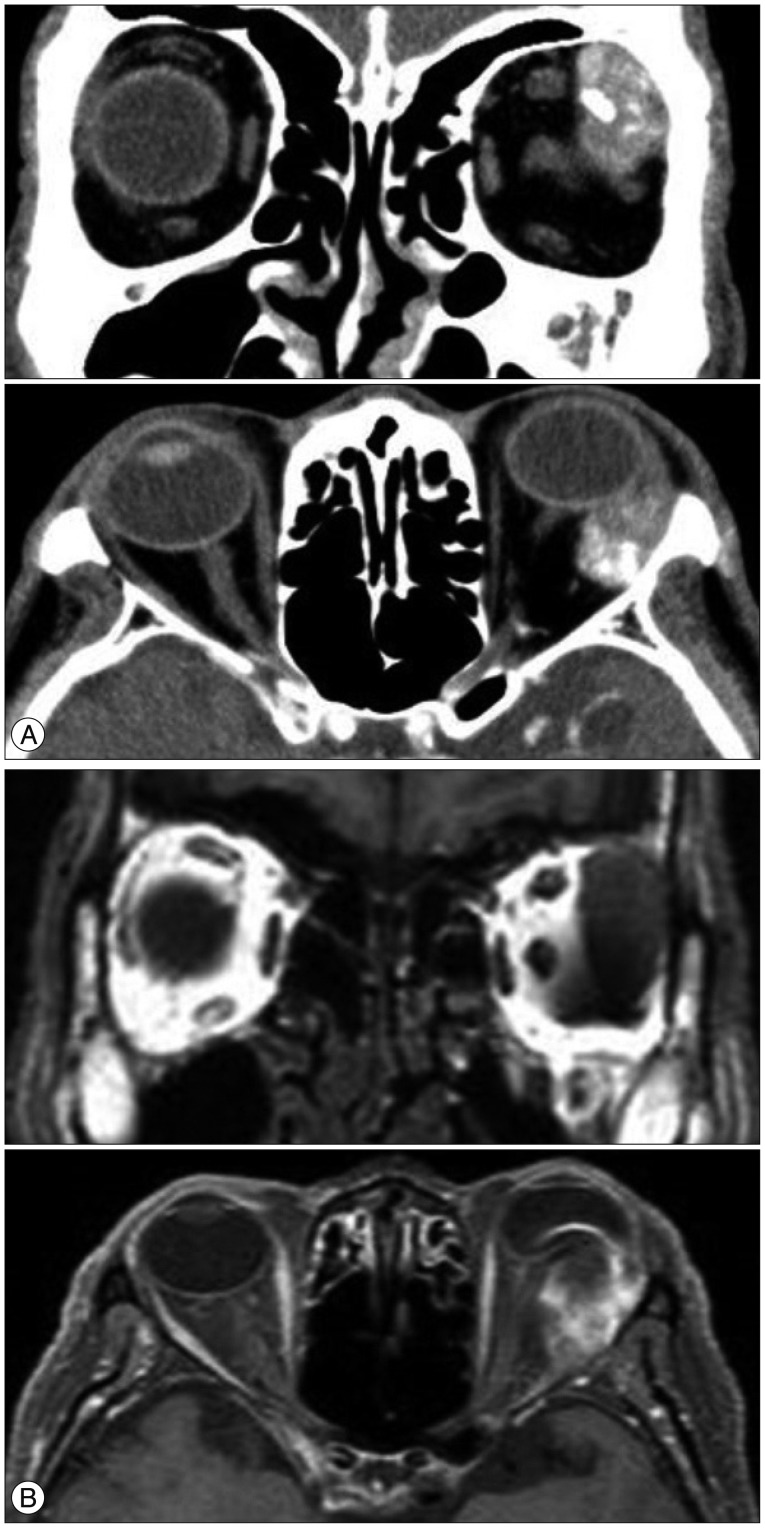
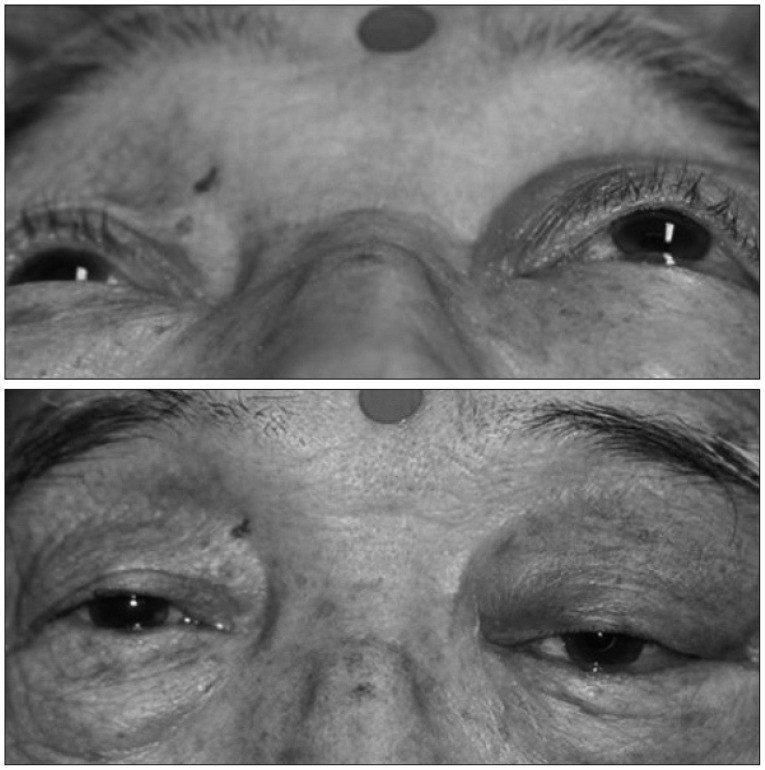
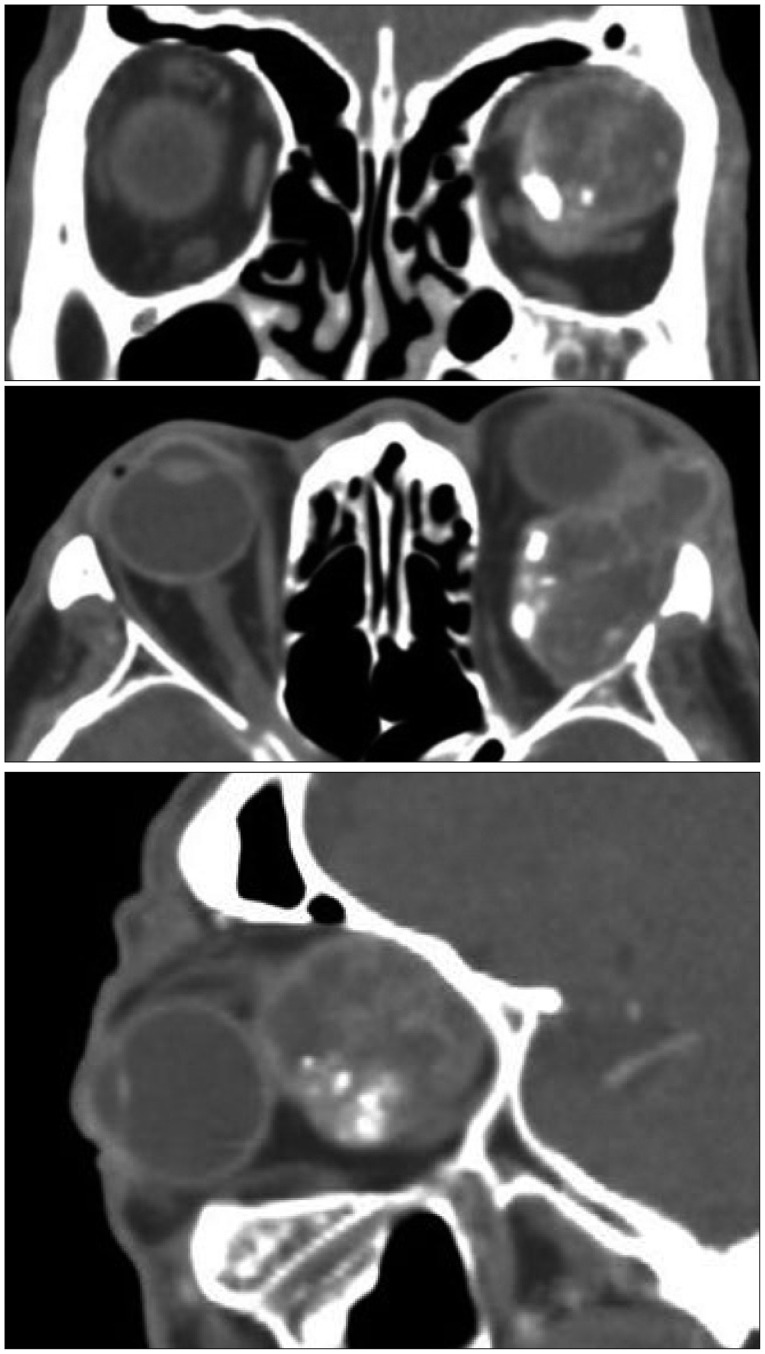
A 69-year-old male presented with a slow progression of the left side exophthalmos during one month. The Hertel exophthalmometer result was 11 mm (OD)/18 mm (OS). Orbital 473computed tomography (CT) and magnetic resonance imaging (MRI) were performed. The CT revealed a well-circumscribed mass lesion with calcification in the supero-lateral area of the left orbit (Fig. 1A). The MRI showed a mass lesion with inhomogenous enhancement in the same area (Fig. 1B). We recommended surgical treatment, but the patient refused the treatment. After 33 months, the patient visited the hospital. He had not undergone any treatment for his disease during the follow-up loss period. His symptoms had worsened severely. The status of the exophthalmos was 12 mm (OD)/22 mm (OS) and the he presented left sided ptosis (Fig. 2). The orbital CT and MRI revealed an expansion of the previous mass and the mass compressed the orbital contents and optic nerve infero-medially (Fig. 3).
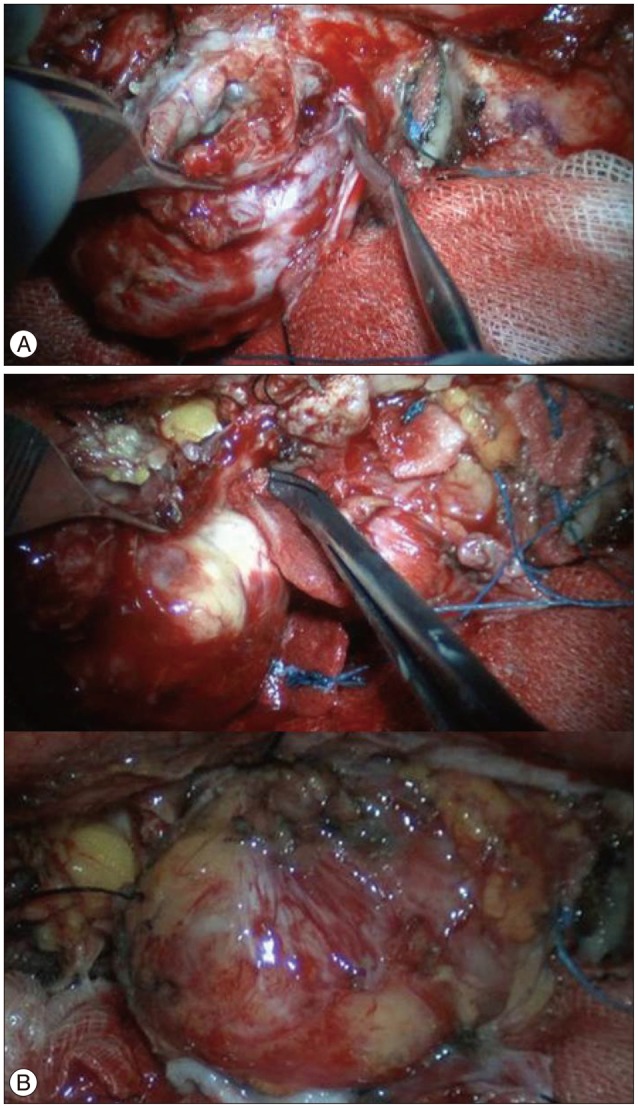
Surgery including a frontotemporal craniotomy and superolateral orbitotomy to expose the periorbita was performed. No extension or infiltration of tumor was detected in the external area of the periorbita. The tumor was relatively well dissected from the surrounding periorbital membrane (Fig. 4A). The tumor was connected to the lacrimal gland. We resected the tumor from the lacrimal gland. After the removal of the mass, a clear surface of the periorbital fat and extraocular muscle was observed (Fig. 4B).
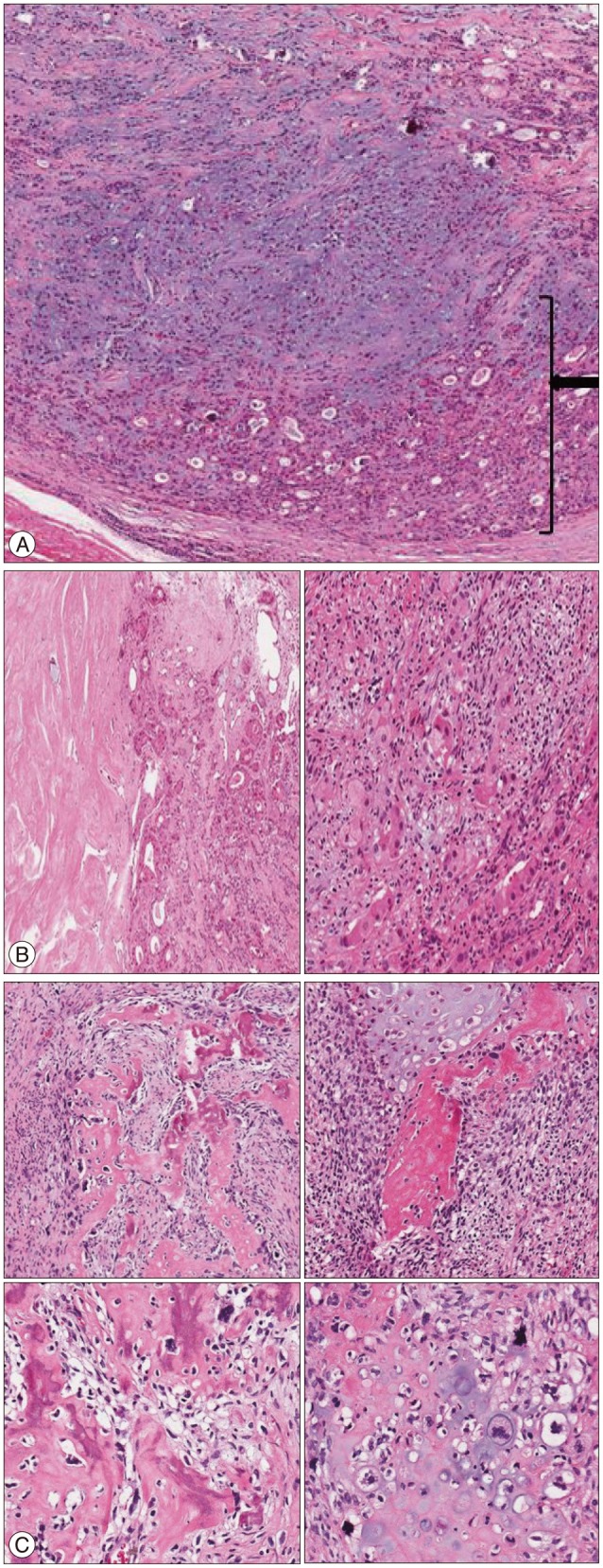
The gross finding of the specimen was central necrosis with surrounding bony cartilage portion, such as osteochondroma. In the pathologic findings, tissues of normal lacrimal gland and typical pleomorphic adenoma were observed (Fig. 5A). On the border of the epithelial and stromal components, the cells of the epithelial components did not have malignant characteristics (Fig. 5B). However, in the pictures of the bone and cartilage, the nucleus of the osteoblast appeared to be malignant, and the cells around the bone and cartilage were increased (Fig. 5C). Thus, our diagnosis was osteosarcomatous change of the pleomorphic adenoma.
The patient's symptoms were improved. Because the tumor had a malignant nature, the adjuvant radiotherapy (54 Gy) was done 4 weeks after surgery. At outpatient clinic for follow-up, we checked the orbital MRI 6 months after discharge. And the positron emission tomography was performed 3 months later. The evidences of recurrence and distant metastasis were not detected during 16 months postoperatively.
DISCUSSION
Masses of the lacrimal gland are generally differentiated from a wide spectrum of two groups, including epithelial origin and non-epithelial origin. The group of the epithelial origin include metastatic cancer, primary epithelial tumors, and the group of the non-epithelial origin have inflammatory lesions, lymphomas. The diseases in inflammatory lesions are chronic dacryoadenitis, reactive lymphoid hyperplasia, sarcoidosis, and lipogranuloma6). Metastatic lesions are uncommon, but can be found especially in breast, lung and unknown primary sites3). Font et al.3) reported that the incidence of non-epithelial origin is higher than that of epithelial origin, but the occurrence of these groups are controversial51015).
Pleomorphic adenoma is the most common benign epithelial tumor of the lacrimal gland35781316). The pleomorphic adenoma is called a "benign mixed tumor". The features required for diagnosis is that it is composed of both benign epithelial and mesenchymal tissue. The ductular epithelium based on structural characteristics form the lacrimal duct and the surrounding myoepithelial cells composed myxomatous mesenchyme1419). Several authors14691418) reported that the LGPA should be removed intact and completely to reduce the risk of recurrence and malignant transformation. The malignant transformation of LGPA is rare (6.25-8.6%)14). When the malignant transformation occurs, the malignant component is mostly carcinoma123456781011141516192122). With these characteristics, the AJCC named the CEPA12).
The pleomorphic adenoma with malignant transformation of the stromal component is extremely rare. Bernardini et al.2) reported that there was the carcinosarcoma, which was called a "true malignant mixed tumor" and composed of both malignant epithelial and mesenchymal tissue. In our review, only 6 cases of the carcinosarcoma have been reported3711171920). Furthermore, cases with malignant change of only the stromal component were more extremely rare. Because of these differences in the incidence, there was the name of CEPA, but the sarcoma ex pleomorphic adenoma (SEPA) was not named in the AJCC12).
In our case, it is not difficult to dissect the tumor from the surrounding periorbital membrane. The pleomorphic adenoma is a well-demarcated tumor. Even if malignant change occurs, the extension to surrounding tissue and distant metastasis is rare11222). CEPA is divided into three subtypes, non-invasive, minimally invasive (<1.5 mm from the capsule), and invasive carcinoma (>1.5 mm from the capsule)241219). Our case showed non-invasion into the capsule, and invasion to surrounding tissue and distant metastasis were not visible.
When the malignant transformation occurred, the patient showed a progressive worsening of symptoms, such as exophthalmos and ptosis, and the tumor size was increased1616172022). Malignant transformation is usually portended by the onset of rapid growth after a slow growth or non-growth9). Likewise, our patient presented progressive worsening of symptoms and an increase in the tumor size after a slow growth or non-growth of about 30 months.
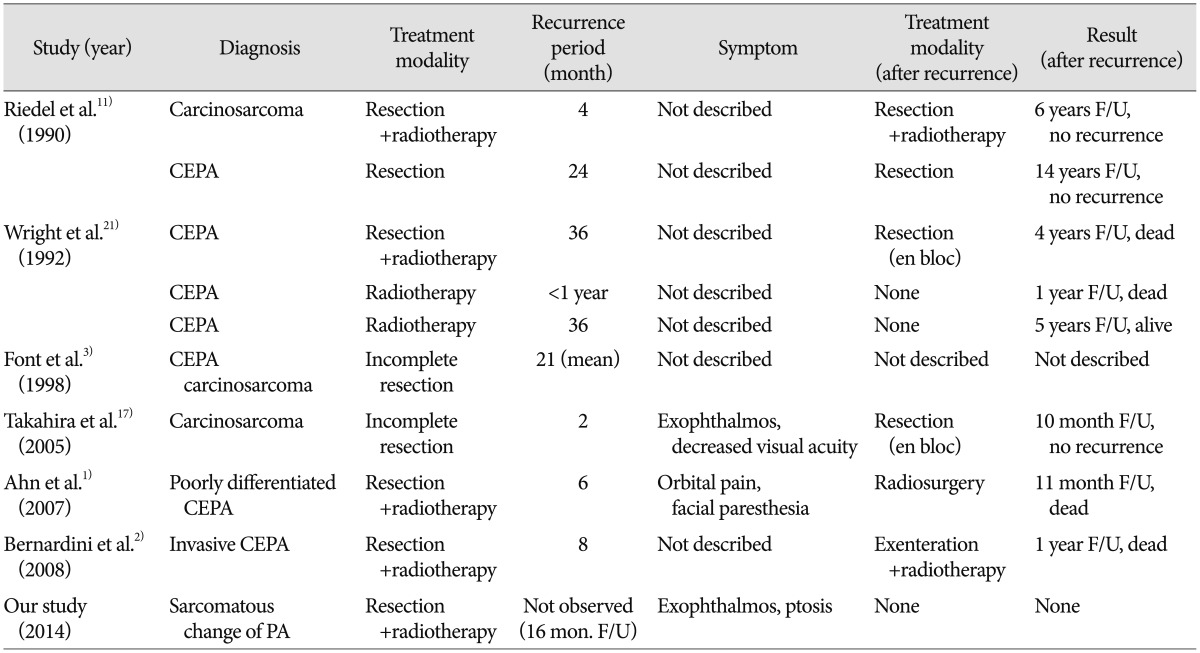
Because of the malignant component, we performed the radiation therapy postoperatively, although we did a total resection enough to identify the normal lacrimal gland in pathologic findings. The postoperative radiation therapy was done in several cases of the CEPA and carcinosarcoma12111321). The postoperative radiation on the local control in CEPA of the parotid gland was effective2). However, due to the low incidence of the CEPA and carcinosarcoma in the lacrimal gland, the effect of the postoperative radiation therapy has not been reported. And the time to recurrence, treatment modality after recurrence, and their results were not studied definitely (Table 1).
CONCLUSION
The pleomorphic adenoma with osteosarcomatous change is extremely rare and no treatment method has been established. If the tumor was well-demarcated mass, the total removal of the tumor as possible should be done. Furthermore, we should consider the adjuvant therapy for the tumor with malignant features. And it is necessary to follow up for detection of the recurrence and distant metastasis.
 XML Download
XML Download