

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Penetrating neck wounds caused by bullets or sharp tools account for 5% to 10% of all injuries3). Without appropriate care, the injury can cause death; thus, penetrating neck injuries are among the most critical injuries. The neck comprises several complex structures including the distal carotid artery, vertebral artery, parotid gland, pharynx, the ninth through twelfth spinal cord segments, and a cranial nerve located between the mandible and skull base. Exposure of these anatomical structures is challenging and risky; therefore, unless significant complications are expected, surgical excision is not recommended owing to the risk of surgical complications.
In this case report, we describe a foreign body embedded in the neck for a long period of time that was diagnosed radiographically, and we provide a review of the relevant literature.
CASE REPORT
A 59-year-old man donated a kidney 8 months prior to evaluation. He later reported a foreign body sensation in his neck, mild to severe cervical, shoulder, and chest pain, as well as tinnitus. He described the tinnitus as a "ssuk-saek" sound, and the symptom worsened when the patient turned his head. Pure tone audiometry was normal in both ears, at 10 dB in the right ear and 12 dB in the left ear. However, there was high tone loss in the 4 kHz to 8 kHz range, and tinnitus in the right ear at 50 dB and in the left at 30 dB. An evoking otoacoustic emission test of transient tone revealed that the average radiating sound intensity was 8.4 dB in the right ear and 2.5 dB in the left ear. The 0-6 kHz reproducibility was 90% in the right ear and 76% in the left ear. The converted otoacoustic emission test had a lower response in the left ear. A laryngeal exam revealed arytenoid edema and pseudosulcus of the true vocal cord.
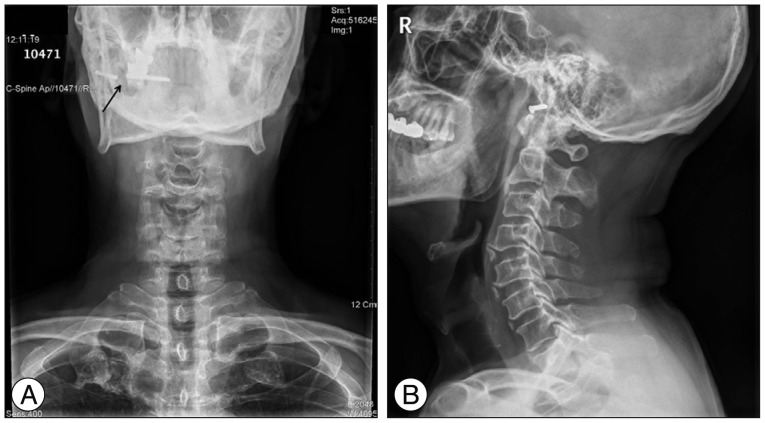
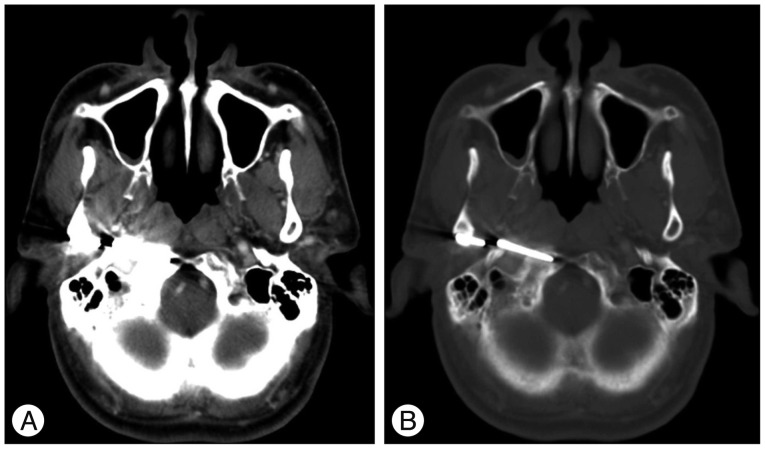
We suspected laryngopharyngeal reflux and prescribed lansoprazole (30 mg, 28 days), but the patient's symptoms did not resolve. Cervical computed tomography (CT) was performed, but no significant findings were noted. The patient was sent for evaluation by the neurosurgery department, and cervical disc disease was suspected. Subsequent cervical radiography and interpretation of previous CT data on a bone setting revealed a broken metallic foreign body 3-mm wide and 4.8-cm long within the right infratemporalis fossa (Fig. 1, 2).
We queried the patient further, and he recalled falling while holding a metal chopstick. The chopstick broke, but its tip was never found. After the accident, he reported no symptoms except momentary pain. There was no infection, edema, or severe neurologic deficit associated with the lesion; therefore, the foreign body was left embedded for several decades. The patient and his guardian declined surgical excision of the object and elected long-term monitoring.
DISCUSSION
In the field of otorhinolaryngology (head and neck surgery), an injury such as a foreign body embedded in the body because of carelessness or an accident is common. Foreign bodies can be surgically excised, but surgery has associated risks of complication and may require exploration of deep neck structures1).
Several reports have described that a fish bone lodged deep in the neck can be displaced into the thyroid gland, neck musculature, or parapharynx by deglutition movements or neck muscle contractions2,4,6,12,15). A previous study described a wire penetrating the piriform fossa into the thyroid gland towards the right posterior10), and there have also been reports of an external auditory canal foreign body infiltrating the jugular bulb and parapharynx9,14). Yet another report described the case of an infant who experienced mental deterioration and left hemiparalysis after falling while biting a chopstick despite a clear penetrating wound never being found8). Most prior cases of foreign body injury resulted from careless negligence, and the foreign body was usually surgically removed shortly after the injury occurred.
However, if a foreign body remains embedded for a long period of time, it may induce pressure damage and cause infection. Allergic reactions, granulomatous inflammation, tissue necrosis, and reactive lymph node proliferation may occur secondarily. In addition to the local histologic response, symptoms such as tinnitus, foreign body sensation, voice change, persistent neck pain, and odynophagia may occur.
Tinnitus is a significant symptom that commonly follows head and neck trauma because of auditory nerve, cochlea, tympanic membrane, or ossicular chain damage7). In the present case, the tinnitus worsened every time the patient turned his head, which may reflect neuromuscular alterations in the tissue surrounding the foreign body.
The infratemporal fossa (ITF) is located deep to the infratemporal crest, continues superiorly towards the temporal fossa and temporalis muscle, and inferiorly towards the parapharyngeal space. The osseous boundaries are the posterolateral maxillary surface anteriorly, the lateral pterygoid plate anteromedially, the mandibular ramus laterally, and the tympanic temporal bone and styloid process posteriorly. The ITF contains the maxillary artery, the trigeminal nerve mandibular branch, the pterygoid muscles, and the pterygoid venous plexus. Owing to its deep position, masses in the ITF may grow for a considerable time before symptoms occur, often delaying diagnosis. Access to the area is challenging, but adequate surgical exposure is critical for the excision of large ITF tumors13).
The ITF is divided into prestyloid and retrostyloid regions. The former contains facial and trigeminal nerves, and the latter contains the internal carotid artery, jugular foramen, and the ninth through twelfth cranial nerves5). A foreign body within the prestyloid process can cause trismus as well as mandibular and pharyngeal wall swelling. A foreign body within the retrostyloid process can cause systemic symptoms such as fever and chill.
In the case we described, there was no evidence of skull fracture or external injury, and the patient could not recall the traumatic event; the foreign body likely resided in the tissue for an extended period of time. The location adjacent to the bone structure may have delayed diagnosis; the foreign body was revealed only after switching the cervical CT data to a bone setting. In a similar case report, a mysterious transverse sinus foreign body remained asymptomatic for over 20 years11).
Because the foreign body was made of metal, suppurative inflammation typical of organic material such as wood was absent; only cervical lymph node reactive proliferation was observed. Moreover, the patient experienced only mild symptoms, and he and his guardian declined surgical excision. Leaving the foreign body embedded is preferred over infratemporal fossa exposure, due to the risk of considerable neurologic and vascular complications.
In a neck injury patient experiencing nonspecific symptoms, a thorough otolaryngologic history, physical examination, and radiography or computed tomography can enable diagnosis. Furthermore, the foreign body can remain embedded in the body without major somatic damage; however, routine monitoring is needed.
CONCLUSION
We reported the rare case of metallic chopstick embedded in the neck for several decades, and tried to find out the possibility of correlation with tinnitus and foreign body sensation. We also presumed the entrance pathway of foreign body into infratemporal fossa.
We assumed that careful history taking, detailed physical examination, and proper radiologic study may important tool for detection and evaluation of foreign body, which is located in important structure of our body.
 XML Download
XML Download