

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Currently endoscopic third ventriculostomy (ETV) is the first choice for obstructive hydrocephalus because of the quality of the endoscopic instrument and imageology10), it had yielded excellent results. This approach has been used for infantile obstructive hydrocephalus, but the treatment effect is still unclear. We retrospectively reviewed seventeen infants with hydrocephalus who were treated in our department by ETV from Jul. 2009 to Jun. 2013.
MATERIALS AND METHODS
Patients
This study included 17 patients between the ages of 51 days and 337 days, with an average age of 143 days, 9 males and 8 females, 4 Han people and 13 Hui people. Of the 17 patients there were 5 cases with encephalitis history, 2 cases with cerebral hemorrhage, and 10 cases of congenital hydrocephalus. Among the 10 cases with congenital hydrocephalus, were congenital aqueductal stenosis in 6 cases, Chiari malformation in 2 cases, and Dandy walker syndrome in 2 cases. Cine phase contrast magnetic resonance imaging (PC cine MRI) scan shows obstructive hydrocephalus in all cases.
Surgical technique
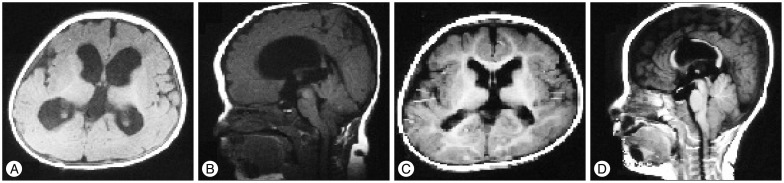
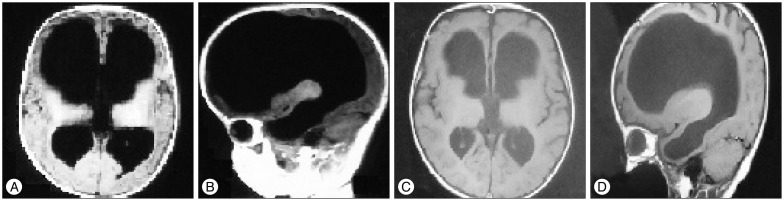
Surgery is carried out in a neurosurgical operating suite under general anesthesia. The patient is placed supine and the head is elevated 20-30° to minimize excessive cerebral spinal fluid (CSF) loss. A hook incision is made in the scalp 3 cm in diameter just lateral to the midline and anterior to the coronal suture. After a burr-hole approximately 1 cm diameter is created in the frontal bone, the dura is opened in cruciate fashion and the edges are suspended. A No. 14 peel-away catheter is then used to cannulate the frontal horn of the lateral ventricle. The endoscope is then passed through the catheter into the frontal horn. The foramen of Monro is located by following the choroid plexus, septal veins, and thalamostriate veins, and the endoscope is passed through this opening and placed into the third ventricle. Once the endoscope is in the third ventricle the cast shadow of basilar artery/posterior cerebral artery, the infundibular recess, and the bilateral mamillary bodies can be observed (Fig. 1A). Fenestration is performed in the slight avascular area at the midway between the infundibular recess and the mamillary bodies (Fig. 1B). A special tongs type grab is used for fenestration, and the edges of the orificium fistulae in 5 mm diameter are then coagulated. The Lilliquest membrane is opened through the orificium fistulae under the endoscope so that there is full communication between the third ventricle and the basal cistern (Fig. 1C, D). After exploring pulsation of the basilar artery and posterior cerebral artery through the orificium fistulae the endoscope is withdrawn. While repeatedly rinsing with 0.9% NaCl, a latin sponge is used to close the punctured pathway and the dura is sutured tightly, mending the periosteum if necessary, and the skull is closed. After surgery all the cases were subjected to oral antiepileptic drugs to prevent seizures. No dehydrant was used. Multiple (2X-3X) lumbar puncture was performed for a period of 7 days in order to promote CSF circulation, release hemorrhagic CSF, and alleviate the discomfort. CT or MRI was performed 7 days and 30 days after surgery to explore the narrowing of the ventricular system (Fig. 2, 3).
RESULTS
Treatment effect
Of the 17 postoperative infants the skull and ventricular system of 7 cases shrank : 1 case with encephalitis history, 1 cases with cerebral hemorrhage, 4 cases with congenital aqueductal stenosis, and 1 case with Chiari malformation, yielding an effective rate of 41.2%. 1 case failed because of severe ventricle inflammatory adhesion, excessive exudation, and vague basilar artery. In the remaining 9 cases whose ventricles were unchanged, ventriculoperitoneal shunt was performed for 4 cases, 5 cases gave up the further operation.
Intraoperative and postoperative complications
Intraoperatively, 2 cases with small artery hemorrhage were repeatedly rinsed with 0.9% NaCl and the bleeding gradually stopped. Four cases developed fever and the temperature returned to normal after expectant treatment. Six cases which developed subdural fluid accumulation which disappeared one month later.
DISCUSSION
The causes of infantile hydrocephalus
It is thought that the ventricular system may develop at an important and specific embryonic time period of neural stem cell proliferation and differentiation in the brain. There are many factors influencing the incidence of infantile hydrocephalus7) such as : asphyxia in perinatal period, hypoxic ischemic encephalopathy, intracranial hemorrhage, premature birth, hyperbilirubinemia, and perinatal infection; the genetic factors can not be excluded as well11).
Gansu province is located in the upper region of the Yellow River in northwestern China. It has a population of 26 million (2009) and has a large concentration of Hui Chinese in Linxia Hui Autonomous Prefecture. In this study we noticed that most infants with infantile hydrocephalus were Hui Chinese from the Linxia area (68.4%). Very recently a specific clinical syndrome or genetic cause was found to correlate with infantile hydrocephalus in a minority in United States (they did not mention which syndrome it is)8). This scientific result inspires us to investigate the possible etiological factors for Hui Chinese in Gansu China in our future work. The second cause we feel it important is Hui Chinese have an early marriage and pregnancy custom. For these 13 cases, the average maternal ages are only 17.2 years old to give birth, this might be consistent with most research believed maternal component is a significant cause for infantile hydrocephalus4).
The treatment effect of ETV
Currently ETV is the first choice for CSF shunt therapy in patients with obstructive hydrocephalus; additionally, the prevailing view is that it can be applied to communicating hydrocephalus9). It thereupon popularizes ETV to infantile hydrocephalus and congenital hydrocephalus, but the effect is still controversial. Some scholars2,6) believe that it is not suitable for infants younger than 2 years old, especially under 1 year old due to the incomplete absorption system of CSF, the orificium fistulae is reclosed, or new membrane formed postoperatively. In 2008 Lipina et al.3) reported that 14 patients under 6 months that presented with obstructive hydrocephalus were treated with ETV. The etiology of hydrocephalus was congenital aqueduct stenosis in five patients, posthemorrhagic obstruction in eight patients, and combination of posthemorrhagic and postinfection in one patient. They recommend ETV as the method of choice in children younger than 6 months of age. In 2010 Ogiwara et al.5) investigated 23 patients younger than 6 months that presented with obstructive hydrocephalus and were treated endoscopically. The etiology of hydrocephalus was congenital aqueduct stenosis in 11 patients, posthemorrhagic obstruction in six patients, myelomeningocele in two patients, postmeningitis in two patients, Chiari I malformation in one patient, and Dandy walker variant in one patient. ETV was successful in eight patients with regression of intracranial hypertension. Ventriculoperitoneal shunt implantation was required in the remaining 15 patients. Total success rate was 34.8%. In patients younger than 3 months of age, success rate was 25.0%. In patients from 3 to 6 months of age, success rate was 45.5%. Based on the above data, ETV should be the first method of choice for hydrocephalus in children younger than 6 months of age, especially in patients older than 3 months of age. Gallo et al.1) reviewed 23 patients younger than 6 months and without a previous history of shunting underwent ETV in their institution between 2003 and 2009. Total success rate was 39.1%. In the successful cases, median age was 140 days, whereas in the unsuccessful cases it was 47 days. The difference between the two groups was statistically significant (p=0.01). The impact of age on ETV failure in infants is clear. The patients' basic body situation should be taken in consideration before the ETV performed, such as age, the tolerance of a ventriculoperitoneal shunt, and the incident rate of complications. In our study of 17 patients, 7 cases improved remarkably : their heads and ventricles shrank, cerebral cortexes thickened morphologically. The ventricles of the remaining cases were unchanged. Our follow up confirms ETV is the best choice for infantile obstructive hydrocephalus.
The advantages and disadvantages of ETV and indications
Compared with a ventriculoperitoneal shunt, ETV has its own advantages : no foreign object (shunt tubing and valve) implanted in the body thus avoiding the catheter related complications such as shunt occlusion, infection, over drainage, abdominal complications, the danger of an infant's thin skin being punctured by catheter, and need for shunt revision with increased age. After accept ETV, the CSF is close to the physiologic circulation, meanwhile, some other procedure can be done intraoperatively : pellucid septostomy, aqueductoplasty, cyst fenestration, etc. Most scholars believed ETV is the best choice for obstructive hydrocephalus. Our data showed there are fewer postoperative complications, less bleeding, fever, and subdural collection of fluid after surgery.
In summary, because of their thin skin and younger age the treatment of infantile hydrocephalus is very difficult. Considering all the benefits mentioned above, we conclude ETV is the best treatment choice for infantile hydrocephalus. We will explore the possible pathogenic factors for infants in future studies so we can avoid or prevent hydrocephalus occurred early.

 XML Download
XML Download