

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In 1953, Seldinger17) introduced the percutaneous vascular access technique, and the common femoral artery (CFA) is the main access site for angiography and interventional procedures11). CFA is considered appropriate because it has a relatively large diameter, is located superficially and can be easily compressed to achieve hemostasis8,9). The incidence of vascular access site complications is 0.44-1.8% during diagnostic angiography and up to 4% during interventional procedures2,10,18). Puncture sites that were not located in the CFA were associated with a higher rate of local vascular complications2,11,6,18). If the puncture site was too low, there was an increase in the incidence of pseudoaneurysms, hematomas, arteriovenous fistulas, or limb ischemia2,9,12,19). If the puncture site was too high, there was an increase in the incidence of retroperitoneal hemorrhage5,6,9,18,19). There is little data about the CFA anatomy during percutaneous angiography especially in Korean subjects. The aim of this study was to assess 1) the CFA anatomy and the influence of demographic and other clinical factors on the common femoral artery diameter and length, and 2) the anatomical relationship between the CFA and femoral head.
MATERIALS AND METHODS
Patients
We retrospectively collected the angiograms of 144 consecutive cases, which were performed by a single physician, and hospital records of the patients, who underwent diagnostic cerebral angiography from January 2011 to August 2011. During this period, 114 cases underwent cerebral angiography via the femoral access and 30 cases underwent cerebral angiography via the radial access. Among the 114 femoral angiograms, 109 femoral angiograms were included because one patient did not undergo femoral angiography; and in two patients, femoral angiography was performed at the same side repeatedly. In two patients, femoral angiography was performed separately for both sides; and in these cases, data of the right side were used. Demographic data were also obtained from the medical records.
Procedure
We marked the inferior border of the femoral head with a hemostat under fluoroscopy and identified the arterial pulse just above the hemostat tip marking. Arterial access was obtained with 18-G needle using the modified Seldinger technique. The needle was inserted at an angle of about 45° from the skin just below the level of the center of the femoral head. After arterial sheath placement, we performed a routine cerebral angiography. Femoral angiography was performed through the arterial sheath before closure of the puncture site. To avoid parallax error during angiography, biplane femoral angiography was performed with the femoral head at the center of the screen in the anteroposterior and oblique 60° projections. After performing femoral angiography, we achieved hemostasis with the use of a closing device or manual compression. The above procedure is routinely performed at our institution during transfemoral cerebral angiography.
Definitions
As demonstrated by Yanganti et al.19) we divided the femoral head into four equal zones (1-4) in a craniocaudal direction. The zone above the femoral head is zone 0, and the zone below the inferior border of the femoral head is zone 5 (Fig. 1A). The lowest position of inferior epigastric artery (IEA) loop and the point of common femoral artery (CFA) bifurcation were identified in the biplane angiogram (Fig. 1B). The contrast-filled opacified sheath was used as the scaling reference and calibrated for precise measurement in each case. The lowest margin of the intraperitoneal space was indicated by the IEA loop. Angiograms were reviewed by the authors who were blinded to patient data. The luminal diameter of the CFA was measured around the center of the femoral head. The length of the CFA was measured from the IEA loop to the bifurcation point of the CFA in a straight direction along the vessel. Internal carotid artery (ICA) stenosis group was defined as the group that showed more than 50% stenosis of the intra/extracranial ICA.
Statistical analysis
Categorical variables are expressed as percentages, and were analyzed by the chi-square and Fisher's exact tests. Continuous variables, such as anatomy of the CFA, were checked for normality and transformed (e.g., log transformation) if necessary. Descriptive characteristics are expressed as means (SD), medians (interquartile range), and were analyzed by the Student's t-test or Wilcoxon rank sum test. The Spearman correlation coefficient was used to analyze the influence of age, height, weight, body surface area (BSA) according to Du Bois's formula (BSA m2=weight0.425 kg×height0.725 m×71.84) on the anatomy of the CFA (diameter and length). Association was found between the anatomy of the CFA and sex, diabetes mellitus, hypertension, dyslipidemia, history of smoking by the Student's t-test, Wilcoxon rank sum test, and Kruskal-Wallis test. Linear regression analysis was used to test the relationship between independent variables and the anatomy of the CFA. Diameter of the CFA with skewed distributions was entered into univariate and multivariate regression models after log-transformation of the data. A multiple linear regression model was constructed, which included variables with a p≤0.05 in the univariate analysis, and height and weight were excluded from the model to avoid multicollinearity. A probability value of 0.05 was considered as the limit of statistical significance. All analyses were performed using SAS software, version 9.3 (SAS Institute, Cary, NC, USA).
RESULTS
Patient characteristics
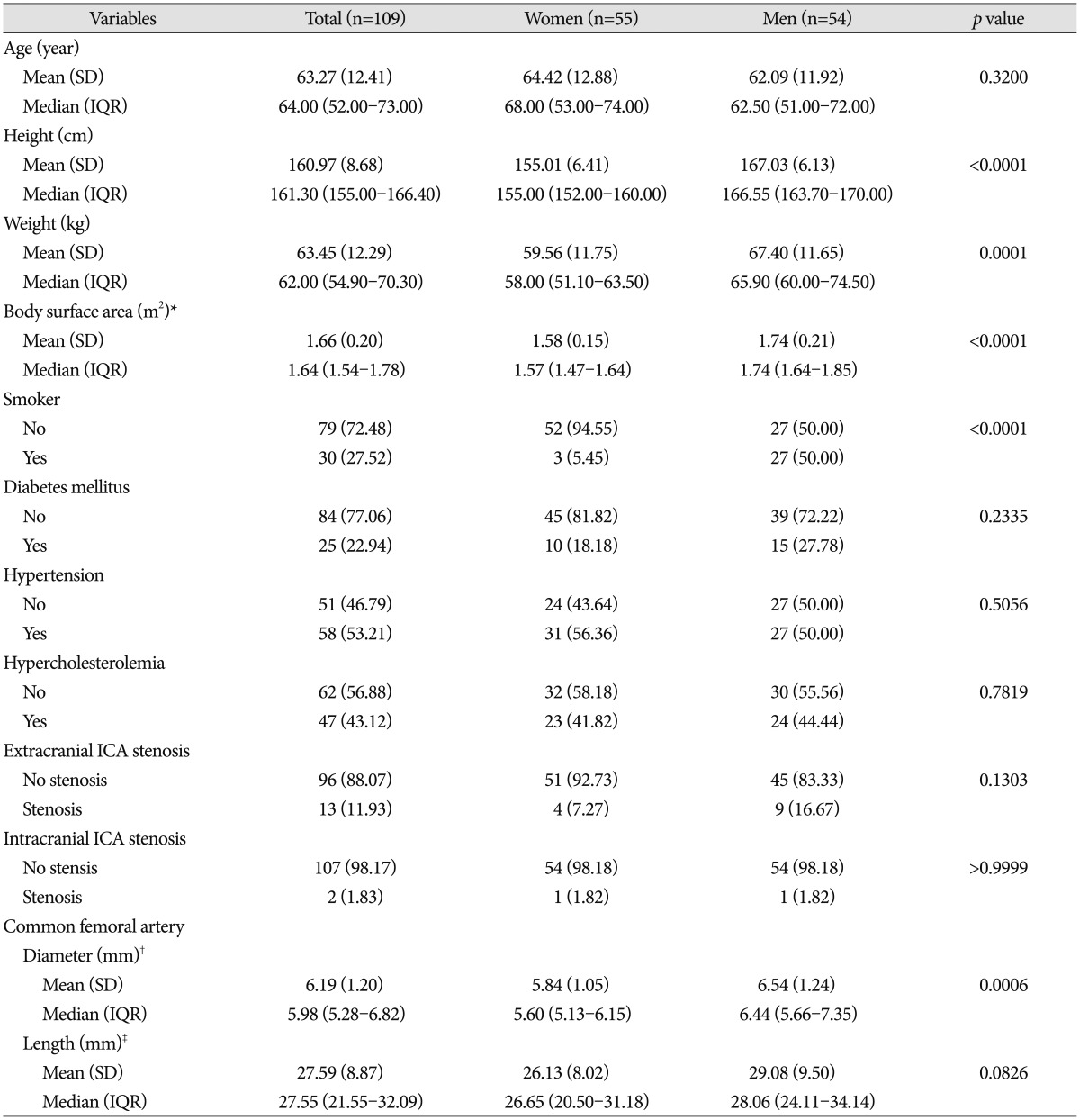
Finally, 109 femoral angiograms of patients (mean age, 63.27 ±12.41 years) were included in this analysis (Table 1). There were 55 female patients (mean age, 64.42±12.88 years) and 54 male patients (mean age, 62.09±11.92 years). The right femoral angiography was performed in 104 of these cases. The length of the CFA was 27.59±8.87 mm (range, 6.44-57.62 mm). The luminal diameter of the CFA was 6.19±1.20 mm (range, 4.34-10.27 mm). Height, weight, BSA, as well as CFA diameter were significantly greater in men than in women (p<0.05). There were no differences between women and men in terms of age and other risk factors (diabetes mellitus, hypertension, hyperlipidemia) except for smoking (p<0.05). The luminal diameter of the CFA was 6.54±1.24 mm in men and 5.84±1.05 mm in women (p<0.05). The length of the CFA was longer in men (29.08±9.50 mm) than in women (26.13±8.02 mm), but this difference was not statistically significant.
Correlation between anatomy of the CFA and clinical factors
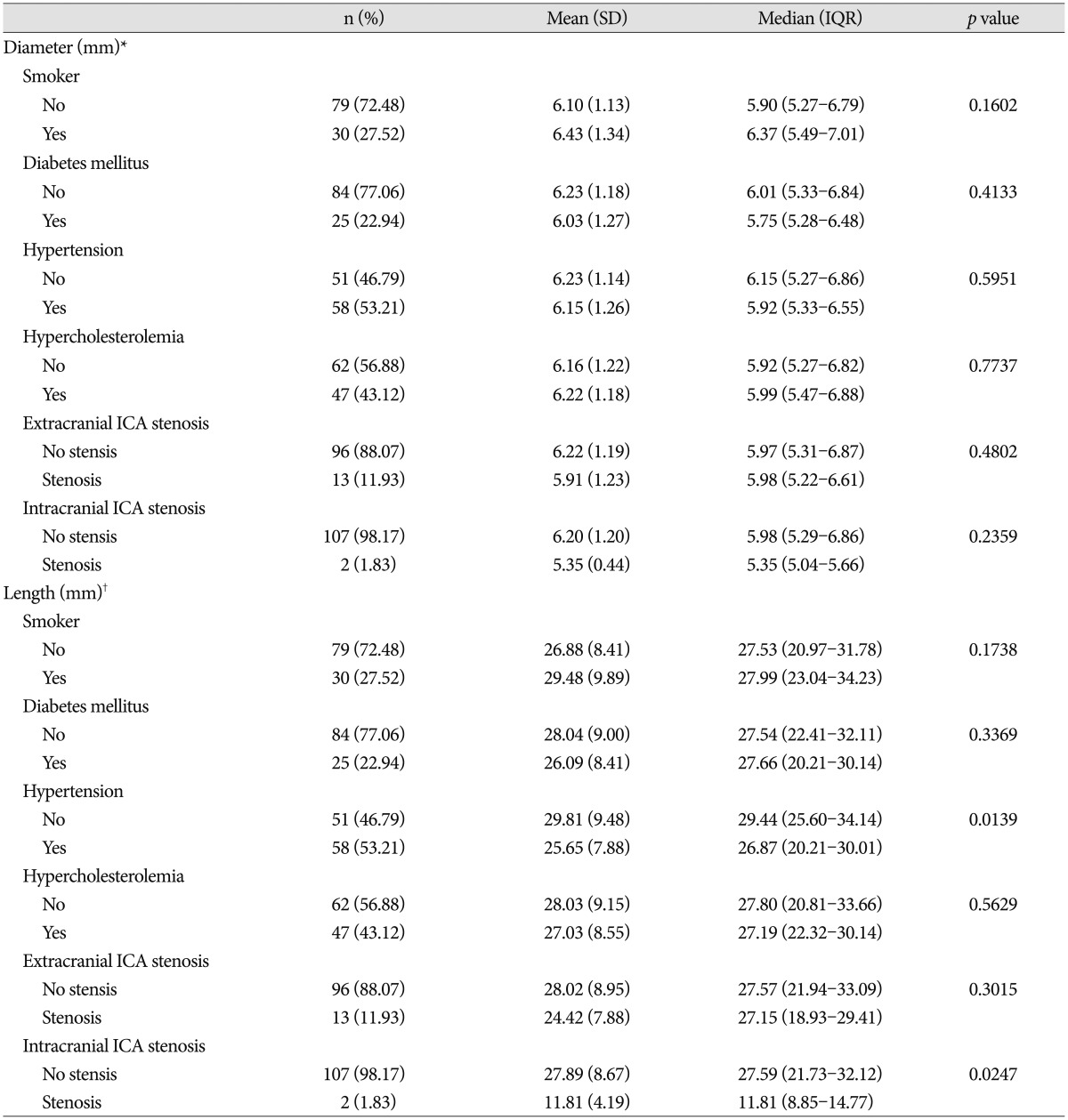
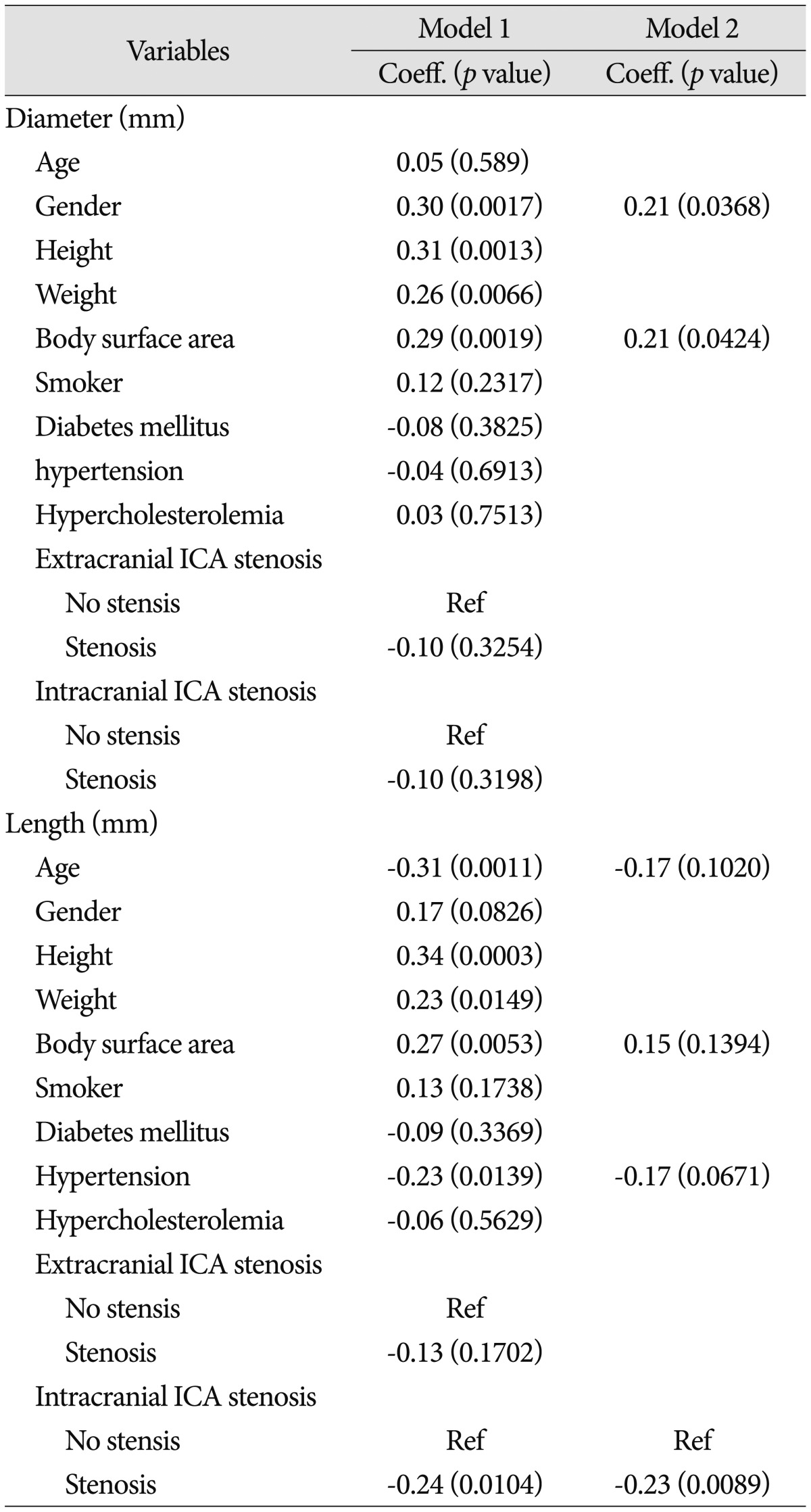
No significant correlation was found between the diameter of the CFA and the other clinical risk factors (Table 2). A significant correlation was found between the diameter of the CFA and body height (r=0.34; p=0.0003), body weight (r=0.31; p=0.0012) and BSA (r=0.34; p=0.0002). A very similar strong positive correlation was found between the length of the CFA and body height (r=0.33; p=0.0005). Body weight (r=0.23; p=0.0005) and BSA (r=0.28; p=0.0037) showed a weak positive correlation with CFA length (Table 3). Multivariate regression analysis showed that gender and BSA were independent predictors of diameter of the CFA (p<0.05) (Table 4).
Anatomy of the CFA in relation to the femoral head
All of the IEA loops were located above the center of the femoral head. The IEA loop was found in zone 0 (n=11, 10.09%), zone 1 (n=67, 61.47%), and zone 2 (n=31, 28.44%) (Fig. 2A). The point of CFA bifurcation was found in zone 1 (n=2, 1.83%), zone 2 (n=3, 2.75%), zone 3 (n=11, 10.09%), zone 4 (n=40, 36.70%), and zone 5 (n=53, 48.62%) (Fig. 2B). Actual puncture sites were located in zone 2 (n=9, 8.26%), zone 3 (n=72, 66.06%), and zone 4 (n=28, 25.69%) (Fig. 2C). In 106 cases (97.2%), the puncture site was located between the IEA loop and the bifurcation of CFA above the femoral head.
DISCUSSION
Vascular access site complications are one of the most frequent complications after percutaneous angiography and interventional procedures2,18). The factors that influence these local complications are thought to be old age, female gender, lower BSA, status of the peripheral vasculature, type of procedure, use of anticoagulation, and technique of arterial puncture and subsequent vessel closure10,13,14,16,18). To reduce these vascular complications we should consider the vascular anatomy and try to identify the optimal puncture location.
In our study, the mean CFA diameter was 5.84±1.05 mm in women and 6.54±1.24 mm in men. This gender difference is similar to that in a study of 200 patients16) and other studies3,15). The mean CFA diameter was 6.19±1.20 mm, and this diameter was 0.5-1 mm less than that in studies conducted in the Western population15,16) and other Asian populations3). The mean length of the CFA was 26.13±8.02 mm in women and 29.08±9.50 mm in men. This length of the CFA was shorter than that in the other study16). This discrepancy in the finding may be due to patients' characteristics and the definition of CFA length with an imaginary line drawn between the pubic tubercle and the anterosuperior iliac spine as the proximal end of the CFA in other study16). Sherev et al.18) described that the IEA rarely overlapped the acetabulum, and most frequently it was located at least 10 mm away from the most superior border of the acetabulum. Yaganti et al.19) reported that in 11.9% (75/631) of the patients, the IEA loop was located in a much lower position, even below the center of the femoral head (FH). In our study, the IEA loop was found in zone 0 (n=11, 10.09%), zone 1 (n=67, 61.47%), and zone 2 (n=31, 28.44%). If we consider that the ideal puncture site is between the loop of IEA and bifurcation into the PFA and SFA on the femoral head, the CFA length for an ideal puncture is shorter than the real CFA length. In our study, none of the patients had an IEA loop below the center of the FH. This finding was not in accordance with that in the study by Yaganti et al.19). The cumulative probability of being above the loop of the IEA can be determined in our study according to the puncture zone (Fig. 3A). The proportion of cases, in which the location of femoral artery bifurcation was above the center of the FH, was 4.59% (5/109), and the proportion of cases, in which the location of femoral artery bifurcation was in zone 3, was 10.09% (11/109). This finding is very similar to that in the other study : 4.4% (28/631) and 10% (63/631), respectively19). The cumulative probability of being below the bifurcation of the CFA was determined in our study (Fig. 3A).
The most widely used puncture site identification methods are the traditional anatomic landmark guidance and fluoroscopic visualization9). A study by Grier and Hartnell8) revealed that inguinal skin crease as a landmark was distal to the bifurcation of the common femoral artery in 71.9% of limbs8). A study by Fitts et al.7) show-ed that puncture under fluoroscopic guidance results in significantly less pseudoaneurysm formation and arterial injury. A study by Abu-Fadel et al.1) reported that although the incidence of access site complications was not different, fluoroscopic guidance has the potential to decrease complications due to low arteriotomy without increasing the risk of retroperitoneal bleeding. Theoretically, accurate puncture of the common femoral artery can be performed under ultrasonic guidance by direct visualization; however, the ultrasonic guidance group did not show a significant difference in the rate of local complications4,14). This study only showed that in obese patients or patients with weak arterial pulse, the puncture time and number of attempts were reduced4). Ultrasonic guidance technique should keep the maintence of sterility and need additional equipment. Moreover, some physicians are not familiar with ultrasonography.
The incidence of access site complications decreases when the puncture site is optimally located between the IEA loop and CFA bifurcation14,18). Actually, the target zone area for puncture can vary according to the IEA loop position and CFA bifurcation. Patients with a low position of the IEA loop and high CFA bifurcation, the so called short target zone patients have a high probability of developing access site complications. Our study showed that if we try to obtain an arterial access with fluoroscope guidance, while targeting just below the center of FH (zone 3), the cumulative probability of being outside the target zone is the lowest (Fig. 3B). There are very rare chances of retroperitoneal hemorrhage and about a 15% probability of being below the bifurcation of CFA. But, the actual puncture point could be outside the range than expected as in our cases. To overcome this problem, we should consider the accurate position of the center of the fluoroscope during detection of the femoral head and the actual gap between skin and arterial puncture point according to patient factors (e.g., obesity/thin).
Our study is limited by its small sample size and retrospective design. We need to perform a large prospective study for further analysis.
CONCLUSION
The diameter of the CFA is smaller in Korean subjects than in Western subjects. Females and patients with a small BSA have a smaller diameter of the CFA. The fluoroscopic guided puncture just below the center of the FH may help to achieve ideal puncture location between the lower margin of the IEA loop and CFA bifurcation.




 XML Download
XML Download