

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Foot drop is a symptom which presents an inability or weakness in the dorsiflexor muscles of the ankle and the toe. It is mainly caused by neurological lesions of the lower motor neuron system, but upper motor neuron injury may also cause the symptom. As above, the most common lower motor neuron (LMN) pathology for foot drop is peroneal neuropathy, which often results from the compression at the fibular head. For other LMN pathologies, there are L4-5 radiculopathy, lumbar plexopathies, partial sciatic neuropathy and polyneuropathy1,4,5,6,9).
Less commonly, an upper motor neuron (UMN) lesion can cause foot drop, which involves the interhemispheric motor cortex, corona radiata, internal capsule, cerebral peduncle, medulla, or spinal pyramidal tract9). Isolated foot drop is very rarely caused by an upper motor neuron lesion3,4,5,6,8,9).
In this report, we present an extremely rare case of an isolated foot drop caused by focal cortical infarction of the motor cortex.
CASE REPORT
A 74-year-old male visited the outpatient department presenting a one-week history of right-side foot drop. The patient had no history of hypertension, diabetes, hypothyroidism, arthritis, cancer, hepatitis or stroke. He denied any recent traumatic accidents to the right leg. The complete physical evaluation was conducted, showing no abnormalities such as visual changes, fever, chills, dizziness, headache, or bowel or bladder problems. In the detailed neurological examination, he was well oriented and exhibited no signs of cranial nerve function disorders such as dysarthria, dysphagia or facial palsy. Distal pulse and sensation were intact in all extremities including the dorsal aspect of the right foot. Passive range of motion was in a normal range in every peripheral joint. The patient was also negative for the straight leg raise test and femoral nerve stretch test. No pathological reflexes were found bilaterally such as Babinski and ankle clonus, with normal deep tendon reflexes. Individual muscle strength tests were normal for all extremities except for the right tibialis anterior and the extensor digitorum. Muscle tone grades in the right tibialis anterior and extensor digitorum were 0/5 when measured by Modified Ashworth Scale.
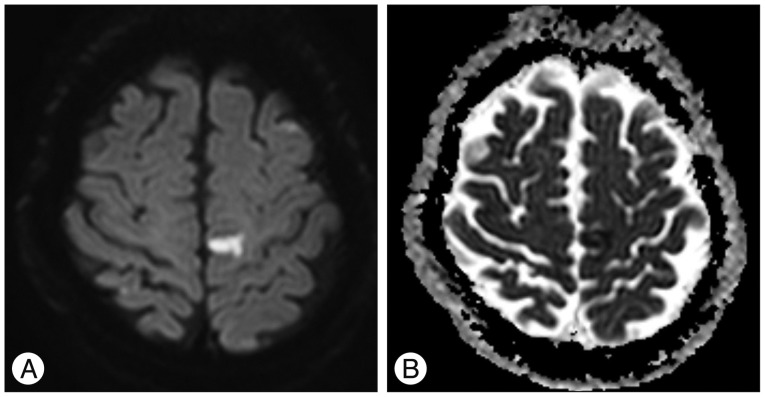
Electromyogram (EMG) and magnetic resonance imaging (MRI) were performed. EMG showed no remarkable findings and lumbar spinal MRI revealed a diffuse bulging disc at the L4-5 disc space level. However, there was no evidence of severe nerve root compression that was susceptible to current condition. Since the lumbar spinal lesions were ruled out for the patient's symptom, a brain MRI was performed to investigate any potential central lesions. Diffusion-weighted imaging (DWI) showed focal high signal intensity on the left upper motor cortex (Fig. 1A). An afferent diffusion coefficient (ADC) map revealed low signal intensity on the same area (Fig. 1B). Subsequently, the patient was diagnosed with subacute cerebral infarction. After one week of treatment with an anti-platelet agent and rehabilitation therapy, the patient's muscle power showed improvement in his right tibialis anterior and extensor digitorum, from 0/5 to 2/5.
DISCUSSION
Foot drop is defined as the weakness of an ankle or one of the toe's dorsiflexors; the tibialis anterior, extensor digitorumlongus, or extensor hallucis longus1,2,3,4,5,6,8,9). It is usually caused by LMN pathology that results from disruption of the deep peroneal nerve. Since the nerve is in contact with the 4th and 5th lumbar spinal nerve, peroneal neurophathy and L4-5 radiculopathy are the most common causes of foot drop4,9). Additionally, UMN pathologies can also cause foot drop. Since the motor components of the 4th and 5th spinal nerves are controlled by the primary motor cortex via the corona radiata, the internal capsule, the basal ganglia and the ventral gray matter of the spinal cord, any lesion along this neuronal pathway can be the UMN pathology of foot drop. However, since these UMN fibers are condensed and closed with many other functional neuronal fibers, isolated foot drop due to an UMN pathology is very rare3,6,8).
For the diagnosis of foot drop, detailed neurological examination and good anamnesis are essential. Sequential EMG and MRI findings were found to be correlated in 92% of foot-drop patients6). We performed an EMG study and spinal MRI to investigate a probable lesion such as peripheral neuropathy or L4-5 radiculopathy. But, none of the results were specific enough to explain the symptom. Although possible UMN lesions were not clearly indicated in previous examinations, showing no signs of abnormal reflexes of the Babinski reflex or ankle clonus, we a performed brain MRI in the interest of being thorough; the MRI revealed a diagnosis of subacute cerebral infarction which caused the foot drop.
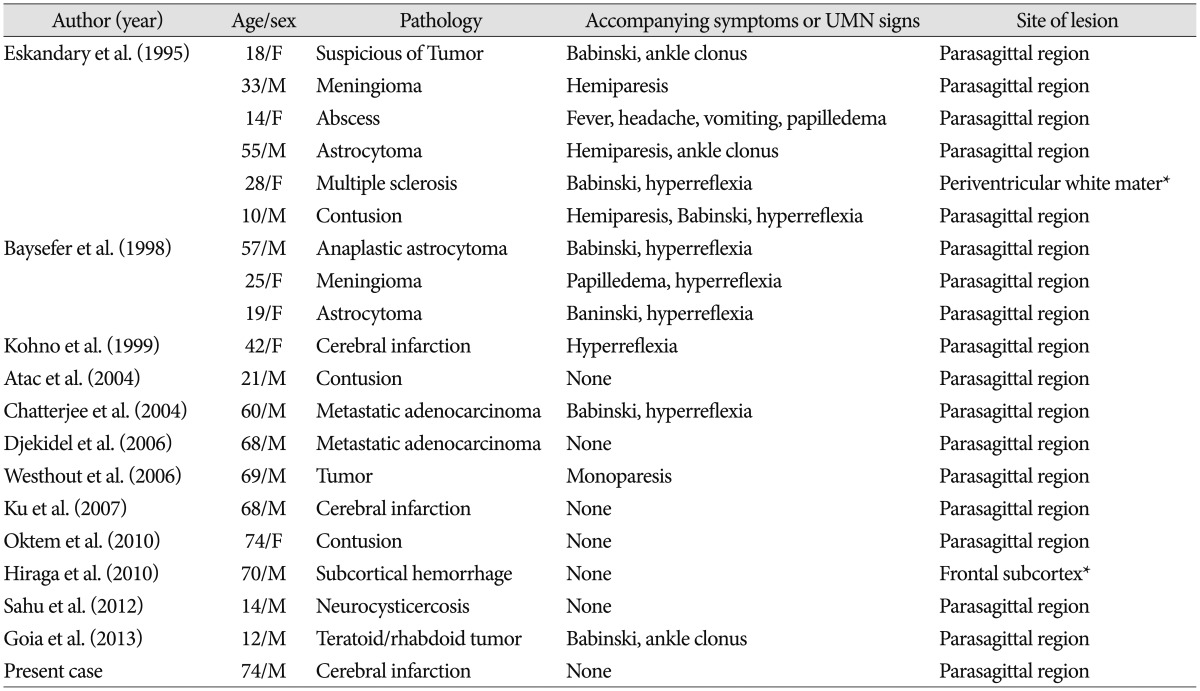
To our knowledge 19 cases of foot drop due to a central nervous system (CNS) lesion have been reported (Table 1). In these reports, various CNS etiologies were illustrated; brain tumors, metastases, contusion, infarction, abscess, multiple sclerosis, neurocysticercosis. However, the majority of pathologies were manifested in the parasagittal area1,2,4,5,6,8,9). Direct parasagittal damage or local mass effect on the parasagittal region can cause the foot drop, since the medial homunculus of the primary motor cortex at the mesial surface, adjacent to the supplementary motor area (SMA), or at the top of the lateral surface of the precentralgyrus are involved in ankle and toe movement5,9). Usually in the motor system, SMA is responsible for motor functions such as planning and initiation. Therefore, the lesions involving the SMA may cause astasia or apraxia rather than weakness. But, rarely it can cause motor deficits because the SMA proper transfers corticospinal efferences and is connected with the primary motor cortex7). There are only two previous reports on isolated foot drop caused by lesions other than parasagittal lesions1,3). In one of those cases, the lesion was within the corona radiata, which conveys neuronal impulses from the cerebral cortex of the primary somatotopic motor area to toe and ankle movement. According to these previous reports, lesions of the cortical surface are more likely to cause foot drop than deeper lesions. Because the descending motor axons are compacted into a small area by deeper lesions, foot drop due to the subcortical lesions are rarely reported3).
Patients with cerebral pathologies of foot drop usually have had UMN symptoms, such as Babinski reflex, hyperreflexia, and ankle clonus1). However, CNS pathologies can be found in some patients without any UMN symptoms, as seen in our case4,6,8). In such cases, diagnosis is delayed due to its atypical presentation which resembles a peripheral type of foot drop.
To our knowledge, this is the third report of unilateral isolated foot drop from a cerebral infarction. Brain MRI showed ischemic damage in the somatotopic ankle and toe motor homunculus.
CONCLUSION
We report a case of unilateral isolated foot drop caused by cerebral infarction. In the initial examination of said patient, it could be easily misidentified as a peripheral pathology or misdiagnosed as other irrelevant conditions. To avoid such mistakes, CNS evaluation should be considered if the lumbar MRI and EMG results are negative for the symptom. Even if the incidence is extremely rare, central isolated foot drop present without any UMN symptoms.
 XML Download
XML Download