

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic encapsulated intracerebral hematoma (CEIH) is a rare cerebrovascular disease that behaves as a slowly expanding lesion with a gradual onset9,10,11,12,13,14,15,16,17,18). It is well established that CEIH is associated with arteriovenous malformations; however, CEIH associated with cavernous malformation (CM) is rare9,10,11,12,14,18). Herein, we report a case of CEIH associated with CM, and discuss its pathogenesis.
Go to : 
CASE REPORT
A 12-year-old female was admitted to our hospital because of a one-week history of progressive headache and nausea. She had no prior history of radiation therapy or surgery. She had a past history of a simple febrile seizure at 21 months of age, and a brain magnetic resonance imaging (MRI) study was performed on a 1.5 tesla device and was judged normal (Fig. 1). On admission, neurological examination showed no abnormality. A brain computed tomography (CT) scan and MRI on a 3 tesla device showed an intracerebral hematoma surrounded by edema in the right frontal lobe (Fig. 2A-D). One week later, her headache and nausea worsened, and a brain CT scan revealed the enlargement of hematoma (Fig. 2E). A right frontal craniotomy was performed. The capsule was opened at a depth of 1 cm from the cortex. The cavity was filled with brownish fluid hematoma similar to chronic subdural hematoma. A lobulated mass was also found on the capsule. The capsule, mass, and hematoma were totally removed (Fig. 2F). Histological examination confirmed the diagnosis of CM, and also revealed that the capsule consisted of an outer collagenous layer and an inner granulated layer with deposits of hemosiderin, which was compatible with CEIH (Fig. 3A, B). Immunohistochemical analysis revealed increased expression of vascular endothelial growth factor (VEGF) and the VEGF receptor (VEGFR)-1 in the endothelium and fibroblasts in the capsule (Fig. 3C, D). Postoperative cerebral angiography showed no abnormality. The postoperative course was uneventful and the patient was discharged without neurological deficit.
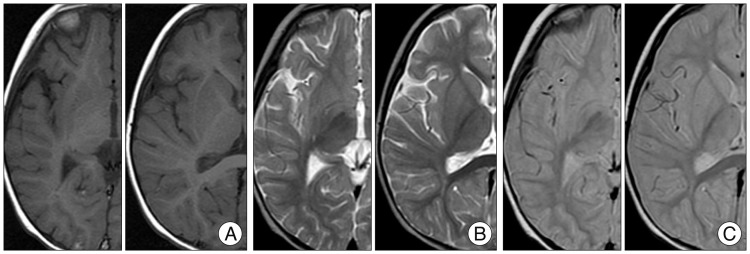 | Fig. 1Imaging findings at 21 months of age. Axial T1-weighted (A), T2-weighted (B), and proton density (C) magnetic resonance images show no evidence of any lesions.
|
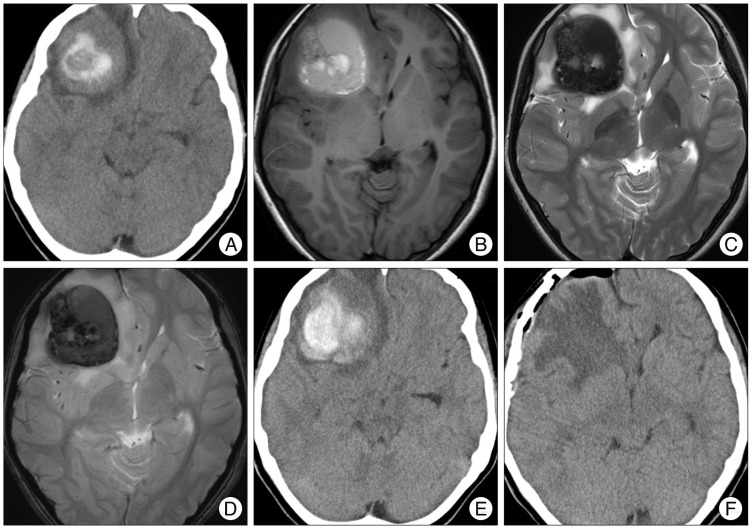 | Fig. 2Imaging findings during admission. A : Computed tomography (CT) scan on admission shows an intracerebral hematoma surrounded by edema in the right frontal lobe. B, C, and D : Axial T1-weighted (B), T2-weighted (C), and T2*-weighted (D) MRI reveal a mass lesion as mixed intensities. E : CT scan obtained one week after admission shows progression of hematoma. F : Postoperative CT scan shows total removal of the lesion.
|
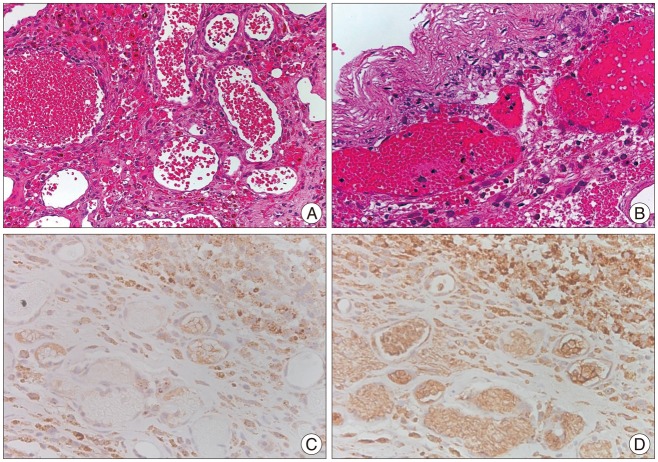 | Fig. 3Histopathological findings. A : Specimen (H&E) taken from the lobulated mass shows thin-walled dilated vascular channels with no intervening brain parenchyma, thus suggesting the presence of cavernous malformation. B : Specimen (H&E) of the capsule shows its structure consisting of an outer collagenous layer and an inner granulated layer with deposits of hemosiderin, which is compatible with chronic encapsulated intracerebral hematoma. C : Immunohistochemistry for vascular endothelial growth factor (VEGF) reveals positive immunostaining in the endothelium and fibroblasts. Original magnification : 400×. D : Immunohistochemistry for VEGF receptor-1 reveals positive immunostaining in the endothelium and fibroblasts. Original magnification : 400×.
|
Go to :
DISCUSSION
We previously reported that features of CEIH associated with CM patients included an adult male predominance, a high frequency of headache or seizure, a high frequency of involvement of frontal or parietal lobe, and high rates of presence of edema formation15). The present case had most of these features, except for age and sex.
Numerous studies of the natural history of CM have been reported over the years, most of which have documented hemorrhage rates ranging from 0.7% to 6% per patient-year19). Most hemorrhages attributable to CM are characterized by microhemorrhages and are seldom catastrophic or fatal. Most notably, supratentorial cavernous malformations leading to massive, life-threatening hemorrhages are rare entities6).
CEIH is characterized by the presence of a fibrotic capsule which histologically resembles the outer capsule of chronic subdural hematoma, and is thought to develop by chronic progressive growth due to repeated bleeding from the new blood vessels in the capsule9,13). The VEGF pathway has been implicated in CEIH as it can specifically regulate endothelial cell growth and differentiation, which may promote the enlargement of this type of hematoma13,15). VEGF binds two related receptor tyrosine kinases, VEGFR-1 and VEGFR-2. Nakamizo et al.13) reported that VEGF and VEGFR-1 were expressed in specimens of CEIH that developed after radiosurgery for arteriovenous malformation, and we also previously reported a case of CEIH associated with CM with high expression of VEGF and VEGFR-115). We reconfirmed that the activated VEGF pathway might contribute to development of CEIH in the present patient with CM.
The etiology of CM remains largely unknown, with some believing these lesions to be congenital while others consider them to be acquired4,7). It is known that CM may be induced by radiation therapy or radiosurgery11,20), whereas de novo formations of CM without previous radiotherapy are rare1,2,3,5,8). Recent studies have demonstrated that the endothelial proliferation induced by VEGF may also contribute to de novo formation of CM1,5). It is possible that CM developed de novo in the present case, however, we could not definitively confirm that hypothesis because the previous MRI had been performed on a 1.5 tesla device. Therefore, we could not precisely assess the relationship between the VEGF pathway and CM formation.
Go to :
 XML Download
XML Download