

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Paresthesia is a common manifestation of patients with neurologic problems. It is characterized by a burning, prickling or unpleasant sensation that is usually felt in the hands, arms, or legs but can also occur in other parts of the body, which sometimes leads to sleep disturbance. Paresthesia of limbs may occur from abnormalities in the peripheral nervous system, from direct compression of the peripheral nerve, or in the central nervous system. Lumbar spinal stenosis and lumbar disc herniation (LDH), or spondylosis may also occur when nerves were irritated, causing abnormal sensation in the legs. Hence, patients with leg discomforts visit spine clinics for identifying their spine problems. The restless legs syndrome (RLS) is also a common disorder affecting up to 5% to 15% of the general population, in which the incidence increases with age5,11,33,44), and includes paresthesia in the legs, that occurs at rest, and worsens in the evening, but improved by movements. Hemmer et al.21) reported RLS associated with myelopathy in one patient with a Borrelia induced myelitis and Zwartbol et al.51) presented patients with an acute acceleration of RLS due to cervical cord ischemia.
In our experience, many patients with RLS are sent to neurosurgeons or neurologists for evaluation of their spine or brain conditions, not sleep specialists for their sleep fragmentation. And, there are no clinical studies on patients diagnosed with RLS visiting spine clinics. The purpose of this study is to investigate the incidence of RLS in spine clinics, its relation to neural compromises using lumbar MRI and to review clinical approaches of this syndrome and its recent treatments.
Go to : 
MATERIALS AND METHODS
From January 2012 to December 2012, a total of 639 patients with leg discomforts had undergone spine magnetic resonance imaging (MRI) to determine whether they had certain spine problems. Among them, a retrospective medical record review was performed on patients with RLS who were diagnosed by National Institutes of Health with four essential clinical criteria based solely on symptoms in 2003 : 1) an urge to move the limbs with or without sensations; 2) improvement with activity. Many patients find relief when moving and the relief continues while they are moving; 3) worsening at rest. Patients may describe being the most affected when sitting for a long period of time, such as when traveling in a car, attending a meeting, or watching a TV; and 4) worsening in the evening or night. Patients with mild or moderate RLS show a clear circadian rhythm to their symptoms, with an increase in sensory symptoms and restlessness in the evening and into the night. Affected limbs were classified as five types according to analysis of enrolled subjects; A) below knees to feet, B) from proximal thigh to feet, C) both feet, D) both lower arms and lower legs, and E) asymmetric severity with unusual localization.
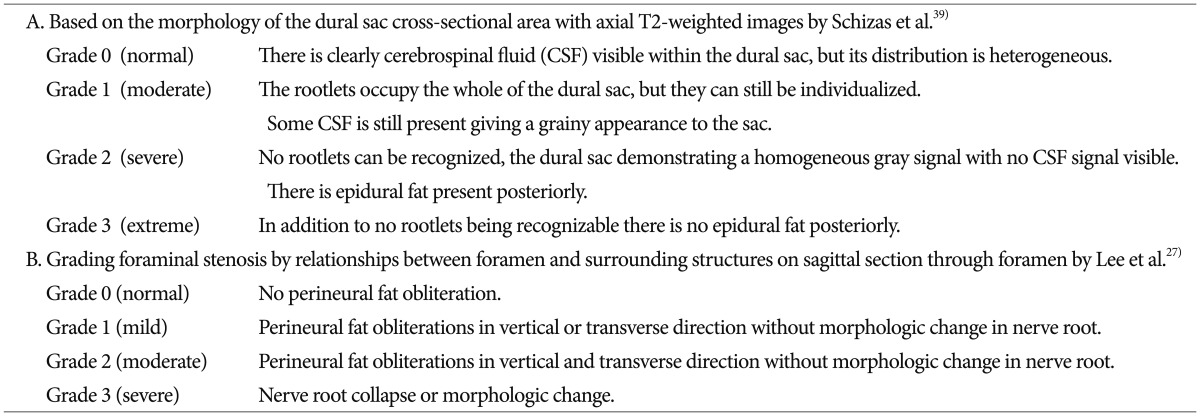
Sensory innervations of lower limbs were related to lumbosacral spinal nerves, especially common peroneal nerve and tibial nerve by L4, L5, S1. Therefore, two grading systems, based on the morphology of the dural sac in an axial MRI (Grade 0 : normal, 1 : moderate, 2 : severe, and 3 : extreme) and foraminal stenosis on a sagittal MRI (Grade 0 : normal, 1 : mild, 2 : moderate, and 3; severe), were used in the evaluation of neural compromises on L4-L5, L5-S1 (Table 1)27,39). Further, we investigated the demographic data, clinical characteristics, such as symptom duration, affected limbs, MRI grades, and aggravating factors and reviewed previous reports on etiology, prognosis and treatment of RLS.
All investigations were performed in accordance with our institutional guidelines that comply with all international laws and policies (Hallym University Institutional Review Board, #2013-10).
Go to :
RESULTS
Over a period of a year, the incidence of RLS was 5.00% (32/639). There were 16 males (50%) and 16 females (50%). The median age at diagnosis was 55.4 years (range, 25-93 years). The median duration of symptoms (from onset to diagnosis) was 14 months (range, 0.5-72 months).
The exact cause of RLS is unknown, but 12 patients have noted the beginning of their symptoms weeks or months after the procedures (epidural steroid injection : 2 patients, spinal anesthesia : 1 patient, lumbar microdiscectomy : 6 patients, percutaneous coronary artery stent insertion : 1 patient, subtotal gastrectomy : 2 patients). Twenty patients did not remember when they first noticed the discomfort, but 12 patients had underlying diseases (essential hypertension : 4 patients, diabetes mellitus : 4 patients, renal failure : 2 patients, hypothyroidism : 2 patients).
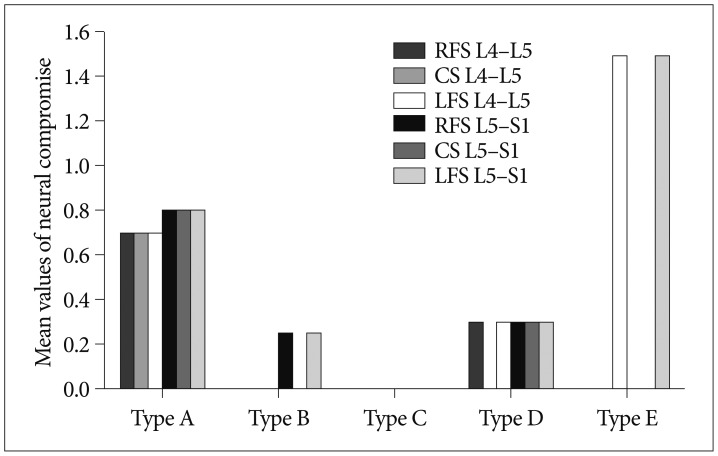
There were 26 patients with the affected limbs on the symmetrical and bilateral lower extremities (Type A : 20 patients, Type B : 3 patients, Type C : 3 patients). Four patients (Type D) were affected with symmetrical and bilateral on both lower and upper extremities and 2 patients on asymmetrical and bilateral lower extremities (Type E) (Fig. 1). Several degenerative changes in the lumbar spine MRI have been observed in 21 patients (spinal stenosis : 13 patients, bulging disc : 7 patients, degenerative spondylolisthesis 1 patient). In all patients except for type E, there are no correlation between the affected limbs of RLS and neural compromises on the lumbar spine (Fig. 2). However, in only 2 patients with bilateral but asymmetric leg discomforts, we found LDHs on left side of L4-5 and L5-S1, and also could not explain the opposite side symptoms on radiologic images. These patients were considered as mixed conditions; neural compromise due to LDH and RLS. Six patients were referred for uncontrolled bilateral legs' paresthesia from local clinics having microdiscectomy. Prior to surgery, they were presented with asymmetric and bilateral leg discomforts, and were diagnosed as herniated lumbar disc. Though surgery has been found helpful in diminishing ruptured side radiculopathy, they were still suffering from restless legs (Type A : 4 patients, Type B : 1 patient, Type C : 1 patient).
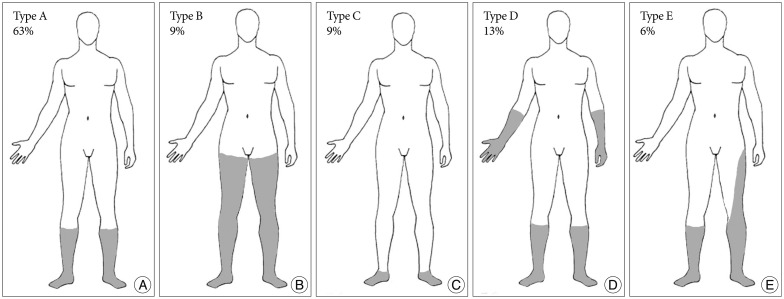 | Fig. 1We classified the affected limbs into five types. The symmetric distributions are as follows : Type A, below knees to feet (A); Type B, from proximal thigh to feet (B); Type C, both feet (C); Type D, both lower arms and lower legs (D); the asymmetric distribution is type E, including asymmetric severity with unusual localization (E).
|
Mirapex® (pramipexole : dopamine agonist; Boehringer Ingelheim, Ingelheim, Germany) was used alone or with Lyrica® (pregabalin, Pfizer, Freiburg, Germany) and these medications can be effective in decreasing unpleasant feeling in the limbs without sleep disturbance. All patients' conditions have become noticeably better on the following day after medication. During treatment, there were no dopamine related complications in subjects. A total of 71% of patients stopped medications within the first 6 months.
Case illustration
A 68-year-old woman was presented with severe paresthesia in the left leg and tingling sensation in the right lower leg (Type E). She had no underlying disease. Spine MRI shows left L4-5 foraminal LDH with Grade 3 foraminal stenosis (Fig. 3). She was treated with a L5 transforaminal epidural steroid injection and was followed up. She felt much improvement on left L5 paresthesia, but still had unpleasant sensation on both lower legs with aggravation during night time. We diagnosed as mixed conditions; left L4-5 LDH and RLS. She took additional pramipexole and then paresthesia of the lower legs disappeared.
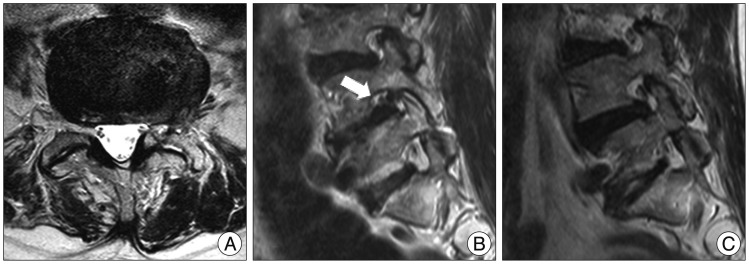 | Fig. 3Spine T2-weighted MR images (A : axial at L4-5) show a left foraminal disc herniation with stenosis. T2-weighted foraminal MR images (B : left side, C : right side) reveal that collapsed nerve root of the left L4-5 at the intervertebral foramen, grade 3 (arrow) and no obliteration of the right foraminal space, grade 0 in a 68-year-old female patient.
|
Go to :
DISCUSSION
RLS was first described by Thomas Willis in 1685 and has been introduced as a well-defined and common distressing entity since Ekbom's clinical description in 1945. Prevalence analyses reported over the past decade have demonstrated that up to 5% to 15% of adults in Western countries are likely to have RLS. Lower incidences of RLS are found in Asian populations when patients are clinically assessed with a specific questionnaire11,14,15,33,35,43). However, in a survey of Korean adults, the prevalence of RLS is comparable to that of Western countries13). Although, this study was not for the incidence of RLS in the general population, over one year, 32 of 639 patients (5.0%) who had undertaken lumbar MRI were diagnosed with RLS in accordance to the essential four criteria by IRLSG. The prevalence of RLS was generally higher for women, almost twice than men in a survey of the general population13,33,44). However, in a survey of population diagnosed with RLS, there was no gender difference in the prevalence of RLS20,36) and we obtained similar results. The occurrence of RLS increases to a peak at age 60 years and then decreases in Western countries and reaches a peak prevalence of 9.1% in the 6th decade of life of Korean adults13). In this study, 17 patients (53%) were in their fifties.
In a systematic survey of RLS in Koreans, 373 of the 5000 respondents (7.5%) met the criteria for RLS13). Despite a relatively high prevalence, this syndrome is usually under-diagnosed or misdiagnosed by clinicians12,16,37). Although there are limited data on under-diagnosis of RLS, Cho et al.13) reported that approximately 12.4% of RLS were not treated. In this study, 50% of patients have suffered from RLS over 12 months without proper diagnosis and treatment.
The diagnostic criteria reported by IRLSG6,7) lack the support of definitive electrophysiological data, and polysomnography change, like as periodic leg movements30,32). The pathogenesis of RLS still remains unclear, but several neuroimaging studies in patient with RLS have been performed using a functional MRI, single photon emission computed tomography and positron emission tomography. These radiologic studies suggest that RLS is related to dopamine D2-receptor dysfunction in the central nervous system, involving the brain and spinal cord. Zwartbol et al.51) presented a patients with an acute exacerbation of RLS because of cervical cord ischemia and this report supported the speculation that disturbance of spinal cord pathways are part of the etiology of RLS. As first described by Ekbom17), nearly all patients were presented with unpleasant sensation in their legs, we assumed sensory dermatomes of L4, L5, S1 were most affected areas in patients with RLS. In this study, we had only two patients caused by mixed conditions and thirty patients with RLS had no correlation with the degree of compromise of the spinal nerve. This result also supported RLS is considered to be a central nervous system related disorder.
Levodopa, as the precursor of dopamine, as well as dopamine agonists, plays an essential role in the treatment of RLS leading to the assumption of a key role of dopamine function in the pathophysiology of RLS. Iron, as a cofactor in dopamine production, plays a central role in the etiology of RLS3,5,18,26,38,42,45,48). Erikson et al.19) reported that there is a significant correlation between serum iron concentration and D2 receptor densities in the striatum, but not in other brain regions, leading to a selective D2 receptor loss (but not D1 receptor loss) with iron deficiency.
The most common clinical presentations of RLS are sleep disturbance, in addition to aggravated leg discomfort during night time leading to a significantly reduce quality of life. In a rat study, circadian patterns of neurotransmitter related gene expression has been shown in the brain regions involved in motor regulation. During daytime, mRNA levels for tyrosine hydroxylase were up-regulated in the substantia nigra and ventral tegmental area; whereas, in the caudate nucleus and putamen, expression level of dopamine D2 receptors were lower during daytime. However, the expression of dopamine D1 receptors remained stable over day and night7,46).
Though degeneration of the spine is a common problem that generally advances with age, about 20% of asymptomatic patients before 60 years of age were found to have at least one herniated disc10). Further studies have found that the degree of disc herniation or nerve root compression on MRI scans did not always correlate with patients' subjective legs symptoms9,25). We confirmed degenerative changes of the lumbar spine on 21 of 32 RLS patients by MRI. However, these MRI results including grades of neural encroachment could not completely explain their problems. In only 2 patients with mixed conditions, we understood the reason why the unilateral legs are experienced more extended and severe pain than the opposite side.
Michaud et al.29) studied the incidence of arm restlessness assessed by a questionnaire in 230 patients diagnosed with RLS and it was reported by 48.7% of the subjects. Winkelmann analyzed clinical characteristics of the RLS in 300 patients and independently the following result was seen; arm discomforts in 26.1%, thigh symptoms in 46.8%, feet symptoms in 56.5%, and calves discomfort in 87%. In this study, 3 patients presented with paresthesia from the proximal thigh to the feet and both limbs were involved in 4 patients.
Causes related with a higher incidence of RLS include pregnancy, iron deficiency, renal failure, diabetes mellitus, uremia, neuro-degenerative disease and medications. Acute or transient RLS can be observed in spinal lesions and following spine surgery or spinal anesthesia8,22). In this study, 9 patients have announced leg discomforts with sleep disturbance, following spine procedures, and 12 patients had underlying diseases.
Hoque and Chesson23) reviewed thirty-two literatures on pharmacologically induced RLS with five groups; antidepressant, histamine antagonist, anti-psychotic, antiepileptic, and other; and reported that the strongest evidence available for drug induced RLS are for the following drugs; escitalopram; fluoxetine; Levodopa and pergolide; L-thyroxine; mianserin; mirtazapine; olanzapine; tramadol, and amitriptyline. Without strong evidence, antiepileptic drugs (phenytoin, methosuximide, zonisamide), cimetidine and caffeine are also considerable factors that induce RLS. Among these medications, we thought that tramadol, amitriptyline, fluoxetine, cimetidine, and phenytoin were commonly prescribed by neurosurgeon.
Because RLS and its symptoms can be caused by various conditions, obtaining an accurate diagnosis is crucial for management and treatment. In pure peripheral neuropathy such as LDH, spinal stenosis, and DM neuropathy, patients do not have the compelling need to move to relieve leg discomfort and the symptoms are not consistently worse at rest or at night.
Though most surgeons are not familiar with RLS, it can be treated quite easily with avoidance of aggravating factors and some medications. A generally accepted hypothesis on the pathogenesis of this disorder is a circadian alteration of the dopamine metabolism in the nervous system, leading to diminishing intra-cortical inhibition and supra-spinal inhibition1,18,19,37,47,50).
As a logical consequence, dopaminergic agents are considered to be the first-line therapy in the management of RLS and several studies are being conducted to establish the efficacy of these substances. Levodopa can lead to a directly increase in the dopamine level in the brain1,34,47,50). However, because of its short half-life, which can be partially prolonged by the extended release formulation, and the augmentation effect, levodopa is not frequently used in RLS4). The frequent side effects also restrict the use of the ergotamine dopamine agonists such as bromocriptine, pergolide, and cabergoline. For this reason, in the last two decades, the non-ergotamine dopamine agonists, such as pramipexole and ropinirole, have become the most used treatments in RLS due to their effectiveness, half-life and safety with very low dosages28,40). Ropinirole, and Pramipexole were approved by the US Food and Drug Administration for the treatment of RLS and the clinical efficacy of these two medications can be considered similar28). Clearly, levodopa or dopamine agonists are valuable for treating and subsiding RLS but these dopaminergic agents may give rise to "augmentation effect" in some patients. Clinical features of the augmentation effect show that RLS symptoms become more severe, and occur earlier in the daytime as well as extend to other parts of the body, several months after start of treatment. The mechanism of this complication was not clear, but proposed in a hyperdopaminergic state, the dopamine D1 receptor response may be predominated with increased dopamine tone4,49). In a preliminary study, Montplaisir described the results of 2 open label studies of ropinirole and noted that augmentation developed in 4% of RLS patients31). Winkelman and Johnston49) assessed the augmentation rates of patients treated by pramipexole and augmentation developed in 32%. Hence, there is a need for alternative medications without the interaction with dopamine metabolism. Several studies have supported that gabapentin enacarbil and pregabalin were effective for treating RLS and also improved sleep hygiene2,24,41). We initially prescribed pramipexole alone for RLS patients or if a patient complained of severe paresthesia on their legs, additional pregabalin was prescribed. All patients showed improvement in their RLS symptoms, sleep disturbance and daytime activity. Only 9 patients were still taking these medications past 6 months, and 71% of patients were considered to be completely cured.
Go to :
CONCLUSION
The RLS is a clearly common central nervous system related disorder of the limbs, usually the legs. Some patients may visit neurologist or neurosurgeon to evaluate their spine problems. However, the RLS does not occurr by the mechanical abnormality of the lumbar spinal nerve. We suggest that the awareness of this syndrome can help reduce diagnostic error; thereby, avoiding the morbidity and expense associated with unnecessary evaluations or inappropriate treatments in RLS patients.
Go to :
 XML Download
XML Download