

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spinal epidural lipomatosis (SEL) is a disorder defined as having pathological overgrowth of normal extradural fat, which can compress the spinal canal or nerve root. It has been regarded as a consequence of long-term administration of exogenous steroids, associated with a variety of glucocorticoid-producing systemic diseases9).
Several literatures, in western population, including retrospective reports on SEL have been analyzed with respect to disease etiology, gender, age, BMI, involved segments, treatment methods and their outcome. Until now, however, no reviewed article ever dealt with Koreans except for sporadic case reports.
The SEL characteristics of Koreans and Westerners were reviewed and compared to the following scrutiny of those reported cases studies, including three cases for this report.
CASE REPORT
Case 1
A 43-year-old male without any underlying illness, suffered a neurologic deficit and neurogenic intermittent claudication (NIC) of his lower legs, which were precipitated by ambulating a distance longer than 100 meters. His symptoms were aggravated despite the conservative treatment. This patient had no history of administering any exogenous corticosteroid. He was fatty and of a short stature without cushingoid appearance. His body weight was 57 kg and his height was 148 cm.
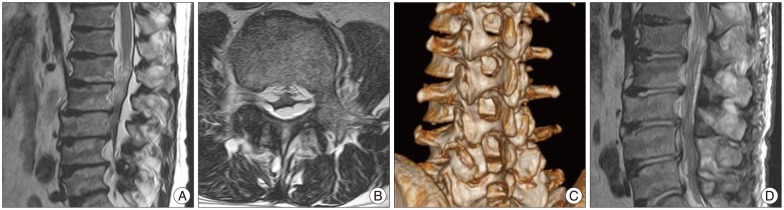
Lumbar MRI on T2-weighted image (T2WI) implicated that the fatty lesion extended from the posterior aspect of L1 body to the body of S1 (Fig. 1A). The axial image revealed the typical "Y-sign" or "Stellate-sign" of the thecal sac (Fig. 1B). Multi-level small laminotomy was performed on the left side of L1, L2, L3, L4, and L5, while bilateral decompression was carried out with a one-side approach (Fig. 1C). The patient showed an immediate improvement after surgery. Postoperative MRI revealed a much reduced epidural fat and decreased compression of the sacral sac (Fig. 1D). Six months after follow-up, he was free from the symptoms.
Case 2
A 58-year-old male had a sustained lower back pain, leg fatigue and weakness, showing neurogenic intermittent claudication (NIC). He had diabetes mellitus and hypertension. The NIC symptoms were precipitated by walking longer than 50 meters. He had no history of administering any exogenous corticosteroid. He had no definitive cushingoid appearance. His body weight was 76 kg while his height was 164 cm.
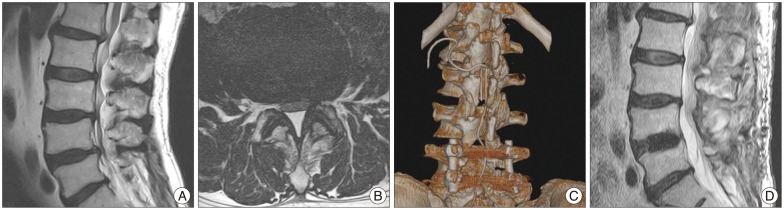
The sagittal and axial T2WI MR images showed an extensive epidural fat deposition with a thecal compression from L1 to L5-like thread beads on the string (Fig. 2A, B). Concomitant L4-5 spinal stenosis, due to a protruded disc and ligamentum flavum hypertrophy, was also seen. Right L3 hemipartial laminectomy and L4 total laminectomy with the interbody fusion on L4-5 were performed for the treatment of underlying spinal stenosis (Fig. 2C). The fat above and below the laminectomy level was scraped out with a hook. Postoperative MRI revealed much reduced epidural fat with decompression of the thecal sac (Fig. 2D). After the operation, the patient improved immediately and one year after follow-up.
Case 3
A 69-year-old male with diabetes mellitus, hypertension, and chronic renal disease, had a longstanding radiating pain, and showed symptoms of NIC predominantly in the anterior aspect of the right knee. These symptoms were precipitated upon a mere initiation of ambulation. He had no definite cushingoid appearance. His body weight was 62 kg while his height was 155 cm. This patient had numbness in the sensory dermatomal distribution of L4 in the right leg.
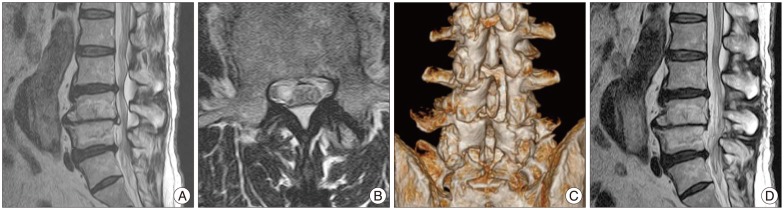
The Lumbar MRI revealed moderately bulged intervertebral discs at L4-5 and abnormal hypertrophy of the adipose tissue on the posterior aspect of the spinal canal extending from L3 to L5. It was especially shown in the anterior aspect of the body of right L4, which revealed compression on the dural sac and right L4 nerve root (Fig. 3A, B). Right L4 hemi-laminectomy, L4-5 discectomy and debulking of the epidural fat, especially on the right anterior aspect of the L4 body (Fig. 3C), were performed. The postoperative MRI revealed a greatly reduced epidural fat, distinctive visualization of the decompressed sacral sac, and L4 root (Fig. 3D). He also showed satisfactory improvement during the follow-up observations.
DISCUSSION
Lee et al.20) in 1975 first described SEL that developed in a patient who had a renal transplantation. SEL is a rare disease, which may occur after long-term steroid administration for the treatment of organ transplantation, dermatomyositis, systemic lupus erythematosus, nephrotic syndrome, asthma, sarcoidosis, rheumatoid arthritis or Crohn's disease, or by systemic disease or endocrinopathies producing excessive endogenous corticosteroid1,16,20).
Occasionally, SEL occurs without any evidence of specific cause. Badami et al.2) in 1982 first reported idiopathic SEL, associated with a symptomatic deposition of spinal epidural fat without any history of exogenous steroid administration or endogenous corticosteroid producing endocrinopathies as described above. Haddad, et al.10) first hypothesized that idiopathic SEL was caused by obesity only without steroid association. A significant number of patients with idiopathic SEL in the literature were males, and more than 75% of all reported patients were obese26).
The treatment of SEL varies from conservative management to surgical treatment. Surgery may be necessary for patients who failed in weight reduction merely to improve the symptoms or for patients with intractable clinical manifestations. So far, according to the paper, the steroid associated cases commonly occurred in thoracic segments, whereas idiopathic cases were usually found in the lumbar segments1,9,13).
Kawai et al.13) review of 30 idiopathic SEL cases showed that this disorder had a strong tendency of male-predominance, and that only 3 of these cases were females. Obesity was observed in most patients and only 4 patients were of normal body weight. The mean age was 42.3 years and the average body mass index was 29.0. The most commonly involved area was the lumbosacral spine (57%)13).
Al-Khawaja et al.1) in 2008 published another review article of SEL with 111 patients where 69 were relevant to steroids, while the remaining 42 were not. Male gender was predominant in both idiopathic SEL and secondary SEL groups, taking up 80% and 70%, respectively. 65% of idiopathic SEL occurred in the lumbar segments, whereas 73% of secondary SEL occurred in the thoracic segments.
Frogel et al.9) in 2005 published a review article with 104 SEL patients. They classified SEL into four categories : the exogenous steroid use, 55.3%; obesity only, 24.5%; the endocriopathy or endogenous steroid group, 3.2%; and the non-obese idiopathic group with approximately, 17%. According to their review, thoracic involvement was associated with the steroid-administered group, while the idiopathic SEL group was found to involve the lumbar segment predominantly9).
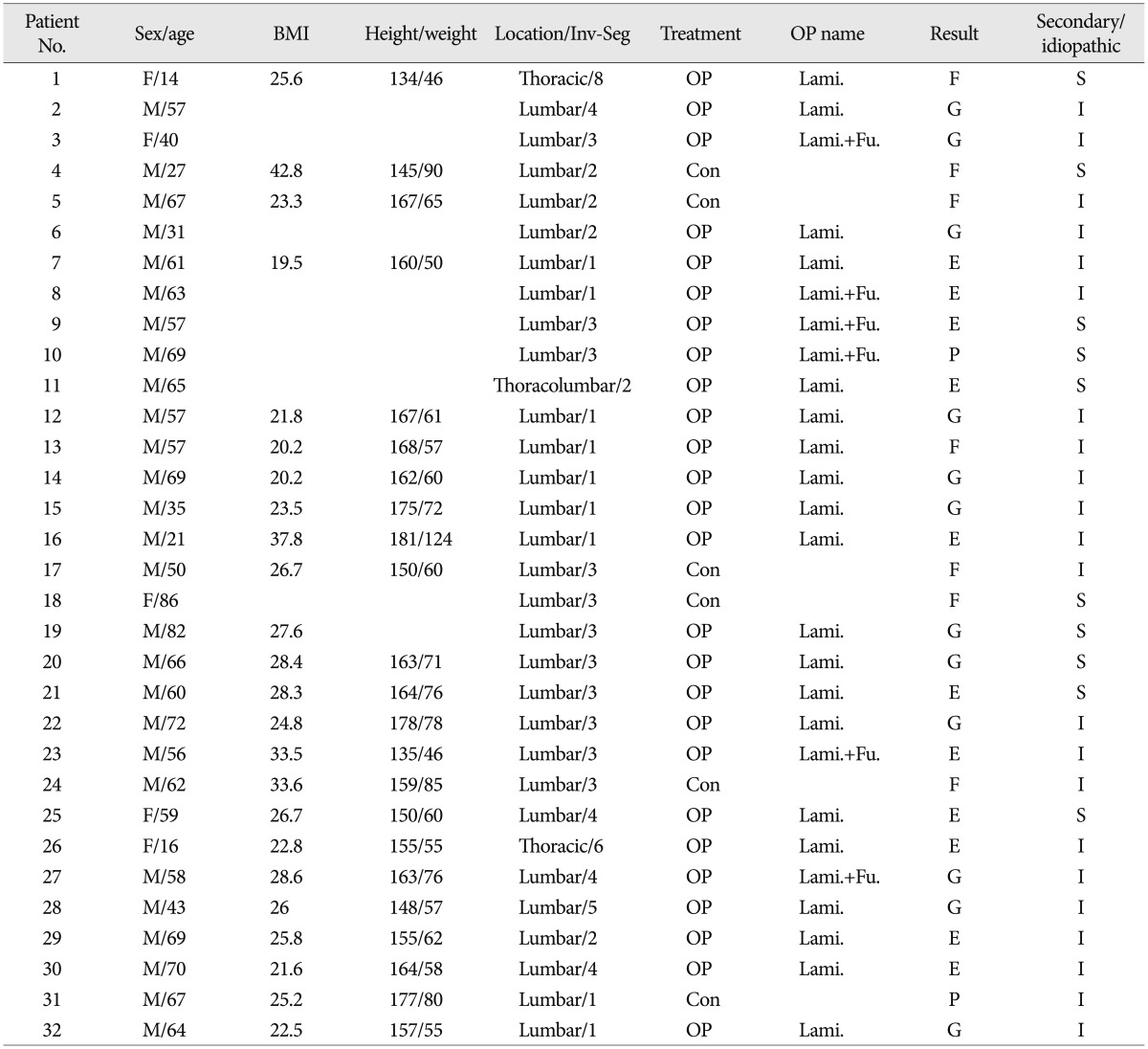
Medical Journal Search engines such as KoreaMed, KM base, and PubMed were utilized to find published articles of SEL associated with the Korean ethnicity. Kim et al.16) in 1986 first reported a case of SEL that a Korean patient with adrenocortical adenoma had developed. Up to now, 32 cases in 19 papers were found. These included 3 cases of this report. The SEL characteristics of Korean patients are shown in Table 1. Three (3) cases of this report and 29 already-published cases of Korean SEL patients were carefully examined and analyzed23). Idiopathic SEL is defined as a rare disorder that causes spinal cord compression and neurological deficits without any evidence of exogenous steroid administration, endogenous Cushing's syndrome or endocrinopathies.
Of those 32 cases, 22 were idiopathic and 10 were secondary SEL cases. The mean age was 55.3 years while the male-to-female ratio was 84.3 to 15.7. However, no significant difference between domestic and foreign cases was found. The mean BMI of domestic cases was 26.5, which was less than that of foreign cases. The idiopathic SEL group among Koreans took up 68.8%, which was significantly different from that of the f reign cases. The secondary SEL group of foreign cases took up 62% to 75%1,8,9,13).
In the analysis of inflicted area, only three of domestic cases involved the thoracic segment. Among those foreign cases, idiopathic SEL cases usually involved the lumbar segments while the secondary SEL group involved the thoracic spine. In our review, thoracic involvement was seen in only 3 cases. Two cases were secondary SEL and one case was idiopathic SEL. Surgical intervention was carried out in 23 cases (78.1%) and the result of surgery was excellent to good in every case except for one case of mortality which was related to medical complications3,4,5,6,7,11,12,14,15,16,17,18,19,21,22,24,25,27,28). Surgical results were similar between domestic and foreign cases. The causative factor of the racial difference was unidentified.
In summary, cases of Korean showed higher incidences of idiopathic SEL, for which the infliction (fat lesion) was manifested predominantly in the lumbar segments, and rarely developed in the thoracic segments, while Korean patients had a lower BMI, in comparison with that of western cases. The inquiry of these case studies is the first comparative analysis between Korean and western SEL cases. Nevertheless, the reason behind such racial differences has not been elucidated.
CONCLUSION
According to this study, there were differences between Korean and western cases. Koreans had higher incidences of idiopathic SEL, predominant involvement in the lumbar segments, very few thoracic involvement and lower BMI, as opposed to westerners. Owing to the lack of a large series of Korean SEL cases, direct comparisons with western reports may not be conclusive and further studies are needed in the days ahead including systemic analysis and multi-center study.
 XML Download
XML Download