

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
IgG4-related disease is a recently defined disorder characterized by an inflammatory reaction rich in IgG4-positive plasma cells associated with sclerosis4). This disease includes autoimmune pancreatitis, Mikulicz disease, pseudotumor of the lung, tubulointestinal nephritis, and Riedel thyroiditis4). Central nervous system involvement is extremely rare, and the most commonly reported location is the pituitary gland4).
Hypertrophic pachymeningitis is an uncommon disorder that causes a localized or diffuse thickening of the dura mater10). Rare cases of dural spinal involvement by IgG4-related screlosing disease have also been reported1,2), and recently, the possibility that IgG4-related sclerosing disease may underlie some cases of intracranial hypertrophic pachymeningitis has also been suggested. However, only 9 cases of intracranial hypertrophic pachymeningitis related to IgG4 infiltration have been reported in the literature3,5,6,7,8,9,11). We herein report an additional case of IgG4-related intracranial hypertrophic pachymeningitis proved by both local infiltration of plasma cells and IgG4/IgG ratio in surgical specimen.
CASE REPORT
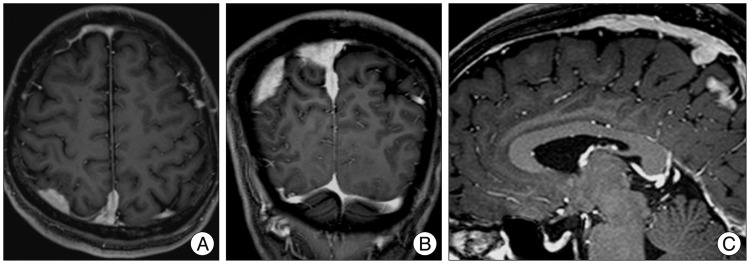
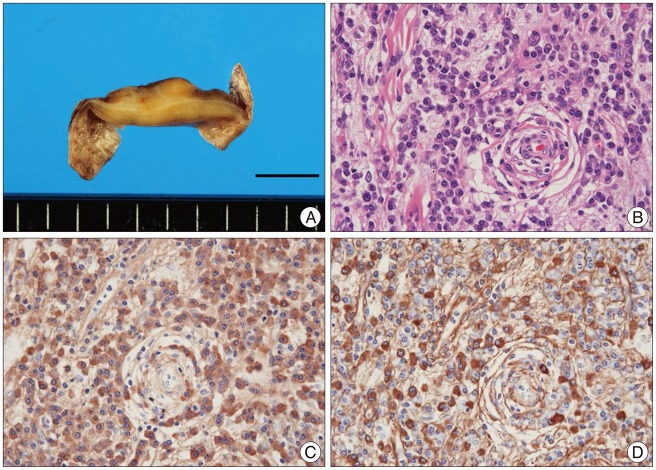
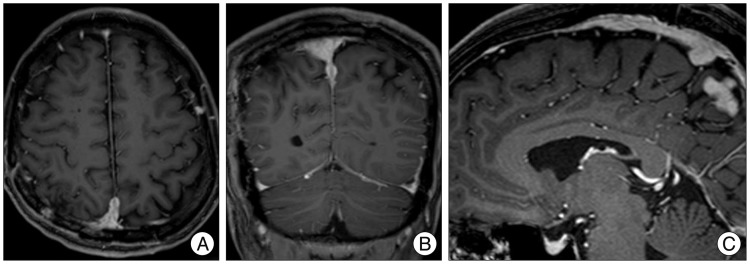
A 45-year-old, previously healthy male presented with focal seizure of left extremities with generalization. On admission, his neurological examination was normal. MRI revealed irregular dural thickening and a marked enhancement of the right parieto-occipital dura and falx (Fig. 1). Whole-body 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography scanning demonstrated no abnormal hyperuptake, in the whole body, including the brain and dura. The preoperative differential diagnoses included meningioma en plaque, lymphoma, tuberculosis, sarcoidosis, collagen vascular disorders, lymphoma, meningeal carcinomatosis diseases and IgG4-related disease. Surgical resection was performed via craniotomy. The mass in the convexity dural region was resected, while the mass adjacent to the superior sagittal sinus and falx was not removed. In the surgically resected specimens, a solid yellow to white-colored lesion measuring 35×33×6 mm was found in the dura mater (Fig. 2A). Histologically, the solid lesion consisted of a proliferation of fibroblast-like spindle cells and an infiltration of mononuclear cells, including predominantly plasma cells, with abundant collagenous tissue (Fig. 2B). For immunohistochemistry, we used monoclonal antibodies against IgG and IgG4. In the immunohistochemical study, most of the plasma cells infiltrating into the sclerosing lesion were found to be IgG-positive [IgG4-positive plasma cells/high power field (HPF), 78], and the ratio of IgG4-positive plasma cells to the overall IgG-positive cells was 45% in the area containing the highest infiltration of plasma cells (Fig. 2C, D). On the basis of the above findings, IgG4-related sclerosing disease arising from the dura mater was suspected. Thus, we evaluated a patients' serum IgG4 level and it was 51 mg/dL (normal range, 4.8-105.0 mg/dL). The patient's postoperative course was uneventful, and no radiological or clinical signs of recurrence were noted 12 months after performing a surgical resection (Fig. 3). Adjuvant steroid therapy was therefore put on hold.
DISCUSSION
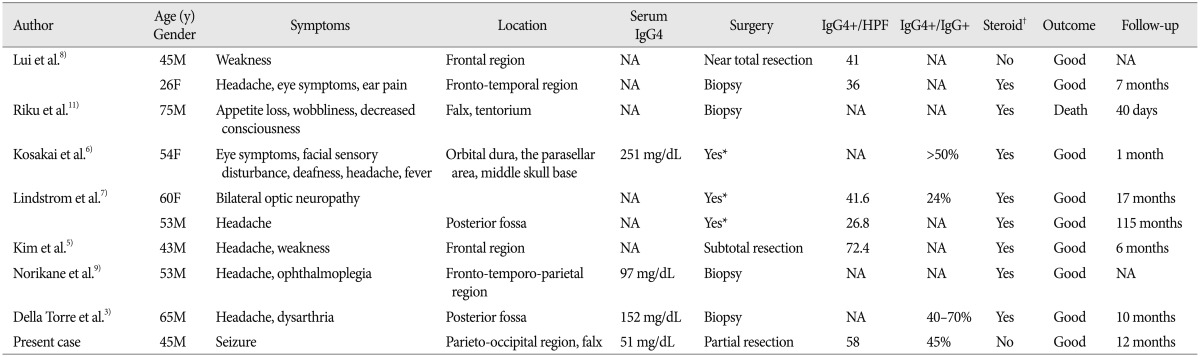
IgG4-related intracranial hypertrophic pachymeningitis is extremely rare. To the best of our knowledge, only 10 cases have been reported in the literature, including the present case3,5,6,7,8,9,11). A summary of the cases is shown in Table 1. The ages of the patients ranged from 26 to 75 years (mean, 51.9 years). Seven patients were male and three were female. Headache was the most common symptom (60%). The serum IgG4 levels were evaluated in four patients, and elevated IgG4 level was observed in one patient. All patients underwent surgery. Steroid treatment was started prior to surgery in one case, and after surgery in seven cases. The outcomes were good, except for one patient who was diagnosed at autopsy.
There are no definite diagnostic criteria for IgG4-related disease. However, some researchers have recommended a cut-off level for the absolute number of IgG4-positive cells at >50/HPF, and the ratio of IgG4-positive cells/IgG-positive cells >40%4). The elevation of the serum IgG4 levels is not mandatory for the diagnosis, because the serum IgG4 level often correlates with the disease activity and the number of involved organs, but the levels may also be normal4). Our patient met the above diagnostic criteria. Additionally, our literature review suggested that serum IgG4 level may be normal in most patients with IgG4-related intracranial hypertrophic pachymeningitis.
Steroid treatment has been recommended for intracranial hypertrophic pachymeningitis as well as IgG4-related disease. However, conservative observation can also be applied in some patients. As a result, we therefore put adjuvant steroid therapy on hold for our patient. Some authors have suggested that a biopsy, followed by steroid treatment, may be safe and valid7,8). However, due to their rarity, there is no unified treatment protocol for such cases. To date, it remains unclear whether biopsy or partial/subtotal resection is better, and whether steroid treatment is necessary. In our patient, easily resectable lesion was removed, whereas we consider that biopsy might be sufficient to obtain definitive diagnosis. Further investigations are required to determine the optimal treatment strategy.
 XML Download
XML Download