

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Various intra-abdominal complications caused by ventriculoperitoneal (VP) shunt have been reported. Among them, pyogenic liver abscess is very rare, especially the occurrence of multiple abscesses. To the best of our knowledge, only nine such cases have been reported in the English literature since the first report by Fisher et al. in 19834). We present another unusual case of multiple liver abscesses, review the previously reported cases, and postulate the most likely pathogenetic mechanism of multiple liver abscess formation after VP shunt.
CASE REPORT
A 50-year-old woman who had been in a vegetative state for two months due to a spontaneous intracerebral and intraventricular hemorrhage was transferred to our hospital. A brain computed tomography (CT) scan revealed severe hydrocephalus without intracerebral hemorrhage and intraventricular hemorrhage. Five days after admission, a VP shunt was implanted. Fifteen days later, the patient had a temperature over 38℃ and a chest X-ray showed patchy consolidation with partial collapse in the right lung. A sputum culture isolated Pseudomonas aeruginosa and Staphylococcus aureus. Cerebrospinal fluid (CSF) and blood cultures were negative.
The patient received an initial regimen of intravenous antibiotics (piperacillin/tazobactam and fluconazole), which was shifted to ciprofloxane due to a sustained high fever until the fever subsided. However, the patient became febrile again 6 days later. Liver function tests yielded an alanine aminotransferase level of 115 U/L and an alkaline phosphatase level of 702 IU/L. Fortunately, a chest X-ray showed gradual improvement of the right lung compared to the previous study. At that time, an ultrasonography of the liver revealed two 6-cm-sized hypoechoic masses. A subsequent abdominal CT showed multiple irregular-walled and diverse-sized cysts, including two large ones, which were not enhanced (Fig. 1). The long segment of the distal shunt tube was found going through the subcapsular portion of the right hepatic lobe and the tip of the tube was embedded in the lower large cyst (Fig. 1B, C). Ultrasonography-guided needle aspiration of the upper lesion and percutaneous catheter drainage of the lower lesion resulted in continuous gushing of yellowish pus. Culture of the abscess isolated Staphylococcus capitis (S. capitis), which was sensitive to vancomycin. The patient became afebrile with the administration of intravenous vancomycin at a dose of 500 mg every 12 hours for several days. The patient was unremarkable neurologically and neuroradiologically. A subsequent abdominal CT showed a marked shrinkage of the liver abscesses. A VP shunt revision was then performed with the distal shunt tube extracted uneventfully from the liver, which was enveloped in yellowish pus. The result of CSF culture was negative. Follow-up examinations have been unremarkable, with normal shunt function without the recurrence of liver abscesses.
DISCUSSION
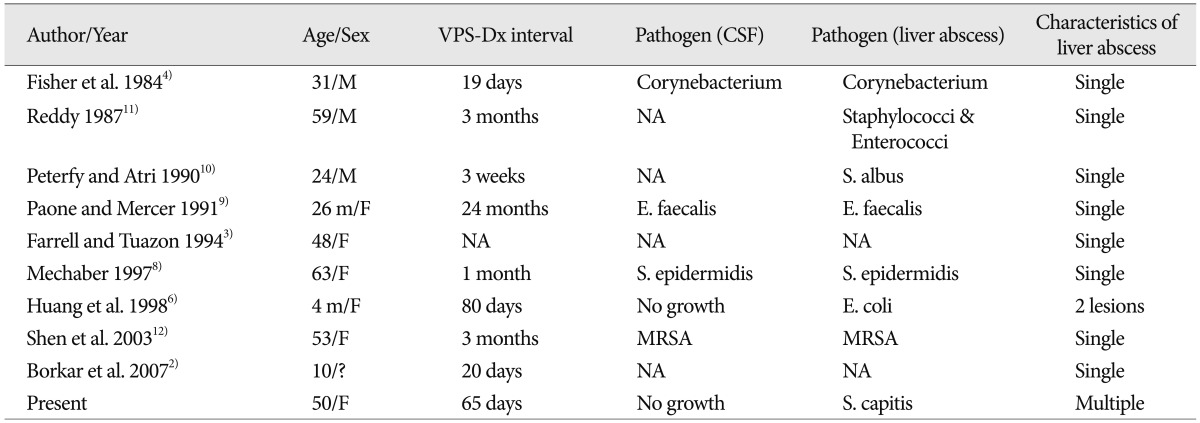
A distal shunt catheter retained within the peritoneal cavity as a foreign body can migrate to any viscera, subsequently creating various complications. Liver abscess is a very rare intra-abdominal complication of the VP shunt. We found nine cases of liver abscess associated with a VP shunt in English Medline literature; they are summarized in Table 1. In our case, a long segment of the distal peritoneal shunt tube was found passing through the subcapsular portion of the liver, and an abdominal CT showed the end tip embedded in the lower cystic cavity. Multiple abscesses were also seen around the intra-hepatic shunt tube (Fig. 1).
Although we cannot explain why or how the catheter migrated to the liver and became fixed there, we postulate the most likely pathogenetic mechanism for the development of liver abscesses. The sharp and hard tip of the tube initially anchored around the liver and may have exerted repeated pressure on liver capsule (Glisson's capsule)9). Combined with the water hammer effect of CSF pulsation, liver perforation eventually occurred5). In addition, mechanical irritation with the local inflammatory process between the liver capsule and catheter tip might also have facilitated the penetration of the shunt tube into the liver parenchyma7). The tip then advanced, thereby drawing in the entire distal shunt catheter into the liver. In the review, it did not take long time to develop a liver abscess associated with VP shunt (Table 1). The time interval from the last VP shunt operation to the development of a liver abscess ranged from 19 days to 3 months. Exceptionally, one case was so long as much approximately two years but VP shunt infection was diagnosed approximately two weeks before the diagnosis of liver abscess9). Our case took 65 days. The clinical condition usually started with fever and nonspecific abdominal symptoms and continued with the development of neurologic symptoms. In our case, the diagnosis was somewhat delayed because our patient could not complain anything because of vegetative state and had only intermittent high fever.
Certain pathogens isolated from liver abscesses in previous cases were Corynebacterium, Staphylococcus albus, Staphylococcus epidermidis, Enterococcus faecalis, Escherichia coli, and methicillin-resistant Staphylococcus aureus. One author described his pathogen just as rare Staphylococcus and Enterococci. The other two authors did not comment on their pathogens. This is the first reported case of liver abscesses caused by S. capitis. S. capitis is usually a nonpathogenic coagulase-negative species that is rarely associated with liver abscess. Most pyogenic liver abscesses are polymicrobial, and mixed enteric facultative and anaerobic species are the most common pathogens6). Therefore, we presumed the liver abscesses in our case formed as a result of translocation of skin flora from the infected VP shunt rather than seeding into the liver via the portal veins due to intra-abdominal sepsis. The compromised state of our patient would potentiate this rare occurrence.
Of the 10 cases of liver abscesses including ours, eight cases were a single abscess and two were multiple ones (Table 1). Multiple liver abscesses are associated with higher mortality than a single liver abscess, especially in compromised patients1). Adequate treatment methods in such cases are beyond the scope of this report. Although we delayed in establishing the exact diagnosis by neglecting the potential hepatic complications of a VP shunt, our patient responded favorably to the intravenous antibiotic therapy, needle aspiration, and a catheter drainage procedure. Finally a shunt revision was performed. All of the other reported cases also had favorable outcomes.
CONCLUSION
Liver abscess formation is a potential complication of VP shunt surgery. The postulated pathogenetic mechanism of liver abscess formation is migration, penetration of the infected shunt tube into the liver, and subsequent abscess formation. The compromised state of the patient will potentiate this rare occurrence. Awareness and vigilance of the possibility of a liver abscess complicating VP shunting will help establishing an early accurate diagnosis and appropriate therapy.

 XML Download
XML Download