

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Transforaminal lumbar interbody fusion (TLIF) has become a common surgical method of spinal fusion. Compared with posterior lumbar interbody fusion (PLIF), TLIF is safer in insertion of a fusion cage into the intervertebral disc space. It has been used as an effective treatment for patients who have unstable low-grade isthmic spondylolisthesis that is unresponsive to nonsurgical treatment4). Also, several types of fusion cages have been developed for TLIF and some are almost the same as PLIF cages. Regardless of cage shape and number, complications associated with fusion cages have been reported in patients under TLIF7,19,22). However, anterior cage migration during the follow-up period after PLIF or TLIF has not been reported to date. We present a case of delayed anterior dislodgement of a banana-shaped polyetheretherketone (PEEK) cage following TLIF for the treatment of grade I isthmic spondylolisthesis with a lumbosacral transitional vertebra (LSTV) and dystrophic change of the L5 vertebra.
Go to : 
CASE REPORT
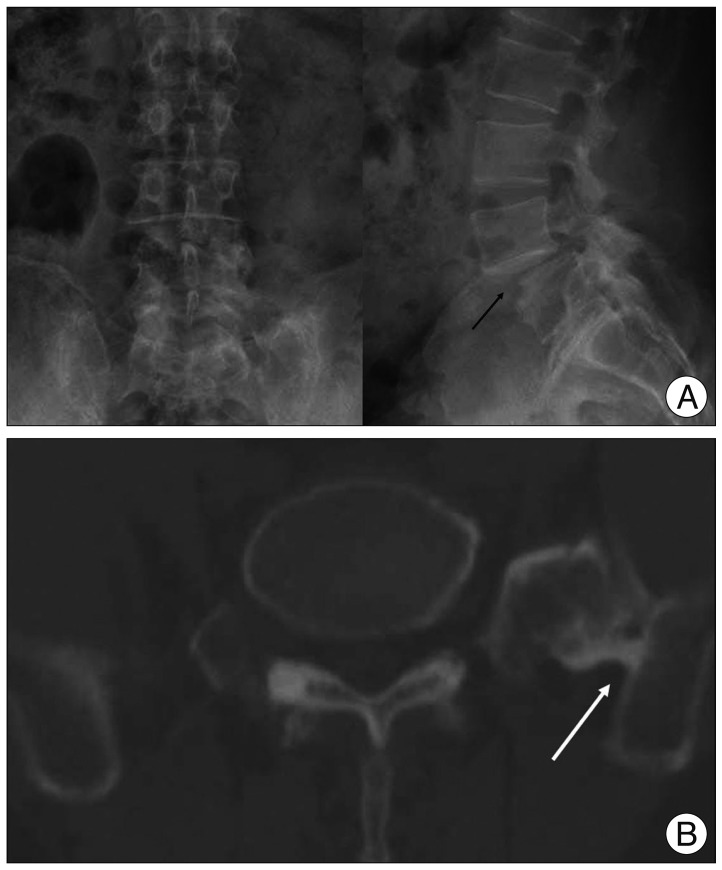
A 51-year-old man presented with lower back and radiating pain to both legs. His symptoms had developed 5 years ago, but conservative treatments had failed. On admission, he had a limping gait and his pain was aggravated by posture. Neurological examinations showed grade 4/5 strength in extension of his left big toe. Plain radiographs and CT images showed L4-5 grade I isthmic spondylolisthesis with instability, a LSTV (Castellvi IIIa), and a dysplastic L5 vertebral body (Fig. 1)3). The anteroposterior length of the cranial endplate of the L5 body was relatively shorter than that of the L4 body, even though the surface was flat. Magnetic resonance images showed canal and foraminal stenosis and L4-5 disc degeneration. The bone mineral density measured by Dual-emission X-ray absorptiometry showed a T score of -2.1 for the lumbar spines.
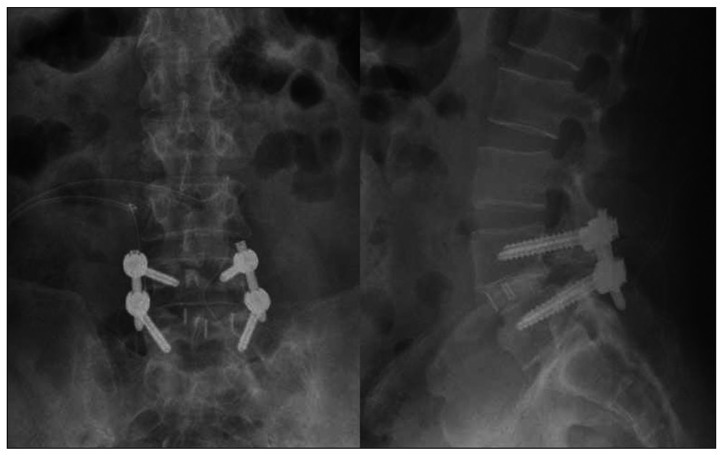
L4-5 decompression via bilateral paraspinal approaches was performed and a banana-shaped PEEK cage (WSH T-cage, WINNOVA CO., Ltd., Seoul, Korea) was inserted through an opening in the intervertebral disc on the left side, followed by bilateral pedicle screw fixation with reduction (VIPER™, DePuy Spine, Inc., Raynham, MA, USA). Local autograft and allograft cancellous bone chips were packed into the fusion cage and into the remaining intervertebral disc space posteriorly after the cage insertion. After surgery, the presenting symptoms significantly improved and the radiographs showed a good reduction (Fig. 2). The patient's pain was assessed on visual analogue scale and improved dramatically after surgery (before surgery; 8 for low back pain, 10 for leg pain : 1 week after surgery; 2 for low back pain, 2 for leg pain). The patient was discharged at postoperative 7 days and returned to daily living activities while wearing a corset.
Seven weeks after surgery, he visited to our outpatient clinic with severe low back and left leg pain for 7 days without any neurological deficit. He denied any history of trauma. Plain radiographs showed anterior dislodgement of the fusion cage as well as a reduction loss of the spondylolisthesis at the L4-5 level (Fig. 3A). Sagittal images on a CT scan demonstrated that the intervertebral space was not fused and the screws were loosened with halo change (Fig. 3B). Physical signs and laboratory findings on admission did not support infection. Revision surgery using an anterior approach was performed to remove the displaced cage. A 5-cm-long midline incision was made and a retroperitoneal approach to the affected level was done using a robotic arm retractor. The anterior longitudinal ligament and annulus were not perforated. The cage had slipped down and was positioned anterior to the L5. After removal of the cage and previously grafted bones in the disc space, the endplates were carefully prepared. A wedge-shaped, lordotic titanium cage (WSH cage, WINNOVA CO., Ltd., Seoul, Korea) filled with allograft chips was inserted a little laterally to the left to avoid a collapsed portion of the inferior endplate of the L4 body. After the closure of the anterior surgical wound, the patient was positioned prone for pedicle screw replacement. The pedicle screws found unstable and in spite of being with thicker and longer ones, two L4 screws still remained loose. Therefore, cement augmentation was added to the L4 screws (Fig. 4A). Postoperatively, however, the patient complained of persistent pain on the anterolateral side of the left leg and difficulty in walking. CT images showed a fracture on the pedicle and anterolateral lateral body wall of the L5 vertebra (Fig. 4B). As a result, he had additional surgery for paraspinal decompression on the left side at the L4-5 level. Removal of the left L5 screw followed by bilateral extensions of the pedicle screw fixation to S1 was performed (Fig. 5). Because the L5-S1 level was congenitally fused due to the LSTV, we considered that extension of the screw fixation made no additional motion limitation of the lumbosacral spine but increased stability.
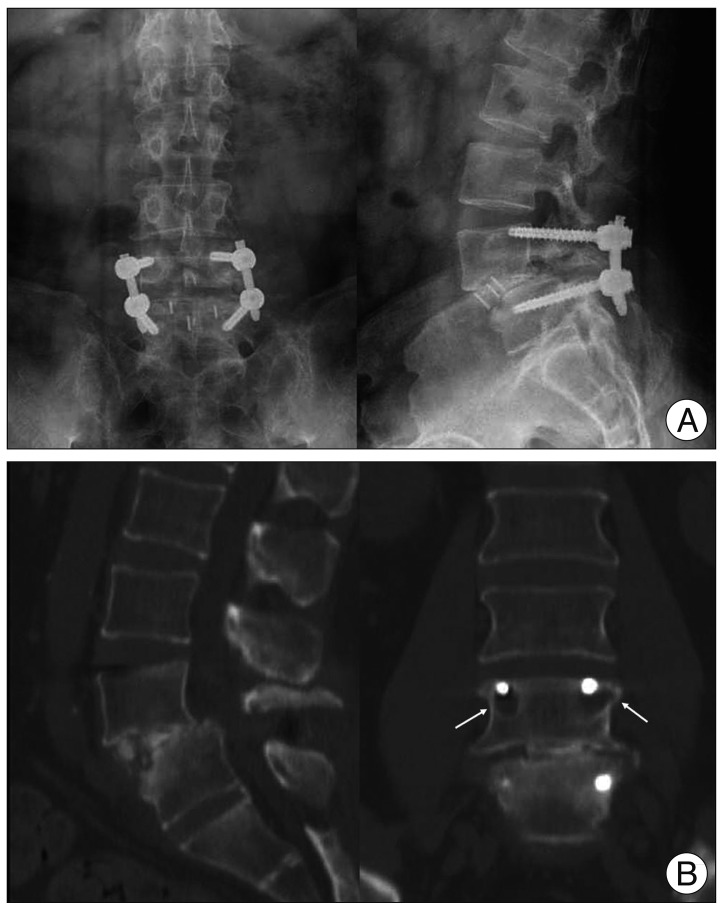 | Fig. 3Plain radiographs (A) and CT sagittal and coronal reconstruction images (B) at postoperative 7 weeks. A : Anterior dislodgement of the fusion cage as well as reduction loss of the spondylolisthesis at the L4-5 level. B : CT images showing that the intervertebral space was not fused and the L4 pedicle screws were loose with osteolysis (white arrows).
|
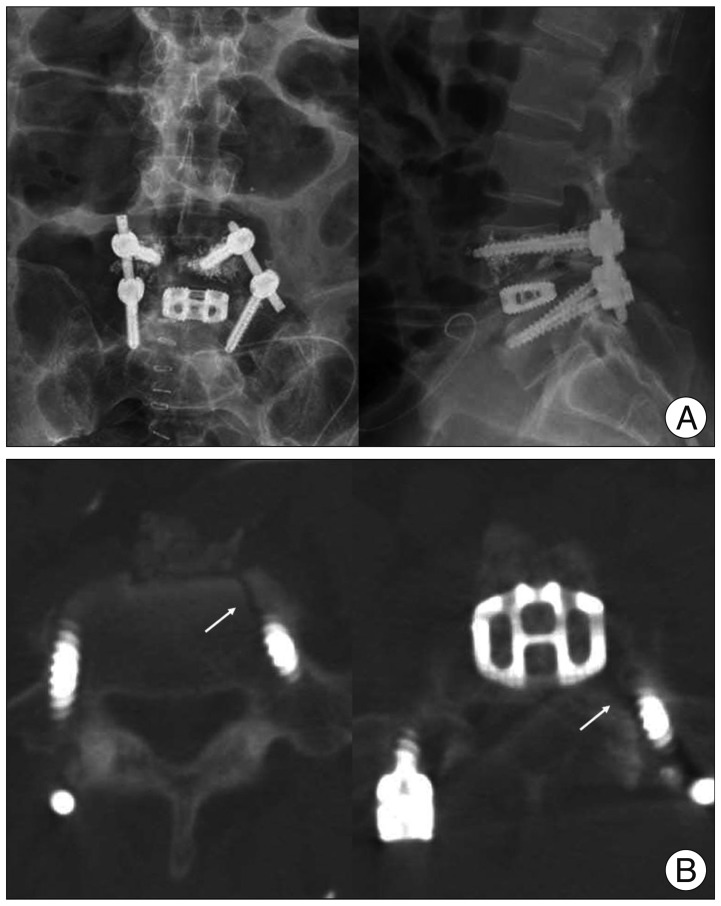 | Fig. 4Plain radiographs (A) and CT images (B) after the first revision surgery. A : The pedicle screws were unstable and replaced with thicker and longer ones, but two L4 screws remained loose. Therefore, cement was used to augment the L4 screws. B : CT images showing the pedicle and lateral body wall fracture in the L5 vertebra (white arrows).
|

After the second revision surgery, the patient showed significant improvement of his symptom except mild left leg discomfort. His gait was improved and the lumbar corset was applied for 3 months. At 6 months follow-up, his left leg discomfort was completely resolved. Radiographs and a 3-dimensional CT scan obtained at 6 months postoperatively revealed a solid fusion at the L4-5 level.
Go to :
DISCUSSION
Fusion rates after the TLIF procedure using cages and bilateral pedicle screws instrumentation are reported to be more than 90%6,14,15). Humphreys et al.9) evaluated patients receiving TLIF in comparison with PLIF and demonstrated that fewer complications occurred after TLIF than after PLIF. Several recent studies have described cases of posterior cage migration after TLIF procedures that were mostly associated with pseudoarthrosis19,22). However, there are few case reports about anterior migration or dislodgement, and the causes included perforation of the annulus fibrosus during the removal of the disc or a feeble condition by spondylodiscitis20,21). In which reports, migration was confirmed intraoperatively. Unlike these reports, our case had completed the initial surgery with good placement of the cage with satisfactory reduction. The authors have inferred that anterior dislodgement of the cage during the follow-up period seemed to result from the high stress at the index level and the abnormal shape of the L5 body.
The patient had a LSTV (Castellvi type IIIa) with a bony union between the transverse process and the sacrum on the left side. Usually, the increased stability between the transitional vertebra and the sacrum can potentially lead to hypermobility above the transitional vertebra5). Hypermobility and abnormal torque momentum at the intervertebral disc are believed to place the disk and facet joints at increased risk of degeneration2,13). It has been postulated that patients with L5 transitional vertebra and isthmic defects in the L4 vertebra have greater risk of anterior slips than patients with L4-5 isthmic spondylolisthesis without transitional vertebra11). Therefore, in our case, isthmic spondylolisthesis combined with a LSTV is considered to have contributed to the reduction loss at the index level during the follow-up.
Commonly, the shape of the vertebral body and the cage could affect cage migration. A recent study showed that banana-shaped cages should be placed anteriorly to avoid cage subsidence, considering regional strength variations of the vertebral endplates7,8). This is supported by a biomechanical study demonstrating that central portions of the vertebral endplates from L3 to L5 are relatively weaker than anterior or posterior portions8). In our case, the cage was positioned ideally on the anterior portion of the intervertebral disc space at the time of the initial surgery. However, the high stress above the transitional vertebra was postulated to make the anterolisthesis recur. In addition, the relatively smaller contact area between the defective superior endplate of the L5 vertebra and the banana-shaped cage might influence the anterior dislodgement of the cage. Even though there have been some experimental studies that the cage shapes do not affect construct stability4,10,16), cage migration could be affected by cage type and positioning1). Therefore, a different type of cage from the banana-shaped ones could have been better for the patient in this particular case. In addition, as appears by this case, a more central location and longer length of a cage is considered to have been safer.
For the removal of the dislodged cage and the treatment of the pseudoarthrosis, the anterior approach was successful, because the revision surgery was not delayed and adhesion around the L4-5 disc was absent. Additional surgery via an anterior approach is a higher risk of complications, but it provides an easier preparation of the endplates, which have been already injured, and enables a larger cage insertion with a greater contact surface19). Several biomechanical studies reported that polymethylmethacrylate augmentation of pedicle screws, bicortical purchase, and replacement of screws with larger diameter are helpful in the setting of screw loosening12,17,18). In our case, all these methods were eventually used to enhance the stability of the pedicle screw fixation during the revision surgery.
Go to :
CONCLUSION
This is a case of anterior dislodgement of a fusion cage after TLIF. In the case of unstable isthmic spondylolisthesis accompanied with a LSTV, the surgeon should be cautious of selecting a fusion cage to be used because especially in cases of the banana-shaped cages there can be a potential of the anterior dislodgement. Additional surgery via an anterior approach may be effectively performed for removal of the displaced cage and reinsertion. Stability at the index segment can be acquired through the anterior cage insertion and the extension of posterior pedicle screw fixation accompanied by the replacement with the larger bicortical screws with cement augmentation.
Go to :
 XML Download
XML Download