

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Bilateral thinning of parietal bone is well known phenomenon since the 18th century4). In the course of time, pathologists, anthropologists and radiologists pointed out this situation1,2). It is a pathological situation, not an anatomical variety1,4). More frequently this condition affects females over 60 years of age with no special reference to race or geographical area1-4). Estimated prevalence is between 0.4-0.5%1). Remodelling of the compensatory spongy bone (diploe), due to erosion on the external table (the compact bone), has resulted in findings of diploe layer waste on histopathologic examination1). Therefore, we aim to present a patient with biparietal osteodystrophy, who had parietal bone fracture and epidural hematoma underneath following a minor head trauma.
CASE REPORT
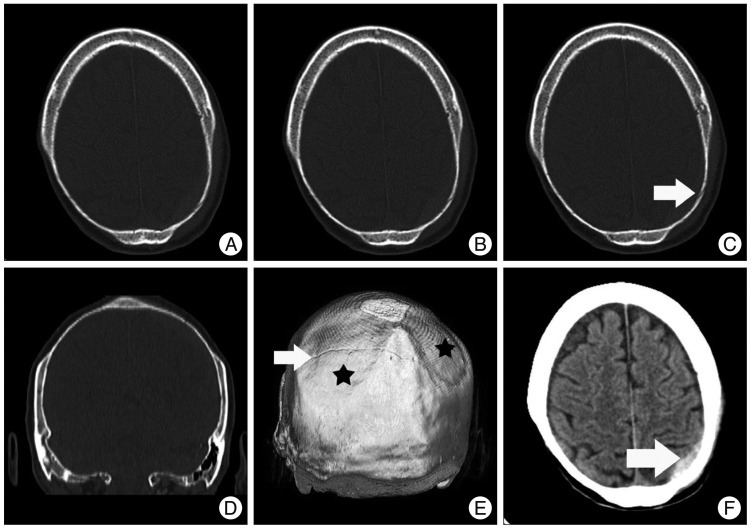
A 78-year-old woman visited to the emergency service with a severe headache after hitting her head to the wardrobe. At first, a neurological examination seemed normal but the patient has undergone computerized tomography (CT) scan because of increasing headaches. The CT scan revealed non-depressed linear fracture on the left parietal bone and epidural haematoma underneath (Fig. 1). Irrelevantly, biparietal bone thinning with lack of diploe layer and external table was pointed out. Patient was consulted to our department with the diagnosis of biparietal osteodystrophy. Patient was treated by the conservative management. No neurological deterioration or a radiological increase of epidural haematoma was observed. Patient was discharged without any problems.
DISCUSSION
Bilateral thinning of parietal bone is a condition that has been known since the 18th century. In the course of time pathologists, anthropologists and radiologists have given special attention to this topic and have carried out many retrospective researches. Current definition was changed by the understanding of that it is not an anatomical variety or result of growing old in time. However, it was described as "senile bone atrophy, senile biparietal atrophy and senile cranial atrophy", firstly by emphasizing atrophy relevant to aging. Histological evidence and new cases with younger ages have changed that point of view1,2,4). Currently, it is described as "biparietal ostedystrophy" by retrospective radiologic researches and histopathologic examinations.
Estimated prevalence is 0.4-0.5% according to radiological scans, case reports and anthropologic researches1). Whereas Cederlund et al.2) reported its prevalence as 0.25-0.8%. Also those researches showed neither relationship to race, climate nor geographical differences1). However, biparietal osteodistrophy occurs mostly in females over 60 years old, in younger ages, male cases have been reported much more than female cases1). However, diagnosed sporadically, there are some family case reports that considered autosomal transmission1).
Clinical presentations show differences in pains in the areas thinning to simple local pain due to fractures that may lead to death4). Review of literature shows that most diagnoses have been done by retrospective radiologic scans such as simple radiography or CT scan.
Radiologic investigations generally reveal oval shaped bone loss in the area between parietal prominence and sagittal suture bilaterally4). Sometimes bone loss enlarges to 8-9 cm area on parasagittal plan1). Unilateral cases were rarely reported. Some authors investigate parietal atrophy under two topics; simple flattening on both parietal bones and groove-like (crater-like) biparietal atrophy1). Simple flattening is considered as the early stage of crater-like biparietal atrophy.
Immunohistopathologic examinations could not determine the leading factor. Examinations exposed relevance with osteoporosis and decreased bone formation instead of increased bone destruction4). However, some studies report that external destruction of bone causes loss of external table and therefore triggers remodelling of diploe layer but that remodelling regressed in time1).
Many theories have been suggested to determine the reason. Also, chronic trauma is one of the considered factors of pathology. That idea was brought forward by archaeologists because they thought that pharaohs' helmet, "Pschent", effected by its pressure. However, even today there are many people who carry load on their heads, the pathology does not exist as before. Recently, muscular traction and aponeurotic friction theory seem unrealistic1).
Either stable cases or progression was reported during follow-up period. Some reports suggest that cranioplasty could prevent the atmospheric pressure effect on brain4).
CONCLUSION
Epidural haematoma underneath parietal fracture due to minor head trauma is generally an unexpected situation. Although our patient had no findings before, incidental minor head trauma on pathologic bone segment led the clinical situation. The absence of external table and diploe layer, old age and female sex are compatible with biparietal osteodystrophy.
 XML Download
XML Download