

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Discal cysts are uncommon, but are capable of causing radiculopathy1). In most cases their removal is easily accomplished, however sometimes the location of the cyst precludes its intraoperative detection17). We describe 2 patients with discal cysts and discuss the efficacy of an intraoperative discography technique for discal cyst location. In our 2 patients, the discal cysts could not easily be identified in the intraoperative field because of their location under the peridural membrane17). We performed intraoperative discography to locate the concealed discal cysts and thereby successfully removed them. Intraoperative discography can be useful, both for locating discal cysts and for confirming whether a cystic lesion is totally removed, or if it has been penetrated, before concluding the operation.
Go to : 
PATIENT 1
A 28-year-old male presented with a several-week history of left L4 radiculopathy. He had sensory abnormalities in the L4 dermatomal area of the left leg, and the straight leg raising test was positive at 50 degrees. Magnetic resonance imaging (MRI) demonstrated a spherical, extradural, cystic mass behind the L3/4 intervertebral disc space, with high signal intensity on T2-weighted images (Fig. 1A, B) and low signal intensity on T1-weighted images.
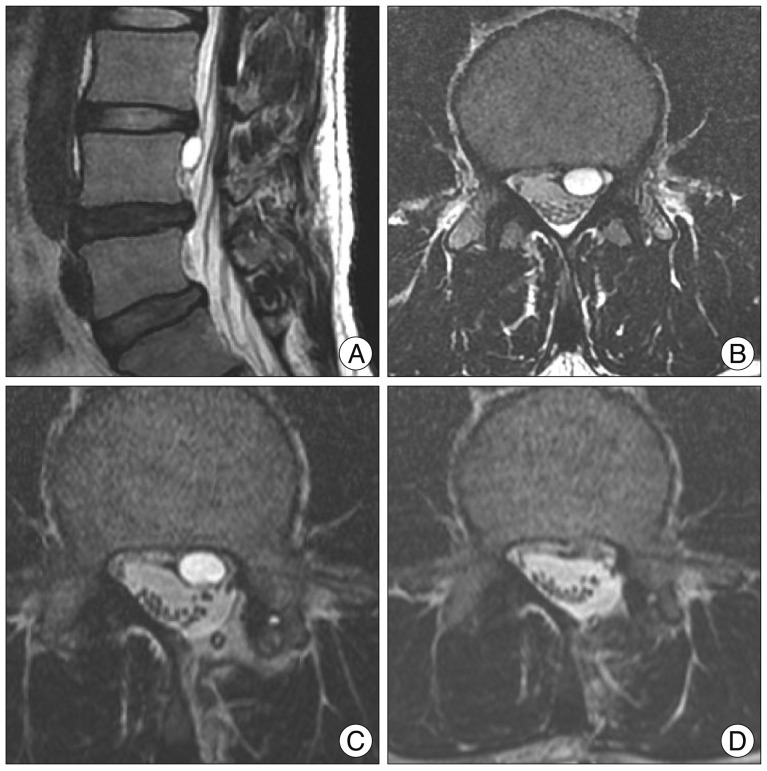 | Fig. 1A : Preoperative sagittal T2-weighted magnetic resonance imaging (MRI) showing a cystic lesion with high signal intensity at the L3-4 level. B : Preoperative axial T2-weighted MRI showing a cystic lesion with high signal intensity at the L3-4 level. C : First postoperative axial T2-weighted MRI showing the remaining cystic lesion. D : Second postoperative axial T2-weighted MRI showing that the cystic lesion has been completely removed.
|
His symptoms persisted after conservative treatment and surgical management was planned. A partial hemilaminectomy was performed and the thecal sac and L4 root were carefully manipulated, but the cyst was not found. It was assumed that the cyst was penetrated during the surgical manipulation. After surgery, the patient's symptoms disappeared but postoperative MRI showed that the cyst was still present (Fig. 1C).
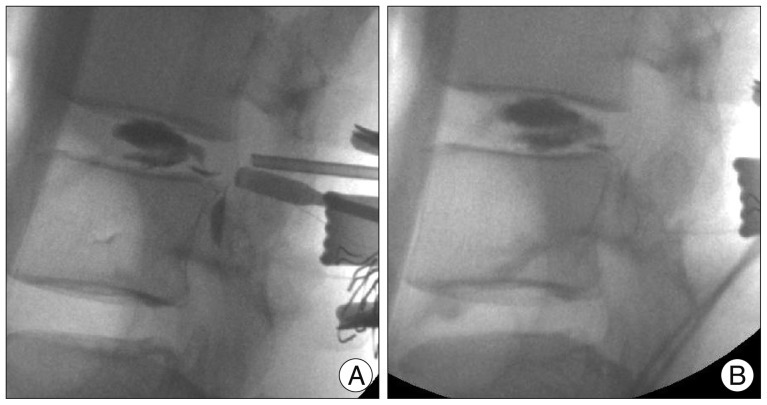
On the first postoperative day, a second operation was performed. Intraoperative discography was performed under C-arm fluoroscopic guidance. A long, 18-gauge needle was inserted into the disc space at the left paracentral region of L3-L4, through the area of the previous laminotomy, and 2 mL of radiopaque dye (Hexabrix, Guerbet Asia Pacific Ltd., Hong Kong) was injected. Care was taken not to injure the thecal sac or the nerve root (Fig. 2A). The bluish cyst was then seen to be located ventrally on the thecal sac, under the peridural membrane. The cyst's location was the likely reason that it could not be visualized during the first operation. In addition, the cyst wall was thick and its margin could not be distinguished from the thecal sac. The discal cyst was penetrated with a 22-gauge needle and the cyst wall was cauterized using bipolar current. A second discography, after removal of the cyst, confirmed that the cyst was no longer present (Fig. 2B). Postoperative MRI confirmed that the discal cyst had been removed (Fig. 1D).
Go to :
PATIENT 2
A 47-year-old male presented with radiating left buttock pain. His symptoms had developed 3 years prior, and had been aggravated 1 week before his presentation. Conservative treatment was ineffective. He had sensory abnormalities in the L4 dermatomal area of the left leg, and the straight leg raise test was positive at 60 degrees. MRI demonstrated a cystic lesion at the level of the L3/4 intervertebral disc space, with high signal intensity on T2-weighted imaging (Fig. 3A, B) and low signal intensity on T1-weighted imaging. The cystic mass, located between the thecal sac and the L4 nerve root, compressed both structures.
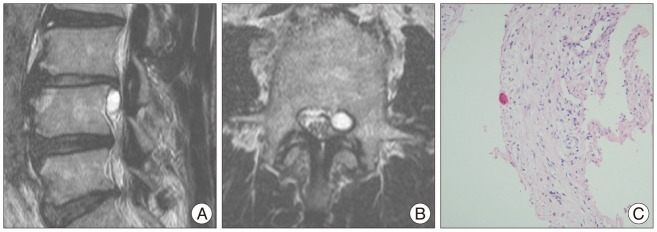
After a left L3/4 partial hemilaminectomy failed to reveal the discal cyst, intraoperative discography was performed. A dark blue, cystic lesion was visualized, compressing the thecal sac and the L4 nerve root. The cyst communicated with the L3/4 intervertebral disc by means of a central annular tear. The cyst was aspirated, then totally excised. The patient achieved complete pain relief after surgery. Histologic examination revealed that the cyst had a fibrotic wall without an epithelial-cell lining (Fig. 3C). Postoperative MRI showed no evidence of any remaining mass lesion.
Go to :
DISCUSSION
A discal cyst is a rare disease entity; in most cases, its clinical symptoms are caused by compression of a unilateral single nerve root. Discal cysts occur at a slightly younger age and at higher intervertebral levels than typical disc herniation12), and imaging studies typically show minimal degeneration of the involved disc. Discography demonstrates a communication between the cyst and the corresponding intervertebral discs, and patients experience severe radiating pain in the affected leg at the time of contrast injection. The cyst contains bloody-to-clear serous fluid1,15).
The pathogenesis of discal cysts is unknown. Chiba et al.1) proposed that they arise from an underlying intervertebral disc injury that causes a fissure in the posterior aspect of the annulus fibrosis. Bleeding from the rich epidural venous plexus may occur in the space between the peridural membrane and the vertebral body. MRI is the modality of choice for the diagnosis of discal cysts. Lee et al.12) reported their typical MRI features : a ventrolateral extradural cyst attached to a lumbar disc; rim enhancement on contrast-enhanced MRI; and occasional extension into the lateral recess.
Several options for treating discal cysts have been reported, but clear therapeutic guidelines have not been established. Most patients are treated by surgical excision, including both microsurgical and endoscopic surgery techniques1,3,7,9,11,12,15,16), but some patients have been treated by computed tomography-guided aspiration4,6,7,10,14); spontaneous regression has also been reported2). Surgical excision remains the therapy most commonly performed for symptomatic discal cysts, with the aim of complete eradication of the fistulous connection between the disc and the cyst in order to avoid recurrence. We chose surgical excision for our 2 patients. In Patient 1, we could not detect the discal cyst during the primary operation because of the cyst's location under the peridural membrane; we performed intraoperative discography to locate the cyst in the subsequent reoperation. In Patient 2, we were easily able to detect the discal cyst using intraoperative discography, but the cyst could not be identified before this intervention.
In most cases, there is no problem identifying and resecting discal cysts. However, as our 2 patients demonstrate, the discal cyst can sometimes be hidden by the peridural membrane as it curves around the sides of the spinal canal, reaching the inside surface of the pedicle5,8,13). The cyst can also be missed if the nerve root is compressed from the direct lateral direction. It can be difficult to locate a pathologic lesion in the limited, narrow microsurgical view if the lesion is not immediately visually apparent.
Intraoperative discography is a very useful technique. It can help to locate a hidden discal cyst by accumulating contrast medium in the cyst, and it can confirm whether a cystic lesion is totally removed or if it has been penetrated before surgery is concluded. It can also evaluate the fistulous communication between the cyst and the corresponding intervertebral disc.
Go to :
 XML Download
XML Download