

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Fusiform aneurysms on the basilar artery (BA) trunk are rare17,24). The microsurgical management of these aneurysms is difficult because of their deep location, dense collection of vital cranial nerves, and perforating arteries to the brain stem9). The endovascular approach is comparatively easy and comfortably compares with surgical treatment. Thus, endovascular treatment is considered as first treatment option in these lesions. Selective occlusion of the aneurysmal sac with preservation of the parent artery is the treatment of choice8). But, some cases, particularly giant or fusiform aneurysms, are unsuitable for selective sac occlusion2,6,15). Therefore, proximal occlusion of the parent vessel is an alternative treatment option. It is important to determine whether a patient can tolerate proximal occlusion without developing neurological deficits.
We report a rare case of fusiform aneurysms in the BA trunk that was treated successfully with endovascular method after confirming bilateral collateral bloods flow through the both posterior communicating arteries, the tolerance of the patient by balloon test occlusion (BTO) with induced hypotension and accompanied by neurophysiologic monitoring (NPM), transcranial Doppler (TCD) and single photon emission computed tomography (SPECT).
CASE REPORT
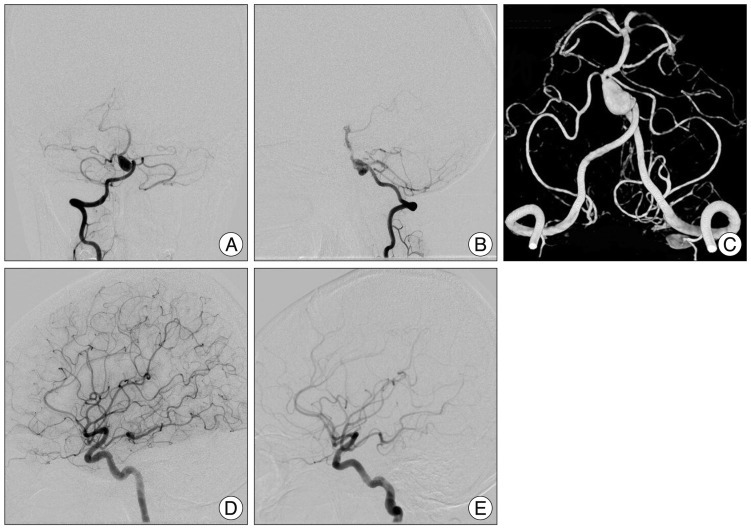
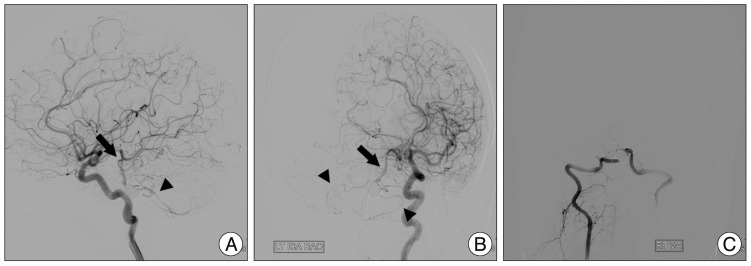
An 18-year-old female suffered a headache for 2 weeks. Computed tomography and magnetic resonance image revealed a fusiform aneurysm on the lower BA trunk. Digital subtraction angiography (DSA) revealed a 7.1×11.0 mm-sized fusiform aneurysm located just below the anterior inferior cerebellar artery (AICA) (Fig. 1). Right side posterior inferior cerebellar artery was not seen. Both posterior cerebral arteries (PCA) and superior cerebellar arteries (SCA) filled normally. Both posterior communicating arteries (PComA) were patent and the diameter of both arteries was more than 1 mm in diameter (Fig. 1). For the proximal portion of the aneurysm forming a severe acute angle, flow diversion with multiple stent is difficult to enforce. Endovascular coiling of aneurysm with occlusion of dysplastic parent vessel is planned if the patient tolerate complete preoperative occlusion test.
Preoperative tests
BTO
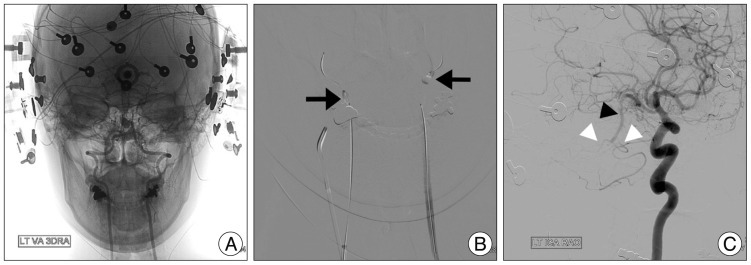
The location of aneurysm is just distal to vertebrobasilar junction and proximal to the origin of AICA, and it is somewhat related perforating artery injury to perform a BTO at basilar artery. We planned the BTO on both vertebral arteries. BTO was performed under local anesthesia and accessible for neurological examination. At the time of the BTO, the neurological status of the patient was continuously monitored by a trained neurosurgeon that assessed speech, motor strength, sensory extinction, and level of alertness (Fig. 2).
Bilateral femoral artery (FA) punctures were performed and guide catheter placed in both vertebral arteries (VA). Additional right FA puncture was performed for diagnostic cerebral angiogram. The patient was anticoagulated by the intravenous injection of 5000 IU heparin. Over-the-wire microballoon (Hyperfrom, Hyperglide; ev3, Irvine, CA, USA) was used for BTO and these balloons were located at VA just around the C2 vertebra foramen (Fig. 2). The balloon was then inflated. Complete balloon occlusion of VA was verified by a proximal contrast injection. The BA and both AICAs were visible through the retrograde blood flow from the PComA, which were visualized by an angiographic injection in the both internal carotid artery (ICA).
Bilateral BTO of the each VA were performed over 20 min under a normotensive state. Baseline blood pressure was 109/72 mm Hg (mean arterial blood pressure, 84.33 mm Hg). The patient tolerated 20 minutes under the normotensive state and hypotension was induced pharmacologically by the intravenous infusion of nicardipine (starting dose of 5 mg/hr with 2.5 mg/hr increase every 5 min if the blood pressure did not reach the target range). After the mean arterial pressure was reduced by 20% of baseline (92/56 mm Hg; mean arterial blood pressure, 68.0 mm Hg), hypotension was maintained for 20 minutes.
TCD
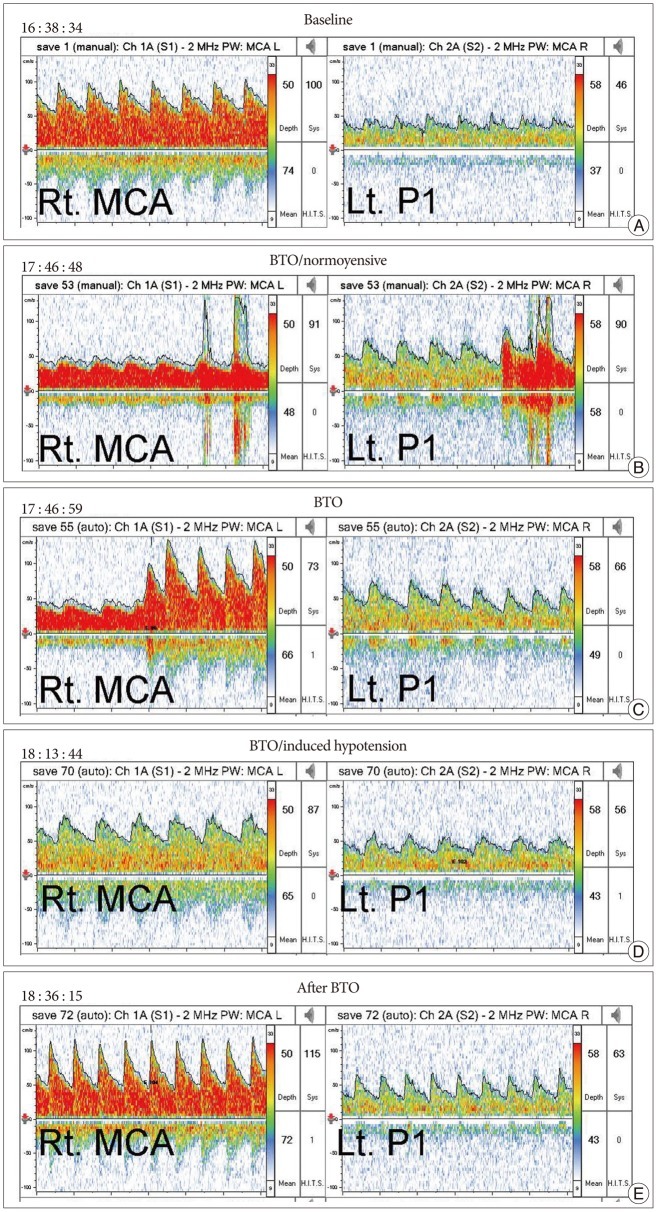
Before BTO, the patient underwent a complete TCD investigation. The patient-customized TCD headset was mounted. BTO was performed with concomitant monitoring of the blood velocity and direction of the blood flow in the middle cerebral artery (MCA) and P1 segment of the PCA.
Results of preoperative test
BTO
DSA during BTO, the right ICA angiogram showed retrograde filling of the distal part of the BA, PCAs, SCAs and AICASs through the PComA (Fig. 2). The patient tolerated 20 minutes under the normotensive state and induced hypotensive state with no developing neurological deficits.
TCD
Baseline mean blood flow velocity of MCA was 74 cm/s (Fig. 3). The velocity during BTO dropped immediately to 48 cm/s upon balloon inflation, but returned to the baseline value (72 cm/s) within several seconds without additional treatment and was maintained during the BTO. After induced hypotension, it dropped to 65 cm/s; the patient tolerated in induced hypotensive condition. After deflation of the balloon, the velocity of the MCA recovered to the baseline value. The reduction of flow velocity was 2.7% under the normotensive state and 12.2% under induced hypotensive state.
SPECT
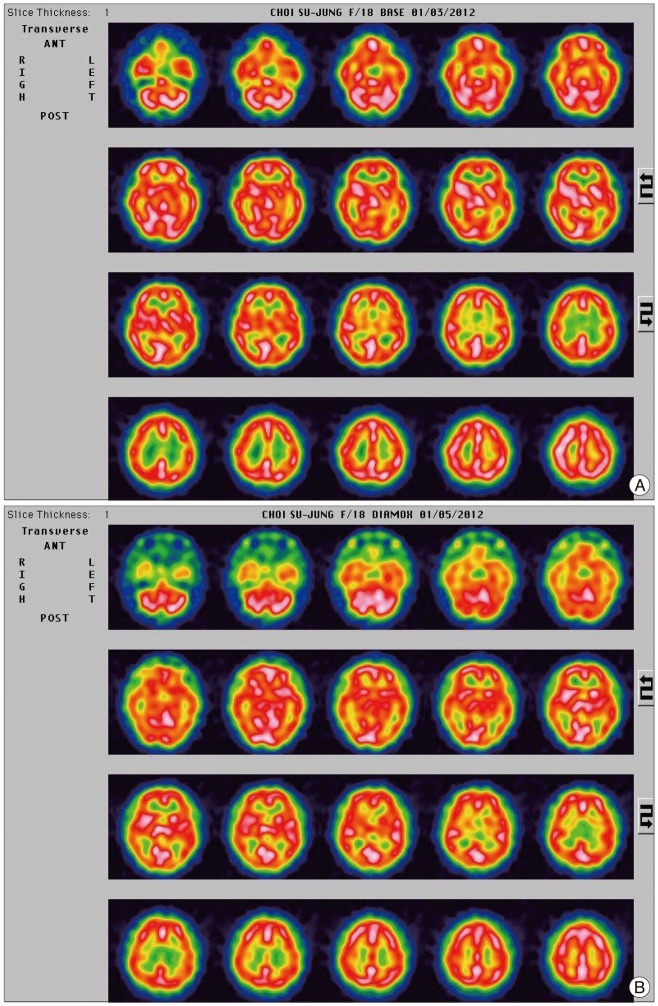
Baseline SPECT images did not show any focal perfusion reduction (Fig. 4). SPECT images obtained after BTO also did not showed hypoperfusion of the cerebral hemisphere and cerebellum compare to the baseline SPECT.
Coil embolization
Coil embolization was performed with multiple coils in the usual way. Care was taken to preserve the both AICAs, which arose close to the distal aspect of the aneurysm. After coil embolization, a left side ICA angiogram (Fig. 5) showed regrograde filling of the BA (arrow) and both AICAs (arrowhead) through the PComA. A right side VA angiogram showed complete obliteration of the aneurysm and no filling of the BA though the VA.
DISCUSSION
Fusiform aneurysms in the BA trunk are rare17,24) and their prognosis is generally bleak. Left untreated, progressive brain-stem compression or subarachnoid hemorrhage may result, with survival as low as 20% after 2 years4,14). Unfortunately, the surgical treatment is very difficult because of the deep location of the aneurysm, dense collection of vital cranial nerves, and perforating arteries to the brain stem9). However, the endovascular approach to this area is comparatively easy, so the first choice of treatment has changed over the last 10 years7,23,25). Selective occlusion of the aneurysmal sac, with preservation of the parent artery, is the treatment of choice8). But, some cases, particularly giant or fusiform aneurysms, are unsuitable for selective sac occlusion2,6,15). In these circumstances, proximal occlusion of the parent vessel is an alternative treatment option. It is important to determine before the operation whether a patient can tolerate arterial occlusion without developing neurological deficits. Although there is no way to guarantee absence of complications after the occlusion of the parent vessel, various preoperative occlusion tests for the selection of patients who can tolerate the loss of the parent artery have been developed.
Angiographic finding
Tolerance of the proximal arterial occlusion depends on collateral flow to distal branches. The diameter of the PComA is an important predictor of success of basilar occlusion4,16,20). Steinberg et al.20) reported that a PComA diameter greater than 1 mm is significantly related to tolerance of BA occlusion, and a favorable long-term clinical outcome. But, in one study, 8% of patients with two large PComAs (both posterior communicating arteries exceed 1 mm) experienced ischemic complications20). Pelz et al.16) reported a trend in which patients with a large PComA will have a better clinical outcome than patients without a large PComA, but the finding was not statistically significant. Also, retrograde filling of the BA by collateral flow from the anterior circulation is an essential factor for parent artery occlusion.
BTO
Other predictors of tolerance include normal baseline cerebral blood flow and tolerance of balloon occlusion1,10,11,19). Linskey et al.11) conducted a systematic review of 254 patients in five studies in which an ICA was therapeutically sacrificed without BTO, and reported an average stroke rate of 26% and mortality rate of 12%. This contrasted with a review of 262 patients in eight studies in which the ICA occluded after performed a BTO with an average stroke rate of 13% and mortality rate of 3%. This reduction in stroke and death rate reached statistical significance, but the complication rate was still high. Also, the false negative rate of the normotensive BTO was about 5%19). To reduce the complication rate, hypotension-induced challenge was introduced19). When the vessel is occluded, and no deficit occurs in a normotensive patient, the blood pressure is pharmacologically lowered to a target pressure. Standard et al.19) reported that parent artery sacrifice in 19 patients after a clinically tolerated hypotensive BTO resulted in no hemodynamic ischemic infarction.
TCD
Sonographic evaluation of the MCA is obtained before and after balloon inflation. Mean blood flow velocity that does not decrease more than 30% is highly predictive of tolerance to carotid occlusion5). Reversal of flow in the P1 indicates a likelihood to tolerate the BTO in cases of basilar occlusion18).
SPECT
The 99m Tc-HMPAO SPECT procedure is an alternative indicator22,26). In this approach, 99m Tc-HMPAO is injected intravenously 10 min after the balloon is inflated. After the BTO is completed, SPECT scanning shows activity from the tracer, and asymmetry or difference of the baseline study is detected qualitatively by visual inspection of the scan. Universally, it does not allow for accurate quantitative measurement of the cerebral blood flow (CBF). But, the brain perfusion index can be converted to a mean CBF value13). A decrease of more than 10% of regional CBF in the BTO study compared with the baseline study is considered to be significant enough to take additional measure of bypass grafting before performing the occlusion26).
NPM
Continuous electroencephalography monitoring is done throughout the procedures. Slowing or other deviation from baseline conditions can be secondary signs of developing ischemia3). Somatosensory evoked potential and brainstem auditory evoked potential monitoring can be tested. The cortical responses are recorded and the timing and amplitude of the response indicated cortical function21).
Neurological examination
The main criteria for success with BTO are clinical neurological testing. In addition to simple neurological testing during BTO, a battery of standardized neuropsychological tests are given to test higher cortical functions12).
CONCLUSION
We report a rare case of fusiform aneurysm on BA trunk treated with endovascular coiling of the aneurysm with parent vessel occlusion after complete preoperative occlusion test. This method may provide an efficient and safe treatment modality. But, it can potentially lead to postoperative ischemic complications. Prior to the procedure, it requires meticulous evaluation of the aneurysm morphology and collateral pathway, multiple tests to predict hemodynamic state, and a provocation test to achieve a complete and safe result before the parent artery occlusion.
 XML Download
XML Download