

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A malignant peripheral nerve sheath tumor (MPNST) is a sarcoma that arises from peripheral nerves or cells of the associated nerve sheath (Schwann cells, perineural cells, fibroblasts). The term "MPNST" has substituted previously used terms such as malignant schwannoma, neurofibrosarcoma, and neurogenic sarcoma1,2).
The MPNSTs comprise approximately 5% to 10% of all soft tissue tumors and have an incidence of 0.001% in the general population and the etiology is unknown. However, more than half of MPNST cases develop in patients with neurofibromatosis type-1 (NF-1) and there is a higher incidence in patients that have undergone prior radiotherapy1,2,5,8,13).
MPNSTs are most likely to metastasize to the lungs, followed by the bone and finally the pleura, but, spinal cord and brain metastasis is very rare in non-NF-1 MPNST3,7). The authors report a very rare case of spinal cord and brain metastasis of MPNST in the lumbar spine that occurred in a 18-year-old man without NF.
Go to : 
CASE REPORT
Presentation
An 18-year-old man presented initially with a 6-month history of low back pain that worsened over time. One month prior to admission, the patient developed radiating pain to his anterior thigh. Neither Café au lait spots nor neurofibromas were seen and his family history was absent of NF-1.
The neurologic examination showed normal motor power in his lower extremities. Magnetic resonance imaging (MRI) showed a paraspinal mass that extended from the central space of L2 to the right psoas muscle through right L2-3 foraminal space. It was an asymmetrical dumbbell shaped mass and the thecal sac was displaced left by the mass. The mass showed iso-signal intensity on T1-weighted images and mixed signal intensity on T2-weighted images. Strong enhancement was visible after gadolinium injection (Fig. 1). There was no evidence of bony erosion.

Surgery
The patient underwent surgery using a posterior approach. A paramedian incision was made from the L1 to L4 and we exposed the right L2 and L3 lamina with transverse process. Right L2 hemilaminectomy was performed using a high speed drill and kerrison rongeur to expose the thecal sac. For removal of intradural portion, the thecal sac was incised. The mass was soft and slightly reddish. The margin of mass was relatively distinct from neural tissue, thus gross total resection was possible under microscopic view. To remove the mass extended to the psoas muscle, the right transverse process of L2 and L3 was resected and the mass was visible. Piecemeal resection of the mass was performed and gross total resection was achieved. Frozen biopsy was reported as schwannoma.
Postoperative course
After the operation, his symptom had improved. However, a few days later, his confirmed pathologic report was presented as MPNST (Fig. 2). The contrast-enhanced MRI was followed at 1 month after the operation and revealed a total removal of tumor (Fig. 3). We recommended the postoperative radiotherapy for prevention of local recurrence. However, the patient declined the external beam radiation due to the fear of potential radiation risk. Six months after surgery, the patient revisited our clinic with a moderate headache. Contrast-enhanced MRI was obtained including brain and spine for workup. Spine and brain MRI showed that the tumor recurrence with leptomeningeal, multiple spinal cord and brain metastases (Fig. 4). Complete surgical clearance of the tumor was not technically feasible, owing to the multiple metastases. Therefore, the patient was referred for adjuvant chemotherapy. In addition, intrathecal chemotherapy was performed. However, no significant effect was observed and the patient's condition deteriorated gradually. After 4 months of chemotherapy, he was referred to the hospice hospital and died within a month.
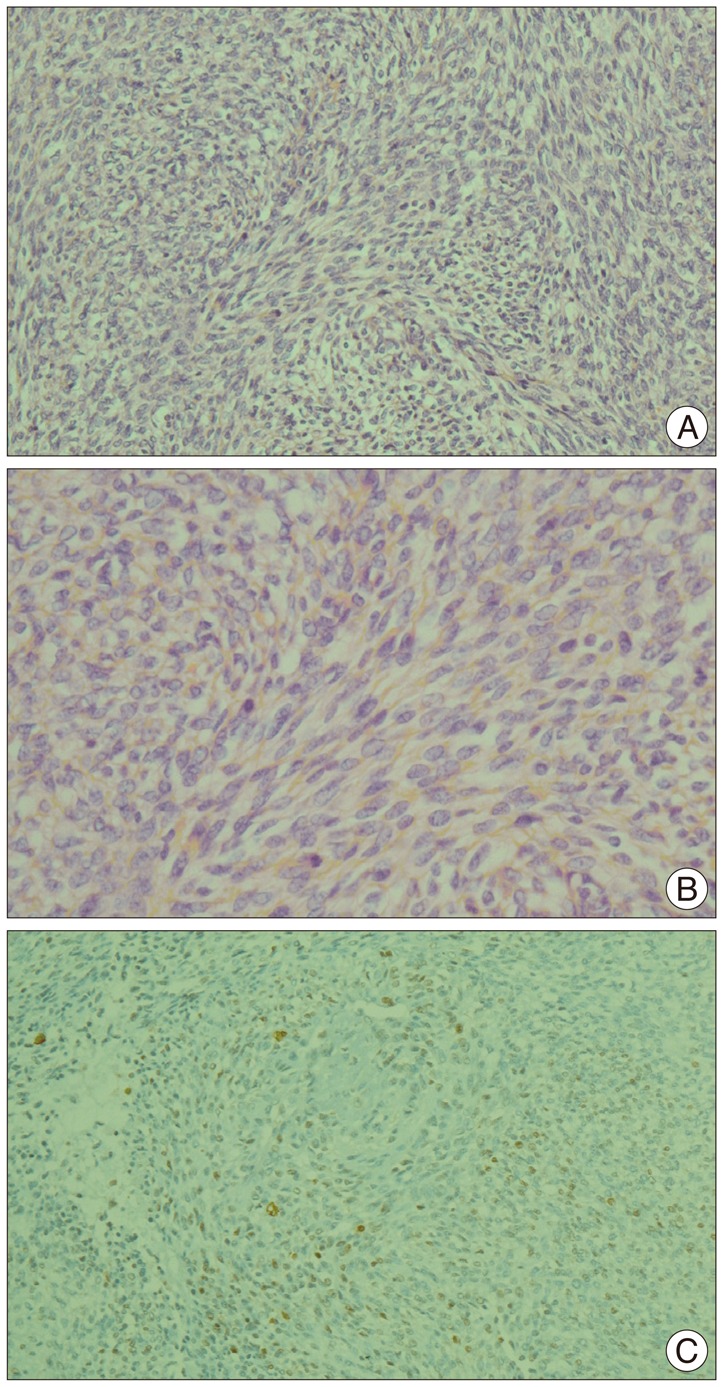 | Fig. 2A : Photomicrographs of the mass demonstrating a spindle cell tumor with high cellularity and a fasciculating growth pattern (hematoxylin and eosin; original magnification ×200). B : Round cells with spindle or fusiform cells appear well a high resolution level (hematoxylin and eosin; original magnification ×400). C : Tumor cells showing immunopositive for S-100 protein (original magnification ×200).
|
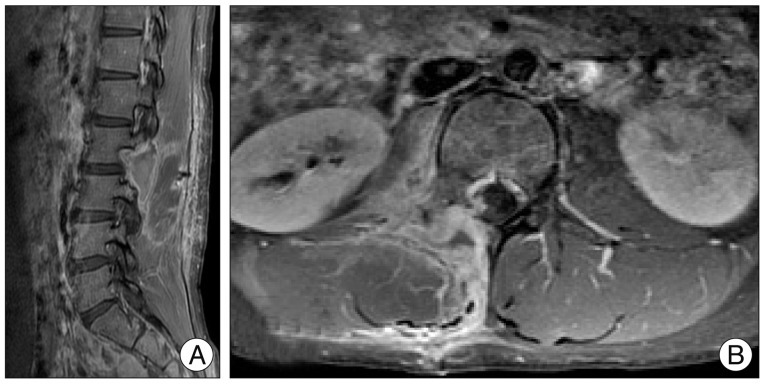 | Fig. 3Post-operative T1-weighted magnetic resonance imaging (MRI) obtained after contrast administration showing gross total resection of the tumor. A : Sagittal MRI. B : Axial MRI.
|
 | Fig. 4Magnetic resonance imaging (MRI) showing spinal cord and brain metastasis of MPNST (6 months after surgery). A : T2-weighted sagittal image showing multiple edematous infiltration of spinal cord. B : Contrast enhanced T1-weighted sagittal image showing multiple tiny enhancing dot lesions. C : T2-weighted sagittal brain MRI showing edematous infiltration on pons and medulla. D and E : Contrast enhanced T1-weighted sagittal and axial images showing small enhancing lesions in the right upper pons. MPNST : malignant peripheral nerve sheath tumor.
|
Go to :
DISCUSSION
Non-NF-1 MPNSTs are very rare and the occurrence of MPNSTs occurring in adolescents is very rare. MPNSTs generally occur in adulthood typically between the ages of 20 and 50 years of age. Approximately 10-20% of cases have been reported to occur in the first 2 decades of life, with occasional cases involving infants as young as 11 months of age5,6).
The metastatic patterns of non-NF-1 MPNST have not been well reported. Hruban et al. described 43 patients with MPNST and of these patients, 28 (65%) had distant metastasis3). Sites of metastasis included the lungs (22 cases), bone (9 cases), pleura (6 cases), retroperitoneum (4 cases), diaphragm (3 cases), inguinal lymph nodes (2 cases), liver (2 cases), chest wall (2 cases), soft tissue (2 cases), pulmonary hilum, pericardium, thyroid gland, and adrenal gland (1 case each). Baehring et al. described 11 distant metastasises in 54 patients with MPNST that included metastases to lymph nodes, pleura, lung, liver, adrenal gland, leptomeninges and brain7). William et al.4) reported a non-NF-1 MPNST case of metastasis to the spinal cord4). Our case showed that leptomeningeal, spinal cord and brain metastasis of non-NF-1 MPNST for relatively short period after tumor removal in young male patient, reflecting aggressive nature of this malignancy.
The mainstay of treatment is surgical resection. The outcome with respect to both local recurrence and distant metastasis largely depends on grade of surgical excision. Radiation therapy combined with wide surgical excision offers statistical significant reduction in the rates of local disease recurrence. However, it has not had a meaningful reduction in either rate of distant metastasis or overall survival15). Benefit of chemotherapy is unproven and its application is limited to high grade metastatic disease3). Recently, the results of using adjuvant chemotherapy have been reported with limited successes. The Italian and German soft tissue sarcoma cooperative group reported an overall pediatric response rate of 45%, with the highest response noted within the ifosfamide group9,11,12).
The recurrence rate for MPNSTs has been reported to range from 40-68%7,10,14). The 5-year survival rate has been reported at 16-52% and a favorable prognosis has been related with complete surgical excision of the tumors that are sized less than 5 cm7,10). Historically, MPNSTs have been difficult tumors to treat due to their inherently aggressive nature and dismal prognosis.
Our patient underwent complete surgical excision, but the patient was not treated with radiotherapy. Follow-up images revealed multiple spinal cord and brain metastases. The patient was managed with chemotherapy, but expired several months later. Despite complete surgical excision, the MPNST progressed rapidly and aggressively.
Go to :
 XML Download
XML Download