

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Proximal catheter obstruction is known to be the most common cause of malfunctioning of ventriculoperitoneal (VP) shunt followed by infection and disconnection14,17). The optimal position of the catheter tip was focused to reduce potential occlusion of proximal catheter by ventricular parenchyma or choroidal tissues1,4,12). Many studies including Tuli et al.22) have shown that a ventricular catheter tip surrounded by cerebrospinal fluid (CSF) could decrease the risk of shunt failure25).
Accurate placement of ventricular catheter is related with both proper insertion trajectory and proper catheter tip positioning. So recently, many studies have validated accuracy in VP shunt with the development of frameless neuronavigation in the field of neurosurgery2,25). However, it has not clearly proven that the role of the catheter position using navigation system on failure rates. The authors conducted a retrospective study of navigated shunt placement about real impact on clinical shunt failure rates, comparing with standard shunt placement.
MATERIALS AND METHODS
Patient population and study design
A retrospective analysis was performed on 72 patients who underwent first VP shunt surgery at our institution within four years from October 2007 to September 2010. All adult and pediatric patients with hydrocephalus of any origin participated in this study. Patients with slit ventricles and those with revision cases were excluded to minimize selection bias.
Each patient had a precise chart review with multiple variables including age, causes of hydrocephalus, the number of shunt revisions, interval time between the first shunt operation and revision, and reason for shunt failure. All patients had preoperative and postoperative brain imaging to reveal the outcomes of shunt surgery.
All patients were divided into 2 groups according to the use of electromagnetic (EM) navigation on surgery. The first group received surgery using EM navigation (Stealth Station Axiem navigation system, Medtronic Incorporation, Louisville, USA) for routine shunt placement. The second group had catheters inserted using manual method with anatomical landmark. Each of shunt revision cases was reconsidered focusing on the causes of shunt failure and catheter position. Patients with shunts were followed up for more than 3 months or until the shunt failure in both groups.
Statistics were generated such as percentages and mean/median values by the data collected from the patients' medical records. Data were analyzed by using statistical methods on the Statistical package for the social sciences version 19. Statistical significance was set at p<0.05.
Surgical techniques
Shunt procedures were performed by neurosurgeons with various training levels. The valve type and catheter were determined depending on the surgeon's preference. In the standard group, skin incision and trepanation of the cranium were done by using anatomical landmarks like Kocher's point or Frazier's point. Ventricular catheter length was determined based on surgeon's measurement using brain computed tomography (CT) imaging. In the EM group, preoperative data acquisition in 3 planes was obtained by CT or magnetic resonance imaging. The dynamic reference frame (DRF), a magnetic field detector within the navigational field, was implanted in an area away from the proposed catheter entry site like Kocher's point or Frazier's point (Fig. 1). After system registration, the surgical plan could be created from the entry site to the final tip position of catheter. The ventricular catheter was placed over the guiding stylet which the detector coils wrapped around the tip of it. The complex was intended to penetrate the ventricular wall along the planned pathway.
Grading system of shunt placement
Proximal catheter position was graded on postoperative brain CT imaging on each case. All patients were graded according the following 3-point scale developed for this study (Fig. 2) : 1) Grade I; catheter tip position free-floating in CSF, away from ventricular wall or choroid plexus, 2) Grade II; catheter tip touching choroid plexus or ventricular wall, 3) Grade III; tip within parenchyma or failure to reach the intraventricular space.
RESULTS
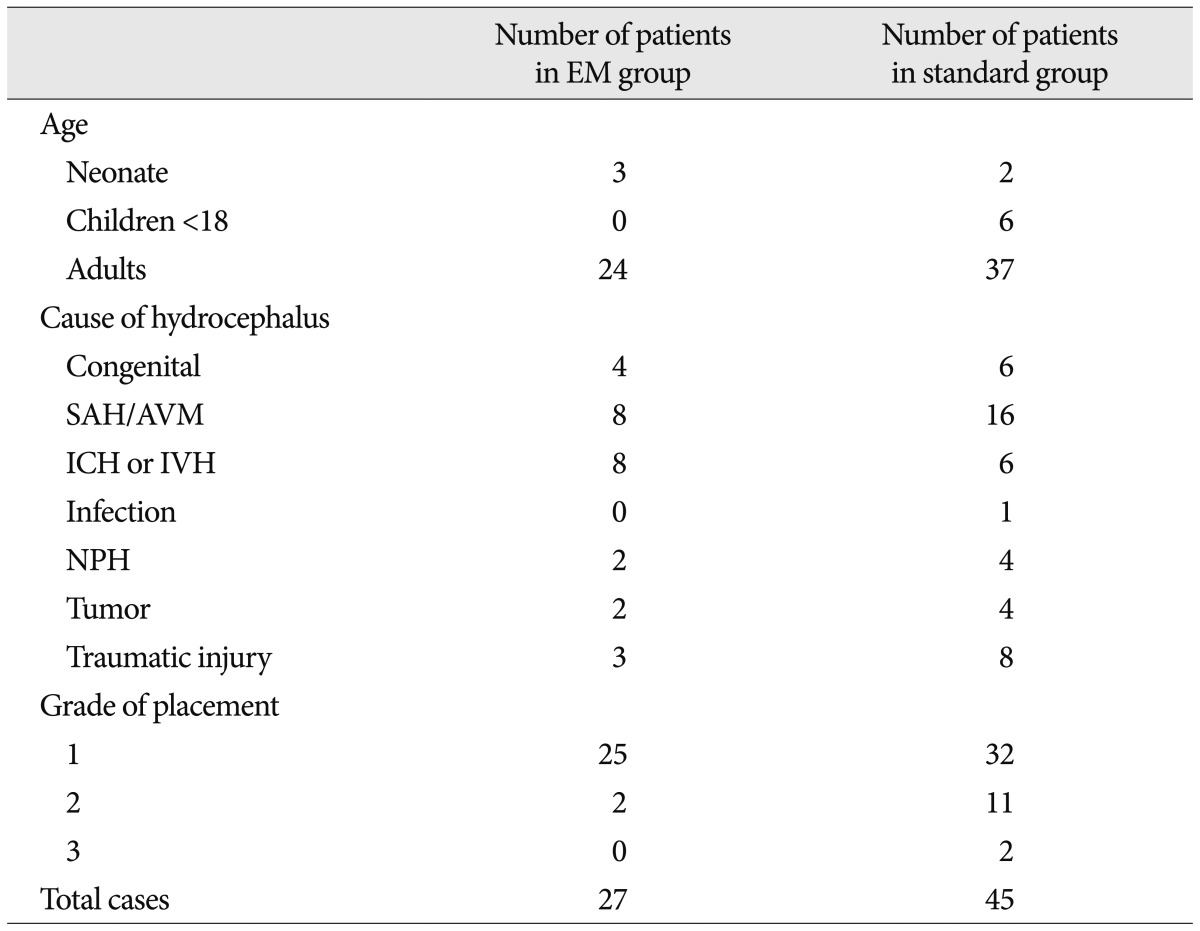
A total of 72 patients were participated in this study, 27 with the EM navigated shunts and 45 with the standard shunts. Eleven patients were children (11% of in the EM group. as 17% of the standard group) and 61 patients were adults. Patients had numerous causes from congenital anomaly to spontaneous or traumatic intracranial hemorrhage. Time interval of follow-up period was various from a day to 20 months. The baseline characteristics of the study patients are shown in Table 1.
Grade of shunt placement
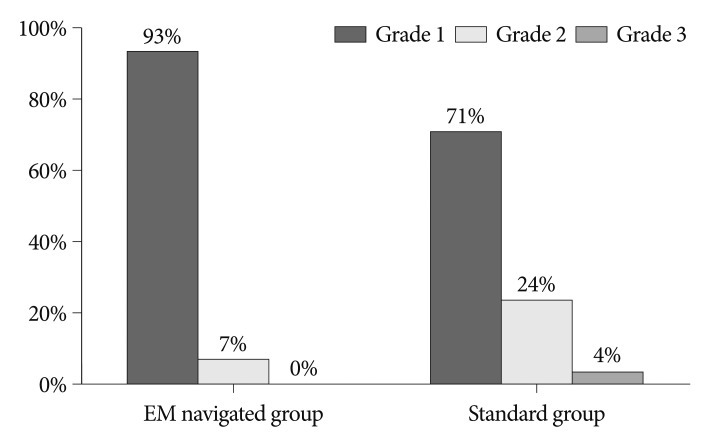
Grade I was found in 25 patients (93% of 27 patients) from the EM guided group and 32 patients (71% of 45 patients) from the standard group. The EM navigated shunts had catheter tip more free floating in CSF (Grade I) compared with one of the standard shunts (p=0.03, chi-square test). Eleven patients (24%) in the standard shunts were classified as grade II compared with 2 patients (7%) in the EM navigated group. Only 2 shunts (4%) were determined to be grade III in the standard group. This result showed that the EM navigated group can get the high potential to have optimal catheter tip position within ventricle (Fig. 3).
Shunt failure rate and characteristics of failure cases
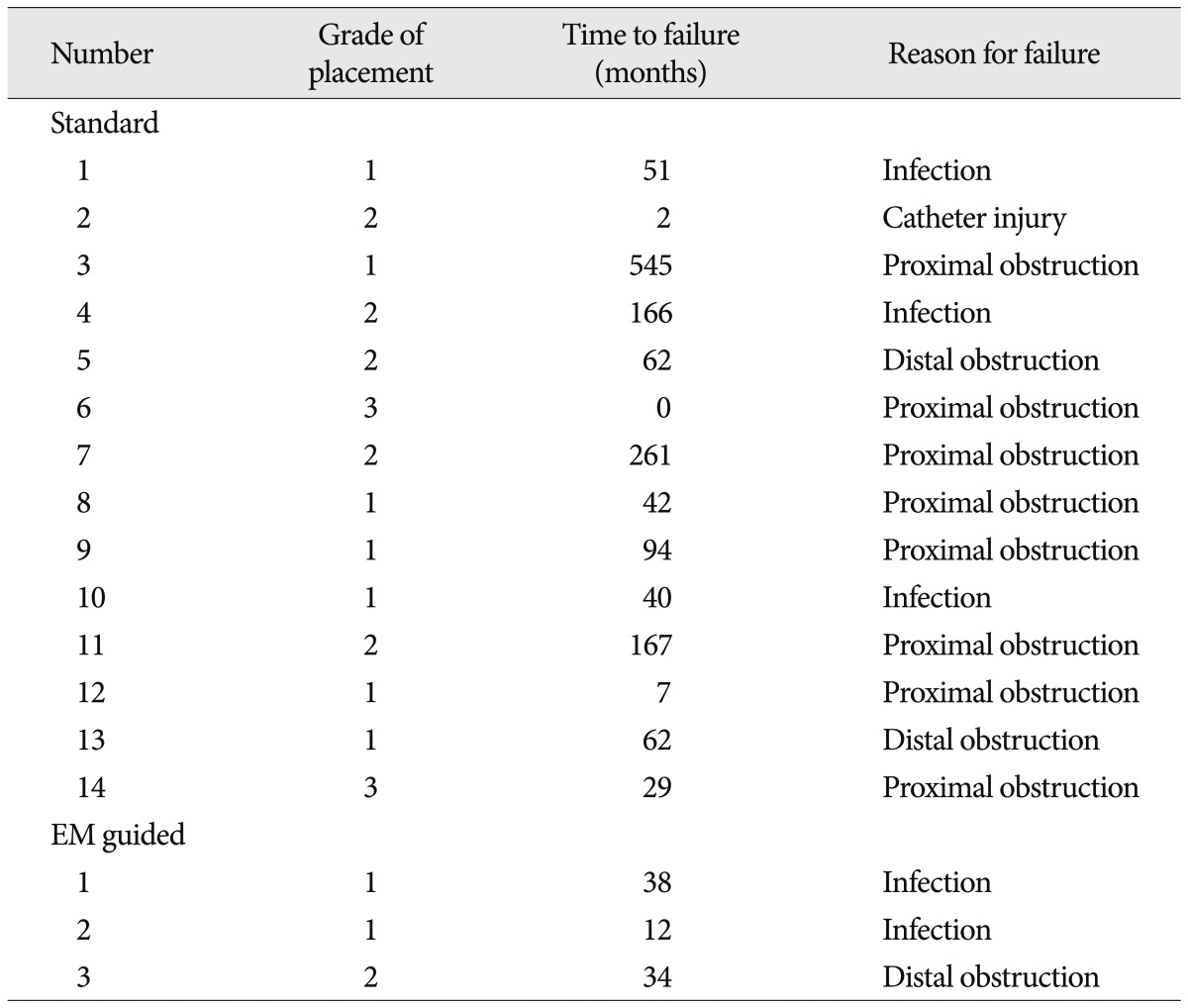
The Table 2 showed characteristics of shunt failure cases. There were 14 shunt failure cases (31%) in the standard group compared with 3 cases (11%) in the EM group. The most common cause of shunt failure in the standard group was proximal obstruction comparing with no revision case from proximal obstruction in the EM navigated group (p=0.020, chi-square test). For distal obstruction, there was higher rate of revision in the standard group (6.7%) than the EM group (3.7%). Similar result of shunt failure rate between 2 groups was revealed with infection. Comparison of distal obstruction and infection showed no statistically significance (distal obstruction p=0.879, infection p=0.905).
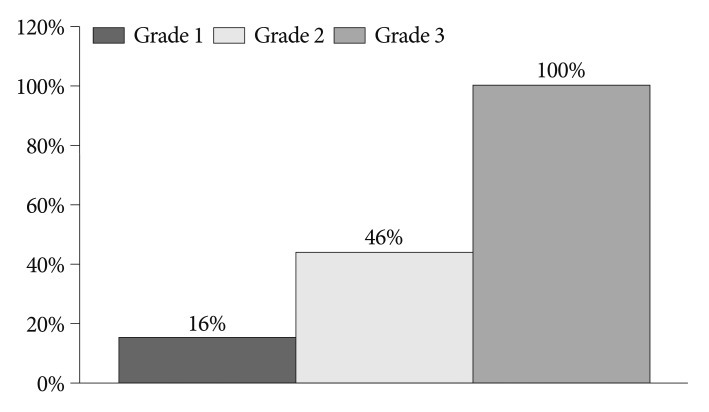
Shunt failure rate according to catheter position
Fig. 4 shows comparison of failure rate among the grades. In grade I, about 16% of cases received revision surgery, as 46% of grade II. Two shunts were included in grade III and those cases all required shunt revision (p=0.002, chi-square test). When compared in terms of proximal catheter position on each group, grade I tended to have lower risk of revision. 2 patients (8%) of grade I and 1 patient (50%) of grade II needed shunt revision on group 1. In group 2, there was growing trend of revision rate according to increase of grade. Revision surgery was performed on 7 patients (21%) of grade I, 5 patients (47%) of grade II and 2 patients (100%) of grade III.
Proximal obstruction was seen in 8 patients in the standard group, especially 100% (two of two patients) in grade III, 15% (2 of 13 patients) in grade II and 5% (3 of 57 patients) in grade I. In the other hand, there was no proximal obstruction in the EM group.
Statistical considerations
This study has several statistical limitations. The number of the samples was too small to represent the population of shunt patients. And it was necessary to consider other factors that might have influenced the results. However, we tried to include patients who had various factors as possible. Other factors were already proven to have no statistical significance except catheter tip position by using multiple regression analysis (age : p=0.138, sex : p=0.430, cause : p=0.226).
The type of shunt could be an important factor to affect the catheter function, but there was insufficient consideration about that point in this study. There has been no specific study to confirm the relationship between shunt types and shunt obstruction up to the present except Tuli et al.21) assumed many factors to have effect on shunt failure including valve type and shunt type. They verified that shunt valve itself could not be a predictor of shunt revision using the multivariable model. However, it would be challenging to prove that shunt type is related with catheter obstruction on the basis of valve's composition. And even if same type of valve was used, shunt valve pressure could make another bias.
DISCUSSION
According to the results of the previous studies, various methods have been suggested to improve the accuracy of catheter tip position. Pang and Grabb15) described a method of calculating catheter length based on bony landmarks on skull radiographs and a shunt placement by free-hand passage using simple stereotactic guidance and palpable surface anatomy. Serlo et al.18) ascertained the catheter position using X-ray imaging by filling the catheter with contrast medium. Neuroendoscopic procedures have also been used effectively16,24). Kestle et al.13) compared the revision rates after endoscopically versus non-endoscopically placed ventricular catheter. Despite placement of catheter tip under direct vision, that study concluded no differences in failure rates between 2 cohorts because burr hole and catheter trajectory were still based on anatomical landmarks1,11).
Frameless stereotaxy has been shown to be helpful for precise location of catheter tip and avoiding unnecessary injury to brain tissue, leading to prevent repeated shunt revisions in children with slit ventricles8,9,18). This study has demonstrated that neuronavigation in the placement of ventricular catheters assures optimal catheter position within ventricles, reducing revision rate in not only special cases, but also general shunt surgeries.
VP shunts are still often complicated by malfunction, predominantly with proximal catheter obstruction despite improved surgical equipment and operative skill10,14,19,25). About 30% to 50% of shunts fail within the first year and only 30% to 37% of shunts survive for 10 years without revision3,21,22,25). Choroid plexus has generally been considered to be the most frequent cause of ventricular catheter obstruction4,12,14,17). It is well known that the ideal placement of the proximal catheter tip is the frontal horn away from the choroid plexus5,7). The obstruction of catheter tip is caused by connective tissue, inflammatory changes, and foreign bodies which are found frequently at the ventricular end. Astrocytes and fibroconnective tissues are especially capable of proliferation. They may fill the side holes in the 15 mm from their tip and the inside of the catheter, leading obstruction of catheters2). Choroid plexus and ependymal cells also have proliferative capability under some conditions. Collins et al.6) frequently found choroid plexus in catheter tips placed in behind the foramen of Monro, but ependyma predominated in catheters placed in front of it.
A ventricular catheter tip surrounded by CSF decreased the risk of shunt failure to one-fifth, whereas a catheter tip touching the brain decreased the risk to one-third, compared with a catheter tip surrounded by brain tissue21,25). The significant relationship of tip position and shunt failure rate has already reported in our study. There might be several other factors to affect shunt catheter obstruction like type of catheter.
Although it is already demonstrated that endoscopically guided catheter insertion could get intended position of the tip with controversy, image guidance like neuronavigation system may be helpful in determining the entry point and approach trajectory before and during the procedure17). The EM group of this study has been found more in grade I, representing the close relationship of navigation and catheter position. Therefore, the formula can be established that use of EM navigation lead an ultimate catheter placement, resulting decrease of shunt failure rate.
There are several disadvantages to frameless neuronavigation which include the prolongation of operation time and dependence on expensive technology8,23,25). More operation time can have risk to increase intraoperative infection rate. In fact, 5 to 10 minutes can be required to install and to register the navigation by skilled person11). Stieglitz et al.20) described that the additional time needed for preparations did not exceed 15 minutes with their experiences. The DRF can be placed while anesthesia personnel are obtaining intravenous access1). The other problem is that frameless stereotaxy is expensive program. It requires additional imaging to be used for navigation with additional radiation dosage11). It also adds cost to the procedure of neuronavigation and to the use of a navigation stylet. As a practice matter, average 40% of total sum of money was charged to operation fee at our institution with EM navigation shunts. But, revision surgery needs more cost added on the first surgery11). Hayhurst et al.11) measured that cost of a shunt revision was ten times greater than the cost of a using navigation in their own country. Furthermore, the time span between revisions shortens progressively after second revision, indicating that economical disadvantages can be replicated14). Therefore, the cost-benefit ratio must be carefully established to obviate its need.
CONCLUSION
Mechanical malfunction and infection are the most significant problems associated with shunts for the treatment of hydrocephalus. Above all, a significant proportion of shunt failures were due to obstruction of the ventricular catheter, and accurate placement of the shunt catheter is highly important to reduce the incidence of shunt malfunction.
In conclusion, the use of EM navigated system in routine shunt surgery can eliminate poor shunt placement resulting in a dramatic reduction in shunt revision rates.


 XML Download
XML Download