

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The CSF leakage, which is related with dural injury during spinal surgery, is one of the commonly encountering neurological complications of spinal surgery. Remote cerebellar hemorrhage caused by this, however, is one of the least common complications, reported just as a case report4,12,13,15). Remote hemorrhage after craniotomy is reported to happen at a rate of 0.2-4.9%. On the other hand, there is no exact statistics on remote cerebellar hemorrhage related with spinal surgery9,13). In our hospital, we experienced an unusual case about remote cerebellar hemorrhage after intradural disk herniation surgery on L1-2 level, which we would like to present a paper about. Intradural disk herniation is a rare lumbar lesion, which is reported to happen at a rate of 0.26-0.30% of total herniated disc lesion, and no remote cerebellar hemorrhage after this surgery has been reported yet1,5,7,8,10).
CASE REPORT
A 66-year-old male patient complained severe back pain and radiating pain to both leg for several days. Spinal MRI demonstrated a huge intradural mass compressing conus medullaris and cauda equina at the L1-2 level, with slight ring enhancement on the surroundings (Fig. 1A, C). He was very healthy previously and did not have any risk factor for stroke.
A laminotomy on the appropriate level was done and dura was opened vertically. On the ventral side, there was a large dural opening and through the defect a large intradural disc material was extruded. The ruptured disc was removed totally with microsurgical piecmeal technique. In order to minimize post operative CSF leakage ventral defect and dorsal dural opening was closed watertightly. Fibrin sealant was covered on the sutured area and lamina was replaced with miniplate fixation. On postoperative MRI, it was removed successfully (Fig. 1B, D).
On the day after surgery, blood mixed with CSF came through the drainage bag, and the patient was instructed to take a rest in lying position. After operation his back pain was minimized and radicular pain was disappeared and the patient frequently took a sitting position against medical advice and about 300 cc of CSF was drained just within 4 hours.
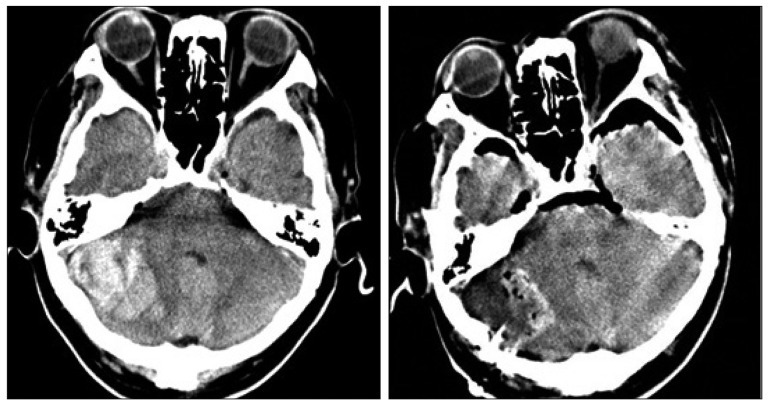
Two days after the surgery, the patient complained unexpected headache, dizziness, nausea and vomiting, while neurological condition was stable, pupillary reflex on both eyes were normal as well as limb motor power, but horizontal nystagmus was detected on both eyes. From the urgently conducted brain CT, it was reported that the patient had cerebellar hemorrhage with size of 3×3 cm on the right cerebellum and 1.5×1 cm on the left cerebellum. While brain stem was not compressed, fourth ventricle was distorted and headache was aggravated, leaving the decision to surgery (Fig. 2A). Suboccipital craniotomy and hematoma evacuation was performed, and hemorrhagic lesion on the right cerebellum was effectively removed (Fig. 2B). After craniotomy, the patient showed clinical improvement. He was able to leave the hospital after two weeks of initial operation without any neurological deficit.
DISCUSSION
Since Chadduck made it announced for the first time, remote cerebellar hemorrhage related with spinal surgery does not show distinct statistics and is only presented as case reports4).
While considering that the CSF leakage related with dural tearing during spinal surgery is one of the most common complications with the rate of 0.1-5.9%, the proportion of remote cerebellar hemorrhage related with this is relatively very low3,9).
Exact cause has not been found of remote cerebellar hemorrhage. In every case of remote cerebellar hemorrhage after spinal surgery, however, it has been found that there was the CSF leakage from dural damage during the surgery. In this condition, venous sagging is caused from the CSF pressure gradient between occipital and spinal cerebrospinal fluid, which generates stretching in cephalad, bridging cerebellar vein. With these in progress, hemorrhagic venous infarction is formed, which is known to generate hemorrhage1,3,5,6,9,11,13,15,16).
Papers published so far show that the type of spinal surgery, posture during the surgery, age or sex is not associated with its occurrence. It has been reported that remote cerebellar hemorrhage occurs in patients who had had preoperative hypertension, blood clotting disorder, aneurysm and cerebral arteriovenous malformation1-3,9,11).
Headache is the most common symptom. Patients, who had CSF leakage from dural injury during the spinal surgery, need to check neurological and clinical conditions carefully. When concurrent neurological abnormality - not influenced by spinal surgery - have occurred accompanied with headache, brain CT or MRI needs to be performed immediately, in order to check the presence of brain lesion5,11,13).
The treatments usually show good result in symptomatic approach. In emergency craniotomy and hematoma evacuation, no difference has been found in treatment between remote cerebellar hemorrhage and spontaneous one, when radiological brain stem compression or moderate distortion of fourth ventricle or clinical deterioration is observed5,11,13,16). The reported cases show that symptomatic approach and surgical approach produce good results with no long-term neurological sequelae and the prognosis is satisfactory5,13,14).
Spinal intradural disc herniation itself is extremely rare, and cerebellar hemorrhage from it is even less likely to occur5,7,8,10). As in the case of our patient, there has been no report on remote cerebellar hemorrhage from intradural lumbar disc surgery.
In our patient, histological confirmed disc materials that compressing dural sac and nerve roots were removed completely and defect of duramater was completely sealed and strengthened with glue. Although CSF leakage was not found during the surgery, some were found to be flowing into the drainage bag from the following day, which shows that remote cerebellar hemorrhage was considered to be caused from CSF leakage on the site of surgery. In case of CSF leakage after operation, to reduce sagging pressure to the cerebellar veins which is critical in the formation of remote cerebellar hemorrhage, avoidance of sitting position or ambulation, minimal and slow drainage of CSF will be helpful.
CONCLUSION
Not uncommonly occurring from spinal surgery, dural damage can be accompanied with CSF leakage. Excessive leakage of the CSF during or after the surgery can cause complications like nerve root herniation, brain stem herniation, cerebellar functional abnormality, cerebellar hemorrhage and cerebellar infarction9,11,13,16).
To reduce remote cerebellar hemorrhage, the patient should be instructed to take bed rest and restrict ambulation if CSF leaks after operation. When these conditions are found or suspected, immediate diagnosis and treatment, including surgery, is essential.

 XML Download
XML Download