

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Golf is a popular sport. Like other sporting activities, it can cause various types of injury to the musculoskeletal system. Golf does not involve physical contact between players. However, reports of golf swing-related fractures include stress fracture of the ribs, ulnar diaphysis, vertebral body, sternum, and hook of hamate2,6,9,15,17). To our knowledge, only one case of multiple spinous process fractures of the upper thoracic spine in a beginning golfer has been reported14). We report a case of multiple cervical spinous process fractures in a novice golf player and discuss its pathomechanism.
Go to : 
CASE REPORT
A 45-year-old female presented with intractable posterior neck pain that had lasted for 11 days. The severity of the pain had prevented sleep and rotation of the neck for 7 days. The patient had experienced a sharp and sudden pain on the posterior neck during a golf swing. The pain began when the club contacted the ground instead of the golf ball. Under the impression of acute sprain, the patient was treated conservatively at the local hospital. But, the symptom was aggravated despite receiving massage and physical therapy. There was no notable history of medical illness, such as diabetes, hypertension and osteoporosis. On physical examination, the patient complained of severe tenderness over the lower mid-cervical area and, in particular, limited range of motion during flexion and extension. However, swelling and ecchymosis were not evident at the tender point. The findings of neurological symptoms and signs were normal. Dynamic cervical radiographic findings were fractures in the spinous processes of C6 and C7 vertebrae without instability (Fig. 1). The patient underwent cervical magnetic resonance imaging (MRI) with a suspicion of other occult trauma around C6 and C7. Sagittal T1 and T2-weighted images (Fig. 2A, B) also showed spinous process fractures in C6 and C7. There was no abnormalitiy in the spinal cord. Fat saturation image (Fig. 2C) revealed high signal areas in interspinous and supraspinous ligaments between the C6 and C7 vertebra suggestive of an acute injury to cervical spine. Under the diagnosis of stable C6 and C7 spinous process fractures, the patient was prescribed with pain medications and wearing a cervical collar was recommended for 6 weeks. After cervical bracing and medication, pain gradually improved.
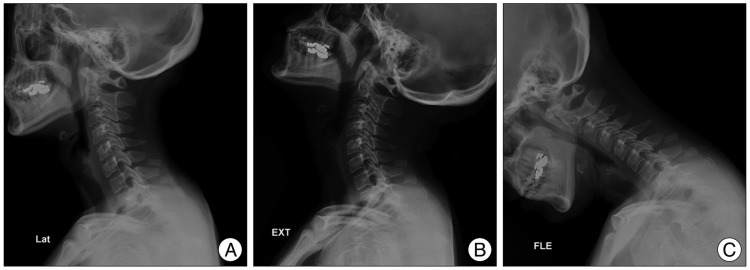 | Fig. 1Lateral radiographs showing C6 and C7 spinous process fractures (A) and no instability on lateral extension (B) and flexion (C) radiographs.
|
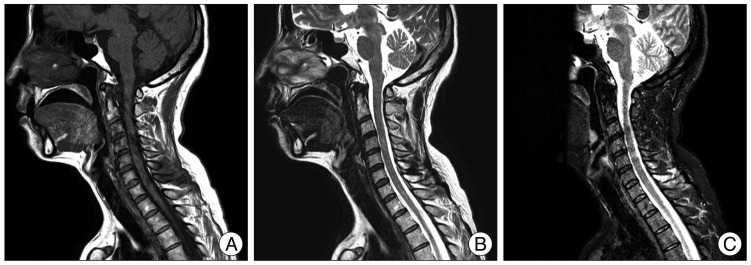 | Fig. 2Sagittal T1, T2-weighted magnetic resonance images (A and B) showing C6 and C7 spinous process fracture without spinal cord pathology. Fat saturation image (C) revealing high signal areas in interspinous and supraspinous between the C6 and C7 vertebra suggestive of an acute injury to cervical spine.
|
Go to :
DISCUSSION
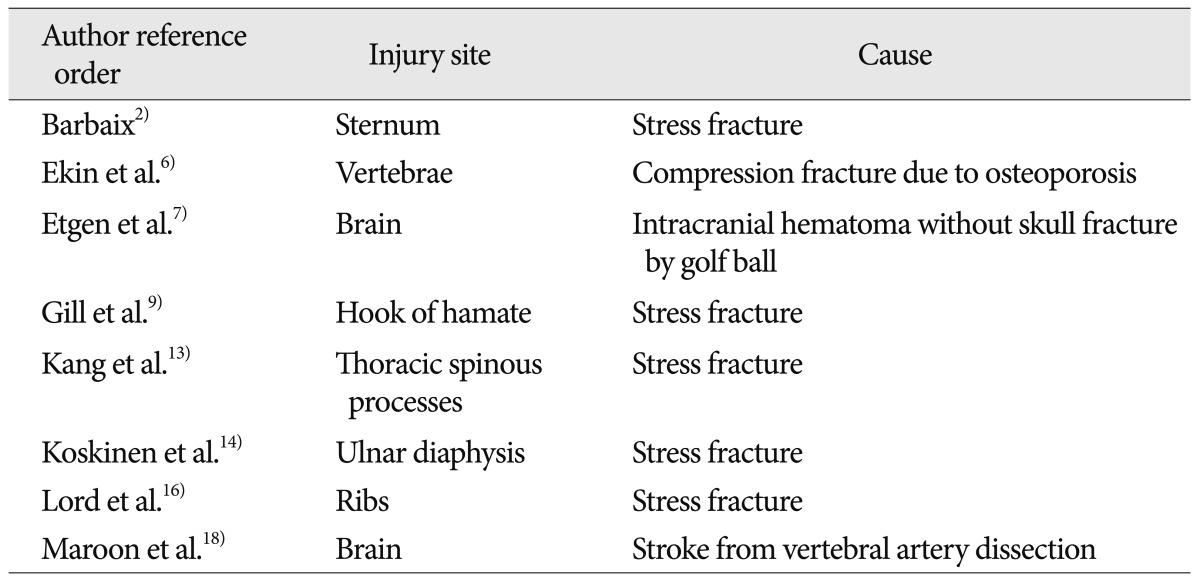
Golf is a global sport. It requires a coordinated sequence of whole body muscle activity to efficiently transfer the power generated by the swing19). During the each phase of a golf swing, there is a potential for injury. There have been a number of reports of golf related injuries (Table 1)2,6,7,9,14,15,17,18). But, only one report has described multiple spinous process fractures of the upper thoracic spine caused by golf swing itself14). The case included acute and delayed stress fractures. Initial MRI revealed a spinous process fracture of first thoracic vertebra. But, the follow-up MRI revealed the additional fracture in the spinous process of the second thoracic vertebra. The pathomechanism of this type injury remained ill-defined and was presumed to be similar to Clay-shoveler's fracture10). Avulsion of spinous process or Clay-shoveler's fracture was first described in Australia10). It is most prevalent among those engaged in hard physical labor10). More recently, it has also been described during Nintendo Wii activity4), volleyball13), car accident1), power lifting12), and golf14). It occurs when the head and upper cervical segments are forced into flexion against the opposing action of the interspinous and supraspinous ligaments11). The injury takes its' name from the fact that, during the throwing phase of shoveling, clay may stick to the shovel and jerk the trapezius and other muscles attached to lower cervical or upper thoracic spinous processes10). It can also occur with a whiplash injury, injuries that jerk the arms upwards, neck hyperflexion, or a direct blow to the spinous processes10). In our case, the trapezius muscle also contributed to the injury. The trapezius muscle originates from the medial one-third of the superior nuchal line and the external occipital protuberance of the occipital bone, from the spines of the seventh cervical and all thoracic verbetrae, and from the intervening supraspinal ligament20). It assists in suspending the shoulder girdle with other muscles. It is relatively flat and thin, but its thickness increases in the lower cervical and upper thoracic region20). Where its increased thickness is matched by a distinct diamond-shaped accumulation of tendinous fibers of origin20)(Fig. 3A). The spinous process is relatively longer in the lower cervical than the upper cervical area. Its fibers converge toward the bones of the shoulder20). During the back swing, the right upper and middle trapezius muscle contracts19)(Fig. 3B, C). During the forward swing, the left middle trapezius muscle contracts19)(Fig. 3D). So we can postulate that muscular contraction moves from right side to left side, like a bow. Because of the pectoralis muscle, the force may be amplified during the acceleration phase (Fig. 3E). When a right-handed golfer swings so the club contacts the ground prior to the ball, the energy accumulated during the back swing cannot be transmitted to the ball (Fig. 3F). There is a sudden change of muscle contraction from the right upper and middle trapezius to its attachment point (the spinous process). If enough force is transmitted through the trapezius tendon, spinous process fracture is possible. When the force is not strong enough to make fracture, if applied repeatedly, overuse or stress-type fracture may occur. This fracture is stable, and by itself is of little significance. But, it is painful. The present patient was initially misdiagnosed as having an acute cervical sprain. Atypically, this fracture may extend to the lamina, thereby involving the spinal canal with the potential of spinal cord injury11).
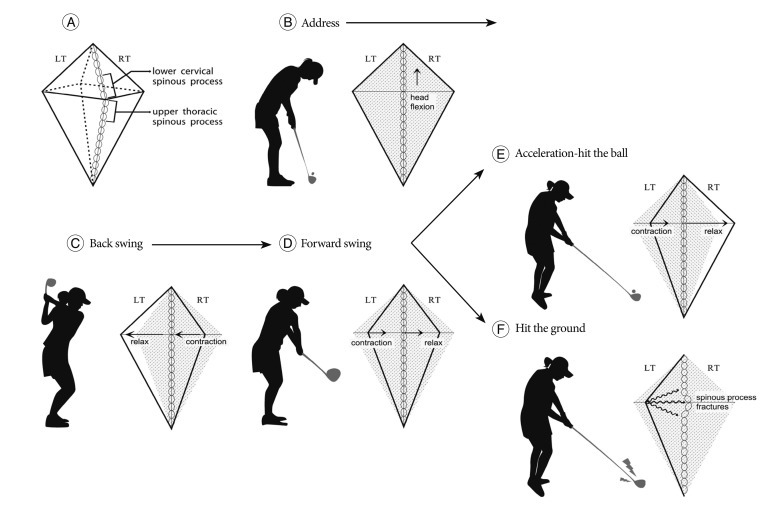 | Fig. 3Schematic draws of trapezius muscle during each swing phase. Trapezius muscle thickness is increased in the lower cervical and upper thoracic region (A). During back swing, right upper and middle trapezius muscle contract from address-neutral state (B and C). During forward swing, the left middle trapezius muscle contracts (D). The force may amplify during the acceleration phase (E). When a right-handed golfer swings such that the club contacts the ground before the ball back swing arc energy cannot be transmitted to the ball (F).
|
If a patient complains of long lasting neck pain, the attending clinician should have further study (cervical spine radiographs, computed tomography scan or cervical MRI) to rule out other occult fractures or injuries16). Midline tenderness may be the clue for the presence of fracture. If the lower cervical spine and/or cervico-thoracic junction are not well visualized on cervical spine lateral radiographs, a swimmer's view5) or CT scan15) should be obtained. An understanding of correct swing technique will help the golf beginner3). Golf related injuries increase without warm-up exercise8). So, warming up and stretching exercise before golf will reduce the risk of golf related injury8).
Go to :
 XML Download
XML Download