

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary bone lymphoma is an uncommon tumor that accounts for approximately 4-5% of extra-nodal lymphomas and less than 1% of all non-Hodgkin's lymphomas9). Furthermore, primary vertebral locations account for only 1.7% of all primary bone lymphomas, and the vast majority occur in short bones, with a predilection for the scapula, ileum, femur, and tibia11). Lymphoblastic lymphoma is a rare type of non-Hodgkin's lymphoma, and is the result of abnormality in adaptive immune cells, typically T-cells. To the best of our knowledge, this is the first report of solitary lymphoblastic lymphoma involving only thoracic spine. Here, we report a unique case of solitary lymphoblastic lymphoma of the B-cell precursor type involving only the thoracic spine. Surgical decompression and stabilization were essential to preserve function and maintain quality of life. We present a successful and requisite strategy for the management of this unique clinical presentation.
CASE REPORT
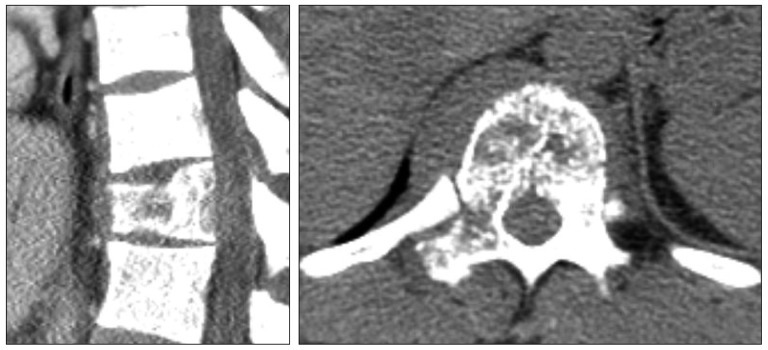
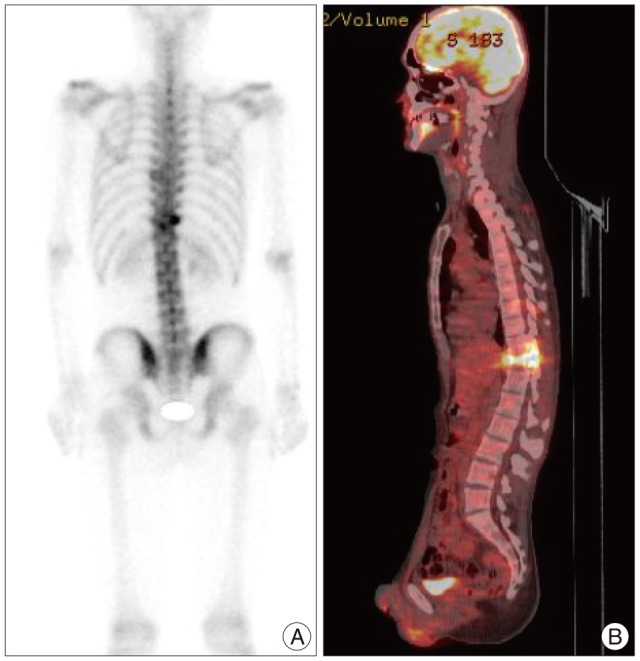
A 27-year-old man had progressively worsening back pain for 2 months. He had a history of mild back pain over the previous 2 years but the back pain had progressively worsened without any traumatic episode. The back pain worsened with activity, and he achieved relief by lying down. He also complained of night sweats and progressive weight loss of more than 10 kg over 4 months. A physical examination revealed no paresthesia or muscle weakness of the legs, no bowel or bladder symptoms, and the patient was able to straighten and raise his legs. Blood tests including erythrocyte sedimentation rate and C-reactive protein were within normal range. A computed tomography (CT) scan of the thoracolumbar spine showed lytic destruction in the body and right pedicle of T11. However, canal compromise by bony fragment was not detected (Fig. 1). Magnetic resonance imaging of the spine showed abnormally high signal changes in the T11 vertebral body and right pedicle with spinal cord compression by soft tissue extension (Fig. 2). Under a preliminary diagnosis of a primary bone tumor or metastasis, radionuclide bone scintigraphy (99m TC MDP) and positron emission tomography (PET)-CT were performed, but failed to depict an extraspinal lesion (Fig. 3). Cerebrospinal fluid examination revealed no abnormality. The patient then proceeded to surgery. Posterior decompression and fixation with instrumentation were performed. Histological specimen analysis findings were consistent with an aggressive lymphoblastic lymphoma of premature B-cell origin (Fig. 4). The tumor was CD10+ and CD99+ but negative for other markers. Postoperatively, marked pain relief was achieved and early mobilization while wearing a thoracolumbosacral orthosis was encouraged. The patient was transferred to our hematology and medical oncology department for chemo- and radiotherapy. He was performed 4 cycles of chemotherapy using Hyper CAVD regimen, followed by radiotherapy. At one year after surgery, he was pain free and able to return to full time work.
DISCUSSION
Lymphoma is a cancer of the lymphocytes, a type of sell that forms part of the immune system. Typically, it presents as a solid tumor of lymphoid cells. It can also affect other organs in which case it is referred to as extranodal lymphoma. The latest classification by the WHO (2008) lists 70 different forms of lymphoma divided in four broad groups3,5,14). The term lymphoma is used when the process is confined to a mass lesion with no or minimal evidence of peripheral blood and BM involvement3). Primary bone involvement at time of presentation is uncommon in non-Hodgkin lymphoma. The accepted definition of primary bone lymphoma is bone involvement without evidence of systemic involvement6). This form of non-Hodgkin's lymphoma is especially rare, and accounts for only 1% of all cases, and of these, primary vertebral locations account for just 1.7% of primary bone lymphomas4). Our patient presented with spinal compression from an osseous lesion consistent with an origin at the T11 vertebral body. No other origin of disseminated or extraspinal disease was observed by PET-CT or radionuclide bone scintigraphy. Primary bone lymphoma is often characterized by osteolytic defects, but these may be overlooked on plain radiographs. Due to its rarity, the true diagnosis is only established by histopathologic examination, and it is an essential to obtain tissue cores for histopathologic examination. Local pain and Type B symptoms, such as, generalized fatigue, night sweats, and weight loss are common1). When lymphoma involves the spine, it is more commonly found to be isolated in the epidural space due to secondary spread. Small case series of lymphoma with a spinal epidural origin have been reported, but these were primarily thoracolumbar in location and thought to result from an epidural, rather than a bony origin7,8). It is believed that primary epidural lymphomas may derive from normal lymphoid tissue in the epidural space12). Regardless of the spinal level or site of origin, patients with spinal lymphoma are at risk of neurological deterioration. The clinical manifestations of a compressive spinal mass may be pain, motor weakness, sensory deficits, and potential bowel or bladder dysfunction, and if left untreated, these may progress to paralysis. The treatment of these lesions is often multifactorial, and includes surgery, radiotherapy, and chemotherapy. Primary lymphoma of bone usually responds well to a combination of radio- and chemotherapy regimens, and an overall response rate of 94% and a 5-year survival rate better than that achieved by most other primary osseous malignancies have been reported2). Peng et al.10) also reported that combined chemotherapy and radiotherapy is the ideal treatment for primary non-Hodgkin's lymphoma of the spine, where as the survival is not influenced by the surgical or non-surgical treatment. In cases of severe pain or neurological deficits, however, early surgical decompression and stabilization is mandatory13). It is important that combined chemotherapy and radiotherapy followed by surgical decompression depending on individual priorities in the indications for operation on primary lymphoblastic lymphoma of spine with neurologic compression.


 XML Download
XML Download