

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Laminectomy is the most common procedure for the removal of spinal cord tumors1,3). Especially, central portion intramedullary tumor and large intradural extramedullary tumor often requires a total laminectomy for the midline myelotomy, sufficient decompression, and adequate visualization. However, the conventional total laminectomy causes muscle atrophy, postoperative kyphosis, postoperative neck discomfort, and a large skin incision4,9,13). Two less invasive techniques are available for total laminectomy, the split-spinous and tubular retractor techniques. The spinous process-splitting laminoplasty was first described in 1982, and since then, the modifications to the technique have been developed5,6,11,13). The major advantage of the split-spinous procedure is that it preserves the attachment of the paraspinalis muscles, which can decrease the postoperative muscle atrophy and discomfort6,11,13). The tubular retractor system, first described in 1997, is widely used as a minimally invasive technique2), and the use of a quadrant tube retractor allows for an extensive visualization with a small skin incision. Due to the differing advantages of the two techniques, we combined them for the removal of intradural spinal cord tumors. Here, we report the combined application of the two techniques.
MATERIALS AND METHODS
Patients and evaluation
A total of 19 patients with intradural cervical spinal tumor were enrolled in the study from January 2004 to April 2009. The mean sagittal tumor size was 11.4 mm (8-14 mm), and each tumor required either a one-level laminectomy or an adjacent partial laminectomy. We performed a total laminectomy considering the tumor size, location, edema and invasiveness. One surgeon performed all of the surgeries.
Between December 2006 and April 2009, a combined split-spinous laminectomy and quadrant tube retractor system procedure (Fig. 1) was used in 8 patients (Group 1). Between January 2004 and November 2007, the conventional total laminectomy technique was used in 11 patients (Group 2).
Preoperative and postoperative evaluations consisted of pathological findings, surgical parameters, radiological findings, and functional examination. Functional examination included a simplified version of the McCormick scale classification1) : Grade I (neurologically, mild focal deficit not significantly affecting the function of the involved limb, normal gait); Grade II (sensorimotor deficit affecting the function of the involved limb, mild-to-moderate gait difficulty, patient can walk independently); and Grade III (severe deficit, patient requires a wheelchair or other assistive devices, and cannot walk independently).
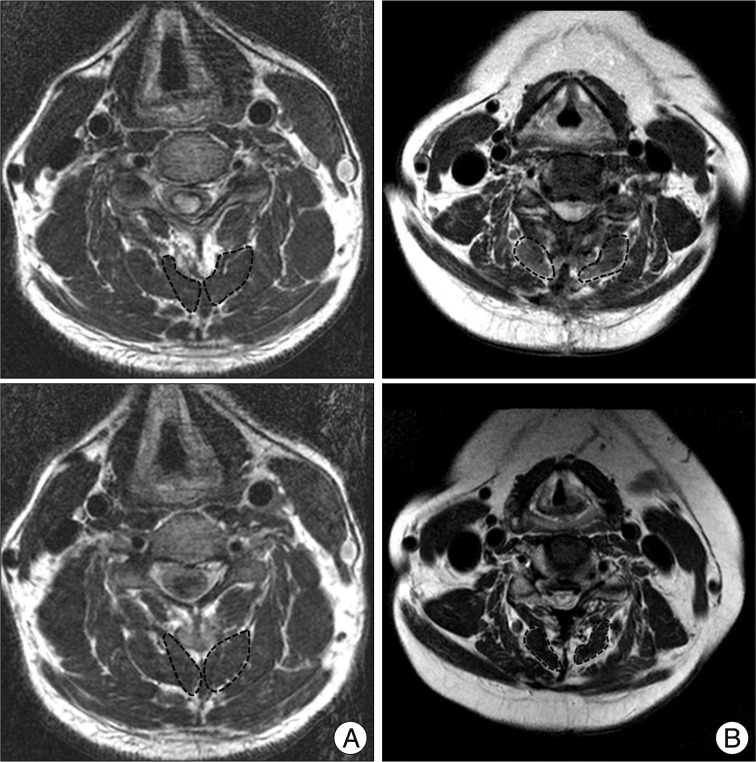
All patients were evaluated for preoperative spinous process shape and postoperative bone fusion, using a computed tomography (CT) at preoperative day one and again at one month and two years postoperatively. All patients underwent preoperative magnetic resonance imaging (MRI) and yearly postoperative follow-up MRI examinations. For a quantitative analysis of the posterior muscle damages, muscle atrophy was calculated by comparing the cross-sectional areas of the deep extensor muscles in each of the pre- and two-year postoperative T2-weighted axial MRIs, at the affected level in all 19 patients (Fig. 2). The rate of muscle atrophy was calculated, using the Shiraishi method11).
Surgical technique
Conventional total laminectomy
All patients were placed in the prone position for a cervical posterior approach. A radiolucent three pin-head fixed instrument was used. A vertical midline incision was made after determining the correct level under the guidance of fluoroscopy. The skin, fascia and nuchal ligament were incised and the muscle was dissected. Total laminectomy and tumor removal were performed. After successful tumor removal, the fascia and muscle were re-approximated.
Combined split-spinous laminectomy and quadrant tube retractor system
Position and exposure
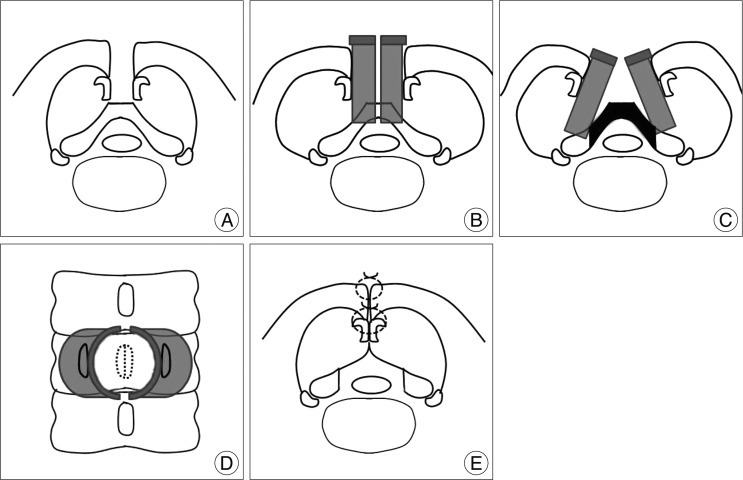
Patient positioning and equipment were the same as in the conventional total laminectomy. The skin, fascia and nuchal ligament were incised. The tip of the spinous process was exposed, and then it was split using a high speed drill with a fine 1-mm bullet shaped burr, without any injury to the attachments of the semispinalis cervicalis and multifidus muscle, bilaterally. The depth of the spinous process was evaluated by preoperative CT image. We divided the three-fourths of spinous process. To expose the target lamina, the remnant portion of the spinous process was fractured, and the muscles were dissected from the central portion of the lamina to the medial margin of the facet joint. Care must be taken for the preservation of facet capsule. Quadrant tube retractors were placed on both lamina with a slight opening, and were widened for the maximal viewing. This technique is illustrated in Fig. 1A-D.
Laminectomy and tumor removal
Total laminectomy and tumor removal were performed. These procedures are similar to the conventional laminectomy. During the procedure, the release of quadrant retractor was mandatory at 30-minute intervals. Quadrant retractor system might overweigh the paraspinal muscles, comparing to the conventional retractor.
Closure
After successful tumor removal, we performed meticulous dural closure in the quadrant tube retractors. We then checked the CSF leakage by Valsalva maneuver and the dural closure covered by Durseal® or Tissel®. The each half of the split spinous process was re-approximated. We made a small hole of the splitted spinous process and we approximated them through the holes. This technique is illustrated in Fig. 1E.
RESULTS
Clinical parameters
Patient characteristics are shown in Table 1. The mean follow-up period was 34.8 months in Group 1 (range, 24-51 months) and 64.1 months in Group 2 (range, 38-83 months). The tumor resection success and postoperative prognosis depended on the tumor characteristics. Two patients with astrocytoma were treated with a total laminectomy for surgical decompression and midline small biopsy, but showed a postoperative progression of motor weakness and an increase in the tumor size at the 12- and 24-month MRIs. We did not perform a statistical analysis of the postoperative functional outcomes, tumor resection and recurrences, because these variables depended on the tumor characteristics.
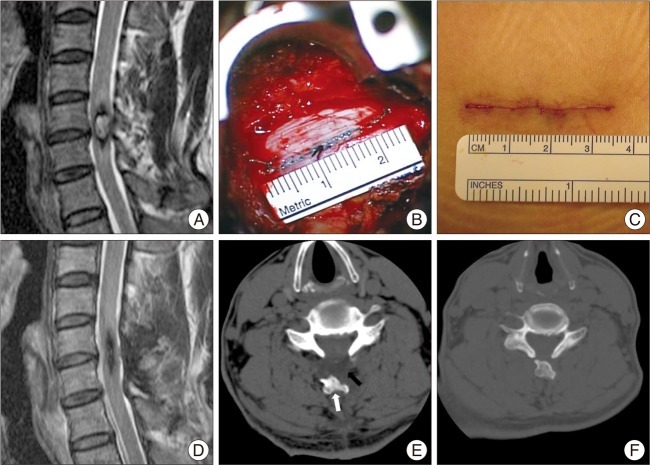
The different clinical parameters by the approach techniques were compared (Table 2). The quadrant tube retractors provided a wide surgical field with a small skin incision. A 54-year-old patient presented with a six-month history of progressive quadriparesis (Fig. 3). MRI scans revealed an intradural intramedullary lesion at the C5-6 level. The patient underwent a surgical resection with the combined technique, which provided excellent visualization and allowed for a midline myelotomy and easy dural closure. A final follow-up MRI showed complete resection with no recurrence. The two-year postoperative CT showed a resolved fluid collection and proper location of the spinous process, with complete bony fusion. In this case, the skin incision scar was 3.4 cm. This particular case illustrates the various advantages of the combined technique. As shown in Table 2, skin incision size and blood loss were significantly smaller in Group 1, compared to those of Group 2 (p<0.05).
DISCUSSION
Laminectomy is the most common procedure for the removal of spinal cord tumors1,3,12). Traditional surgical resection involves a posterior midline approach and the stripping of muscles and ligaments from the underlying lamina and spinous process. However, the conventional laminectomy procedure, intraoperatively, damages the posterior supporting structures, which can require a wide skin incision, and can lead to irreversible atrophy of the paraspinalis muscles and postoperative kyphosis4,9,13).
In 2006, Tredway et al.12) reported a minimally invasive resection of a cervical schwannoma, using a quadrant tube retractor system and hemilaminectomy. Although hemilaminectomy is a less invasive and an effective procedure, it has not enough surgical view to achieve sufficient surgical decompression and midline myelotomy to remove a intramedullary cord tumor or central located large intradural extramedullary tumor7,9,10,12). Therefore, we used a technique that combined split-spinous laminectomy with a quadrant tube retractor system. Split-spinous laminectomy can preserve the paraspinalis muscles and allow for the performance of a total laminectomy with a midline myelotomy, sufficient surgical decompression, and a meticulous dural closure6,11,13). A quadrant tube retractor with a 26 mm outer diameter is expandable to approximately 40 mm, with easy control of the surgical angle, using the fixable arm assembly, which provides a good visualization even with the small skin incision. Thus, these two surgical techniques have a synergistic effect, in minimizing the invasiveness of the removal of an intradural cord tumor. As shown in the results of this study, the skin incision size and blood loss were significantly smaller in Group 1, compared to those of Group 2. Also, the two-year postoperative muscle atrophy rates were significantly lower in Group 1. Paraspinalis muscle acts as a dynamic stabilizer of the cervical spine, and they are injured by a conventional posterior surgery8). This split-spinous technique allowed for far less injury of the muscle attachment on spinous process, resulting in reduced postoperative atrophy of the muscles. However, the preserved spinous process was off the lamina in our procedure, so we could not be sure of the function of the spinous process or paraspinal muscle. But, we used the combined technique when only two or fewer cervical levels were involved. The deep extensor muscles were involved more than two levels in the cervical spine. Therefore, we could expect a positive function of the preserved paraspinal muscles.
There are some tips of our procedures. First, the quadrant tube retractor has a limited longitudinal surgical field. As such, it must be repositioned by one or two levels if it is to be used on a lesion covering the three or more cervical levels. In these cases repositioning of the retractor would require an additional skin incision and muscle dissection, decreasing the advantage of the tubular retractor. Therefore, we recommend the quadrant tube retractor in cervical lesions covering the two or fewer spinal levels. Second, this procedure is suitable for an intramedullary cord tumor, requiring the midline myelotomy or central located large intradural extramedullary tumor, needing the sufficient decompression. In other cases, hemilaminectomy could be advantageous. Third, the tip of the procedure was the release of quadrant retractors during the operation. Quadrant retractor system should decrease the skin incision, but it might overweigh the paraspinal muscles, comparing to the conventional retractor. Therefore, we released the retractor for 2-3 minuites at 30-minute intervals.
There are some limitations to the present study. First, this study analyzed a small series of consecutive patients with different tumor pathologies. As such, the postoperative prognoses varied, according to the specific tumor characteristics. These differences might influence the postoperative progress, postoperative medication and muscle atrophy. Second, the periods of the study differed, based on the surgical technique. Between December 2006 and April 2009, a combined split-spinous laminectomy and quadrant tube retractor system was used, whereas, between January 2004 and November 2007, the conventional total laminectomy technique was used. Although, the surgical techniques were different, the difference in time of the surgery might have influenced the experience and ability of the surgeon. Lastly, our study did not include the biomechanical analysis. The paraspinal muscle could influence the cervical alignment, such as postoperative kyphosis, or dynamic motion, but we did not check these. Therefore, future studies with prospective, randomized controlled trials are needed to address these issues, such as the safety and efficacy of this technique, and whether less muscle atrophy has positive effect on a long-term clinical and functional outcome.
CONCLUSION
The combined spit-spinous laminectomy and quadrant tube retractor system technique allowed for a total laminectomy with minimal trauma to the surrounding tissue. We propose that this technique offers possible advantages over the traditional open tumor removal for the intradural spinal cord tumors that require a total laminectomy and that cover one or two cervical levels.


 XML Download
XML Download