

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital intracranial cysts are rare benign and developmental cysts that originated from aberration of the lining membranes3,6). Modern neuroimaging techniques have improved the diagnoses of intracranial cysts, as a result, increasing numbers of patients from all age groups with these cysts are being observed. Although some children with intracranial cysts may experience symptoms, many present with only mild unspecific symptoms such as headaches, learning deficits, or behavioral disturbances. Furthermore, in infants, increased head circumference is sometimes the only known indication.
In general, careful monitoring is used for asymptomatic cases. However, cysts in infants and in younger children can grow to a substantial size26,50). These observations suggest that treatment by surgical decompression may be necessary for asymptomatic patients26). Surgery is also necessary in cases where the cysts gradually enlarge, when local neurological symptoms or epileptic seizure are present, and when intracranial pressure is elevated by hydrocephalus or subdural hematoma.
It is a matter of debate whether these children should be subjected to surgeries, and if so, there are diverging views on which type of surgery should be performed. Some surgeons prefer to perform fenestrations through a craniotomy11,13,14,28,31,40,42), whereas others advocate a shunt insertion2,5,7,19,29,30,32) or fenestrations through an endoscopic procedure5,34). However, each of these methods has advantages and disadvantages. When craniotomy is performed to excise cysts, the complete removal of the cysts is difficult and the recurrence rate is approximately 25%. When cystoperitoneal shunting procedures are performed, there are many possible complications38). When endoscopic fenestrations are performed, it is difficult to control bleeding and copious amounts of irrigation are often required for a period of operations. The limited number of working and viewing channels is also a disadvantage of endoscopic procedures.
In the present study we retrospectively reviewed the 110 children who underwent surgeries for intracranial cysts. We analyzed and compared the clinical and neuroimaging outcomes according to treatment modalities that were used.
MATERIALS AND METHODS
Study design and data extraction
This was a retrospective study that included all children (age ≤18 years) that underwent surgeries for intracranial cysts between 1996 and 2011. Only patients that had verified benign developmental cysts were included. Surgical intervention was done in patients with symptomatic cysts, who demonstrated signs of increased intracranial pressure, hydrocephalus, or focal neurological signs, and those complicated by intracystic or subdural hemorrhage. Asymptomatic patients with intracranial cysts including sylvian arachnoid cyst also underwent surgical management if the cyst showed mass effects, such as midline brain shift, prominent bony protuberance, cyst was suspicious of tumorous condition, and if there was parent's strong wish to get rid of pathologic lesion in their children.
The following data were extracted from the medical records of the patients : demographic information; presenting symptoms; clinical findings; location and side of the cyst; surgical method that were used; postoperative changes in cyst sizes; postoperative changes in presenting complaints; and possible adverse effects of the operations identified by clinical or neuroimaging examinations, such as subdural hygromas, subdural hematomas, or new neurological symptoms or deficits.
All of the patients were subjected to preoperative computed tomography (CT) or magnetic resonance imaging (MRI) examinations and to postoperative CT examinations within 72 hours, and at 3, 6, and 12 months following surgeries. PetaVision software (Hyundai Information Technology and the Asan Medical Center, Seoul, Korea) was used to measure the cyst volumes in the pre- and postoperative CT and MRI scans. Patients that showed postoperative abnormalities (such as subdural hematomas or hygromas) were subjected to further follow up examinations until either spontaneous remissions or remissions after further surgical treatments were observed.
Surgical procedures
Endoscopic cyst fenestrations were the most commonly performed procedure, with 71 cases (64.5%), while craniotomies and cyst excisions (with or without fenestrations) were performed in 30 cases (27.3%). Cystoperitoneal shunting procedures were necessary for nine patients (8.2%). Of these nine patients, shunting alone was performed in four patients, and shunting combined with craniotomies was performed in five patients.
Clinical outcome scale (COS)20)
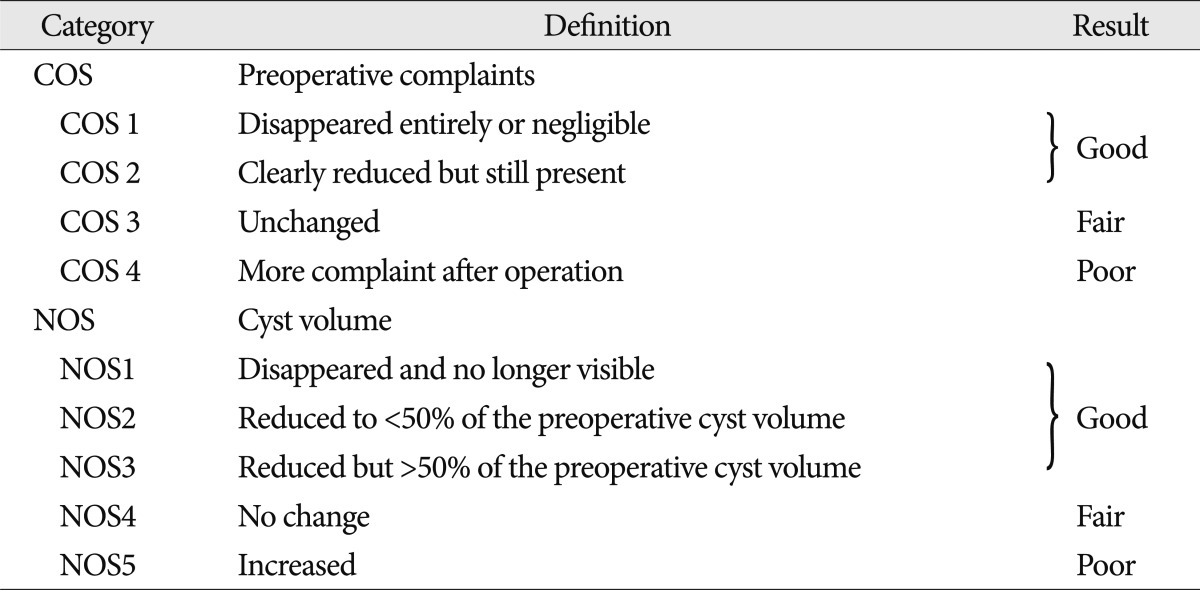
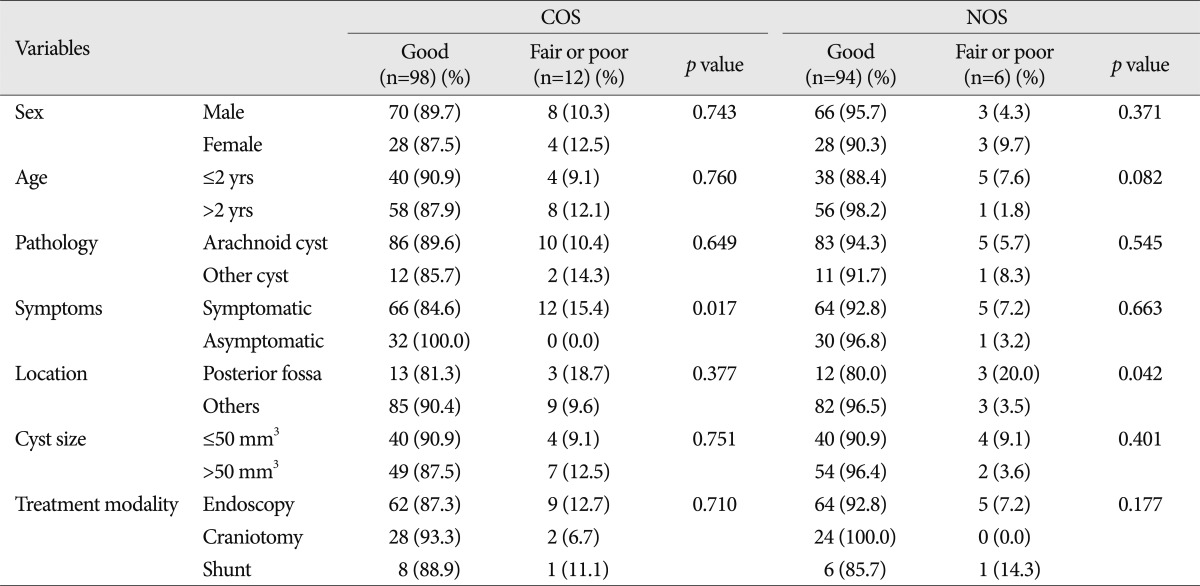
The clinical results were categorized into one of the following four COSs based on information from the medical reports of the last follow-up : in COS1, the preoperative complaints had disappeared entirely or were negligible; in COS2, the preoperative complaints were clearly reduced but were still present; in COS3, the preoperative complaints were unchanged; and in COS4, the complaints increased after the operation. COS1 or COS2 were defined as having good results, COS3 as fair, and COS4 as poor (Table 1).
Neuroimaging outcome scale (NOS)20)
The neuroimaging results of the decompression procedures were defined as being the changes in cyst volumes that were measured in the CT scans performed during the last follow-up examinations. These results were categorized into one of five possible NOSs : in NOS1, the cysts had disappeared and were no longer visible; in NOS2, fluid volumes that amounted to less than 50% of the preoperative cyst volumes were still visible at the cyst sites; in NOS3, fluid volumes were observed that were reduced but still greater than 50% of the preoperative cyst volumes; in NOS4, no changes in cyst volumes were observed; and in NOS5, the cysts had enlarged. Patients that were NOS1, NOS2, or NOS3 were defined as having good results, NOS4 as fair, and NOS5 as poor (Table 1).
Complications, recurrence and treatment failures
Complications were defined as additional pathological conditions caused by the treatment procedures. Recurrences were defined as increases of greater than 30% in smallest cyst sizes (based on MRI or CT scans) after the cyst sizes had been reduced. Treatment failures were defined as the treatments that had no effects (patients that were COS4 or NOS5).
RESULTS
Patient and radiologic characteristics
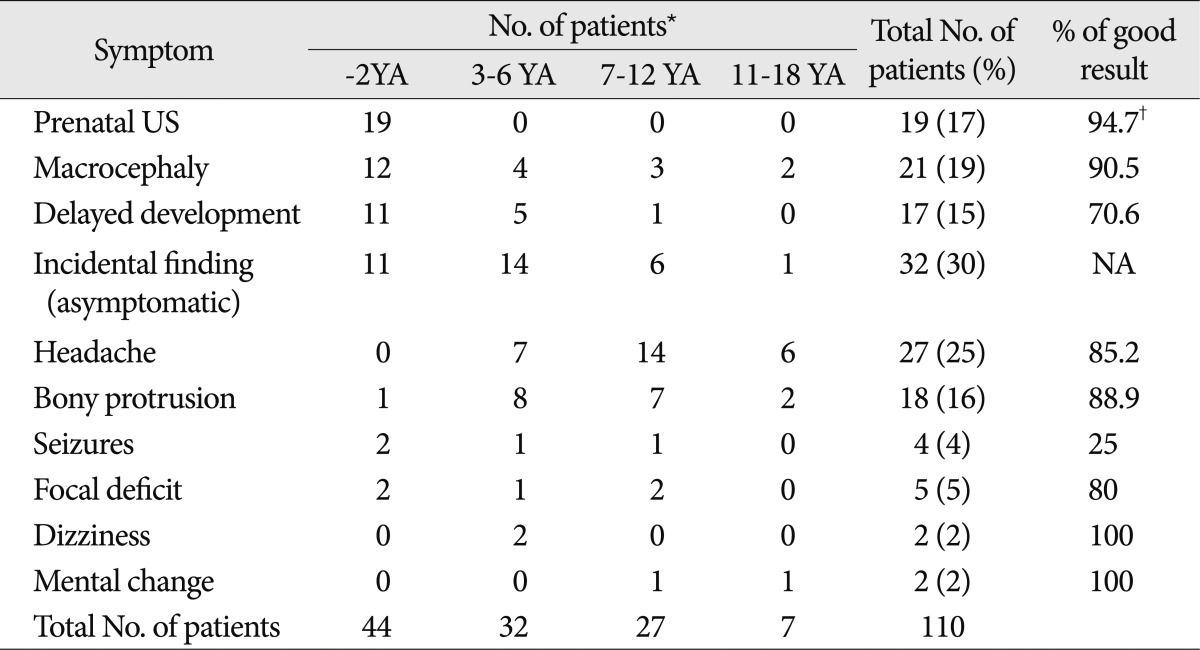
A total of 110 patients (78 boys and 32 girls) were included in the study (M : F=2.4 : 1). The mean age of the patients at the time of surgery was 4.8 years (with a range from 4 days to 17 years, and a median age of 3 years). The mean follow-up duration was 44 months (with a range of 3-161 months, median duration of 28 months). 44 patients were less than 2 years old; 32 patients were preschool age (2-6 years); 27 patients were prepubertal (7-12 years); and 7 patients were adolescents (13-18 years). The main preoperative complaints are summarized according to age in Table 2.
Eleven patients underwent surgeries because increased cyst sizes were observed during the follow up examinations. On the preoperative CT or MRI scans, obstructive hydrocephaly were observed in 18 patients, subdural hemorrhages in six patients, subdural hygromas in six patients, and brain compressions by cysts in 13 patients.
The majority of patients had cysts in the sylvian fissure (56 patients, 50.9%; 42 patients with cysts on the left side, 13 with cysts on the right, and one with bilateral cysts). Sixteen patients had cysts in the posterior fossa (14.5%). Twelve patients (10.9%) had cerebral convexity cysts, eight (7.2%) had suprasellar cysts, four had interhemispheric cysts, and three had quadrigeminal cysts. The remaining 11 patients had cysts in other locations. The mean size of the cysts was 86.5 cm3 (with a range of 4.7-470.1 cm3, and a median size of 54.8 cm3).
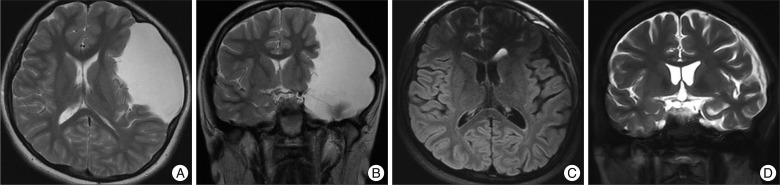
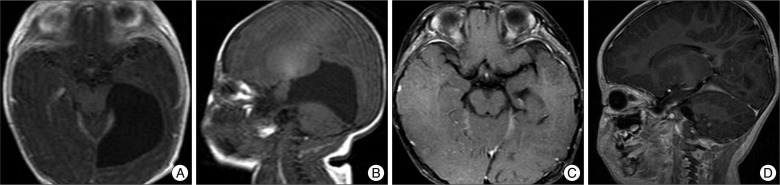
The most commonly observed intracranial cyst were arachnoid cysts (96 patients, 87.3%) (Fig. 1), followed by neuroglial cysts (six patients) (Fig. 2), endodermal cysts (three patients), porencephalic cysts (three patients), and choroid plexus cysts (two patients). Intracranial cysts other than arachnoid cysts are summarized in Table 3. All of the sylvian fissure cysts (n=56) were arachnoid cysts and the ratio of cyst locations (left relative to right sylvian fissures) was 42 : 13, indicating that left-side sylvian fissure cysts predominated.
Clinical outcomes
A total of 98 patients (89%) reported better functions after surgeries. Sixty-two (56%) were symptom-free in follow-up examinations (COS1). Thirty-six (33%) patients reported significant reductions in their preoperative symptoms (COS2), and 12 (11%) reported no change after operations (COS3). No patients reported worsening of their symptoms after surgeries. Of the 12 patients that reported no changes, developmental delay symptoms were present in five, headaches in four, intractable seizures in three, macrocephaly in two, bony protrusions in two, decreased visual acuity in one, and a psychiatric disorder in one. Both the pre- and post-operative neuroimaging scans were available for 11 of these 12 patients : comparison of these scans showed that after surgeries the cysts were reduced to less than 50% of the preoperative volumes (NOS2) in three patients, were reduced but still greater than 50% (NOS3) in five, were not changed (NOS4) in one, and were increased in size (NOS5) in two.
Asymptomatic cases were predictive of good outcomes (COS1 or COS2) (p=0.017). No other symptoms or signs, such as increased intracranial pressure, subdural hemorrhages, ages of the patients, cyst pathologies, cyst locations, or cyst sizes, were significantly associated with the clinical outcomes (Table 4). In addition, the operation methods that were used (endoscopic fenestrations, craniotomy and cyst excisions, or shunting procedures) were not significantly associated with the clinical outcomes (Table 4).
Neuroimaging outcomes
Neither the pre-, nor the postoperative scans were available for ten of the 110 patients. Therefore, these patients were not included in the neuroimaging analyses. In the remaining 100 patients, the cysts were no longer visible on the postoperative images (NOS1) in 8 patients, were reduced to less than 50% of the preoperative volumes (NOS2) in 43 patients, were reduced but still greater than 50% of the preoperative volume (NOS3) in another 43 patients, were not changed (NOS4) in two patients, and were enlarged (NOS5) in four patients. The pre- and post-operative cyst sizes were compared among three different surgical groups (Fig. 3). Statistically, there were no differences in neuroimaging outcomes on the basis of the ages of patients, pathologies, cyst sizes, or among the three different surgical techniques. However, posterior fossa cysts predicted unfavorable outcomes (NOS 4 or NOS5) (p=0.042) (Table 4).
Association between clinical and neuroimaging results
Both the clinical and neuroimaging outcomes could be assessed for 100 of the 110 patients. There were no strong associations between postoperative volumes and clinical outcomes (Spearman's correlation coefficient=0.111, p=0.270). However, after patients were dichotomized according to their good or poor clinical outcomes (COS1 and 2 compared with COS3 and 4), and according to neuroimaging outcomes (NOS1, 2 and 3 compared with NOS4 and 5), a significant association was observed between good clinical outcomes and good neuroimaging outcomes (p=0.017).
Complications
None of the complications that were encountered were severe, nor did they lead to any permanent sequelae. A total of 26 patients (24%) experienced complications, with ten (9%) requiring additional surgeries. The most common complications were postoperative subdural hygromas (n=18); however, in the majority of cases, these hygromas were asymptomatic and spontaneously resolved (n=15); in the remaining three patients, the primary procedure that was used was shunt insertion (cystoperitoneal in two, and subduroperitoneal in one). Patients that were treated with shunting operations seemed especially prone to complications. Postoperative subdural hematomas occurred more frequently following insertions of internal shunts (two of nine patients) than after endoscopic cyst fenestrations (2 of 71 patients). Furthermore, shunt infections occurred in two patients, and a shunt malfunction was observed in one patient.
One patient who underwent endoscopic cyst fenestration developed an oculomotor nerve palsy and presented with spontaneous remission after a few months.
Recurrences & treatment failures
Thirteen patients (11.8%) underwent additional surgeries due to recurrences or treatment failures. Of these patients, ten had undergone endoscopic fenestrations, two had undergone craniotomies and cyst excisions, and one had undergone a shunting procedure. The type of treatment did not influence the recurrence rate (p=0.662) or the failure rate (p=0.247). The reoperations that were necessary due to recurrences or treatment failures are summarized in Table 5.
DISCUSSION
Overall, the majority of patients that underwent operations for intracranial cysts had good clinical and neuroimaging outcomes. No severe or permanent complications related to the treatments were observed.
A great deal of debate exists about what is the best choice of treatment for asymptomatic patients with intracranial cysts12,20,21). Generally, conservative treatment approaches are recommended for adult patients with asymptomatic cysts, whereas some authors advise more aggressive approaches for asymptomatic pediatric patients. There is substantial evidence indicating that there are critical developmental phases in childhood during which specific abilities are learned. Deprivation of stimuli that are important for the brain development during these critical periods can cause permanent deficits4,9,18). In several studies, intracranial cysts have been shown to cause functional deficits, metabolic deficits, or deficits in the perfusion of blood to the underlying cerebral tissues10,22,39,42,44,49). Therefore, the presence of intracranial cysts during childhood may impair optimal brain development during critical developmental periods. Intracranial cysts in children may not only cause acute symptoms in some patients, but also affect the developing brain in more subtle ways, which can ultimately lead to learning difficulties and behavioral problems. The series presented in this study included asymptomatic newborns with giant intracranial cysts or progressively enlarging cysts. In our opinion, it is important to consider these possible impairments when deciding whether to perform surgical decompressions of intracranial cysts in children because early decompression in a child may help to relieve the pressure on the underlying cerebral tissues and thus allow more normal brain development.
Most authors agree about the indications for treatment of symptomatic cysts19,37,51). In general, the more evident a symptom is, the sharper the indication is, which is followed by more satisfactory results. Neurological focalities usually respond favorably to treatment28). All patients with focal deficits improved in the series that was presented here, independent of cyst locations. Increased intracranial pressure, hydrocephalus, and mass effect are other clear indications for treatment.
The indications for treatment are debated far more in cysts with headaches or epilepsy8,15,27,45,47,48). This series included a few cases of patients with headaches (without increased intracranial pressure), and the results of treatment in these patients were not satisfactory. Headache remain a controversial indication for cyst surgery47) and there is even skepticism about the effectiveness of cyst treatments48). Epilepsy is frequently associated with intracranial cysts15,25,33), but the seizure etiology remains unknown, and the coexistence of seizures and cysts may be incidental15,27,33,47). Thus, careful preoperative selections are mandatory.
The clinical improvements observed in our series seemed to parallel the postoperative reductions in cyst volumes, as the children who had the most pronounced volume reductions experienced better clinical improvements. Similar clinical correlations with neuroimaging have previously been described by other authors16,17,23,36). However, these results contrast with findings in adults that underwent surgeries to treat arachnoid cysts21). In these adults, clinical improvement seemed unrelated to the degrees of volume reductions. This difference between adults and children is likely due to the fact that many of the children underwent surgeries when their brains were still growing. Throughout childhood, the neurocranium is molded to fit the contents of the skull. Thus, intracranial cysts create surplus intracranial spaces by being present during skull growth. In adults, this extra volume may be too large for the relieved brain to fill even after successful cyst decompression. Therefore, in these situations, there would be residual fluid volumes. However, in children the growing brain may be able to fill in the vacant space left by the cyst. Therefore, surgical decompressions at early ages may prevent the mismatches between skull volumes and brain volumes that are often encountered after decompression in adults20).
The optimal treatment for arachnoid cysts in children has yet to be determined. The most common procedures are shunt placements and fenestrations of the cysts, but both procedures have drawbacks2,11,14). The shunt operation is a non-invasive, simple, and safe procedure compared to direct removal of cyst walls43). According to Punzo et al.38), shunt operations must be considered in the following cases : 1) when the non-communicative arachnoid cysts are accompanied by hydrocephalus and the basal cisterns are obstructed; 2) when neither mass effect nor hydrocephalus was confirmed on radiography; and 3) when long surgical times enhance the risks. However, the disadvantages of shunt operations are : 1) the arachnoid membranes are left to perform secretory and filtrating functions; 2) surgical vision is limited; and 3) there is a possibility of fatal slit ventricle syndrome due to infection, obstruction, or overdrainage of cerebrospinal fluid (CSF). Moreover, the postoperative outcomes are complicated by subdural hemorrhage and headache. For all of these reasons, shunt operations are now only performed in rare cases38,41).
Gradually, fenestrations have become the primary therapeutic option. In a large microsurgery series by Helland and Wester20,21), 82% of patients improved and 5% worsened; the rates of complications were 17% in adults and 6% in children; and additional surgeries were required in 7% of adults and 17% of children. Levy et al.28) reported a microsurgery series of 50 patients and concluded that microsurgery was better than endoscopy because it offered better control of hemostasis with bipolar forceps and other standard instruments. Nevertheless, the complication rates in this study were not negligible : 10% of the patients suffered from meningoceles, 6% had nerve palsies, 6% had CSF leaks, 4% had subdural hematomas, and 2% had wound infections.
In the last 20 years, the rapid development of modern neuroendoscopic techniques had offered a new option for cyst fenestration. There are some authors that consider the current endoscopic success rates to be worse than those obtained with microsurgeries1,28). However, there are also several articles reporting that endoscopic results are better than microsurgical results37,46). Nowoslawska et al.35) reported a series where microsurgeries and endoscopies were compared. This study found similar success rates with significantly shorter duration of hospitalization after endoscopies. Karabatsou et al.24) obtained clinical and radiological improvements in 92% and 63% of cases, respectively, when using endoscopic neurosurgeries. These results can be compared with the clinical and radiological improvements of 72% and 79% of cases, respectively, reported by Levy et al.28) after microsurgeries.
In our study, clinical and radiological improvements were reported in 87.3% and 92.8% of cases, respectively, after endoscopic neurosurgeries, in 93.3% and 100% after open microsurgeries, and in 88.9% and 85.7% after shunt operations (Table 4). There were no statistical differences in clinical outcomes (p=0.710) or volume reductions (p=0.177) when the different surgeries were compared. Endoscopic neurosurgeries are less invasive than microsurgeries, and are at least as effective as open surgeries. Thus, given the advantages and complications of these surgical techniques, we suggest that endoscopic fenestration should be the first treatment attempted in children with intracranial cysts.
In this study, there seems to be little differences in surgical outcomes among the type of pathologies. However, given the surgical outcomes depending on the kind of cysts or mechanism of cyst growth could be different, prospective and large-sized study grouped according to pathologies of cysts should be investigated.
CONCLUSION
Surgical decompressions of intracranial cysts in children yield good long-term outcomes for the majority of patients, with low risks of complications or additional impairments. Although there is no general consensus about which of the treatment modalities is appropriate for intracranial cysts, most authors agree that fenestrations of the cyst walls have advantages relative to shunting procedures. However, the same fenestrations that are obtained with open microsurgeries can also be obtained with closed endoscopies. Endoscopic neurosurgery is less invasive and less complicated than microsurgery or shunt operation and at least as effective as open surgery. Thus, given the advantages and complications of these surgical techniques, we suggest that endoscopic fenestration should be the first treatment attempted in children with intracranial cysts.



 XML Download
XML Download