

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hirsch6) reported successful results from his discectomy without intervertebral body fusion in 1960, and various approaches have been suggested by other authors7-9,16). However, complications were also reported related to the anterior surgery from the injury of vertebral artery, nerve root and spinal cord during the operation7,18,19). Although complication from vertebral artery damage is not common, it may result in serious conditions with ischemic neurologic damage5,7,16,17,19). Flynn4) reported 0.19% of nerve root damage in 82114 anterior cervical surgery cases.
The concern for possible complications may lead to insufficient nerve decompression being performed. In this regard, adequate anatomic knowledge of the cervical spine is essential for successful surgery without complications. Pait et al.14) and Oh et al.12) studied the spatial relationship between the uncinate process and vertebral artery in 1996, and Chang et al.2) published the anatomic measurement data required for an uneventful anterior microforaminotomy. However, more studies are required in this area, especially where it lacks of in Korea.
The purpose of this study is to elucidate the anatomic relationships among neurovascular structures around the uncinate process.
MATERIALS AND METHODS
Twenty-eight formalin-fixed cervical spines were removed from adult cadavers of nineteen men and nine women who ranging in age from 41 to 78 years. The anterior part of the cervical vertebral bodies and discs from C1 through C7 were exposed after removing the structures in front of them except for the longus colli muscle. Then, in the prone position, the spinal cord and nerve roots were exposed by laminectomy. The cervical vertebrae were then transected at the level of the disc spaces. Measurements made on the transverse sections were performed to understand the anatomical relationships of the various structures.
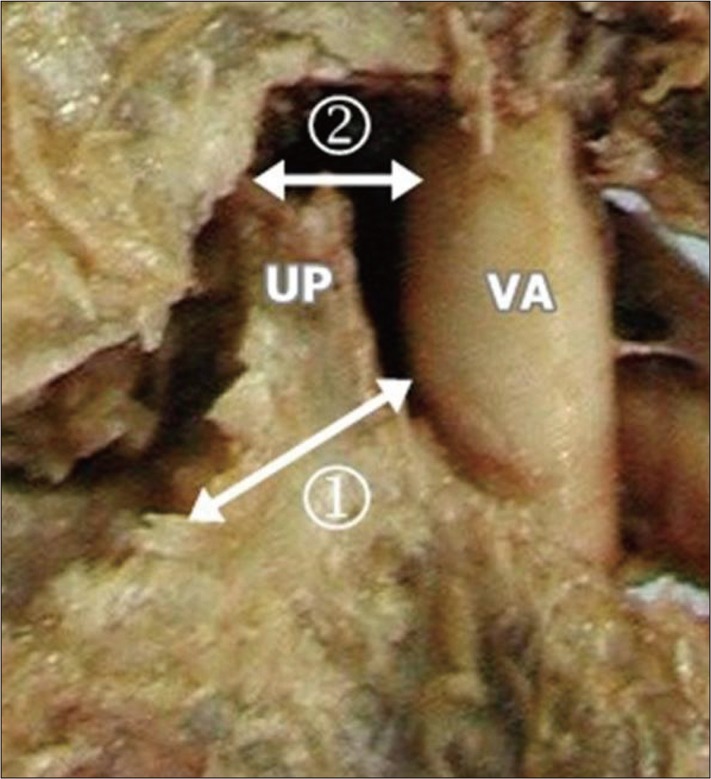
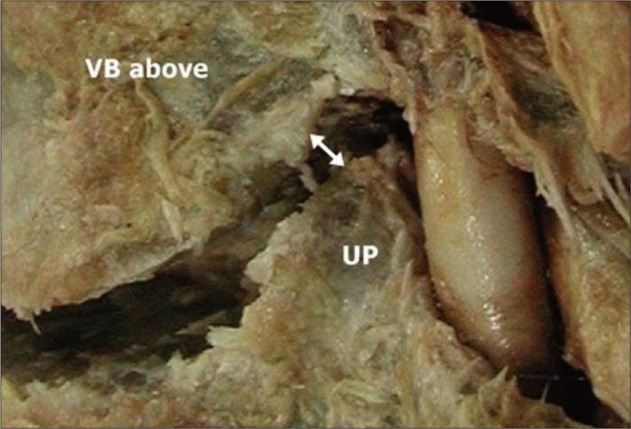
The uncinate process is a hook-shaped process on the lateral or posterior-lateral borders of the vertebral body. The height of the uncinate process is defined as the vertical distance between the upper tip of the process and the superior surface of the vertebral body (Fig. 1). The width of the uncinate process and the distances between the medial border of the uncinate process at the anterior, middle and posterior margins of the vertebral body were measured (Fig. 2). The shortest distance from the lateral wall of the uncinate process to the vertebral artery and the angle between the posterior tip of the uncinate process and vertebral artery were measured. The shortest distance from the posterior tip of the uncinate process to the nerve root was measured (Fig. 3). To elucidate the three-dimensional spatial relationship between the various structures of interest, the relative position between the uncinate process and vertebral artery, the shortest distance from the upper tip of the uncinate process to the vertebral artery and the shortest distance from the most antero-medial point of the uncinate process to the vertebral artery were determined (Fig. 4). The shortest distance from the upper tip of the uncinate process to the vertebral body immediately above it was measured (Fig. 5).
The dimensions of each cervical vertebra then were measured with an electronic digimatic caliper (Mitutoyo, Tokyo, Japan) at a precision of 0.01 mm, and all angular measurements were recorded with a goniometer that was precise to within 1°. Averages and standard deviations were calculated, and the results for each side of uncinate process were compared to clarify the difference. The results were examined with the t-test using SPSS statistical software (version 14.0; SPSS, Chicago, IL, USA) and statistical significance was set at p<0.05.
RESULTS
Height and width of uncinate process
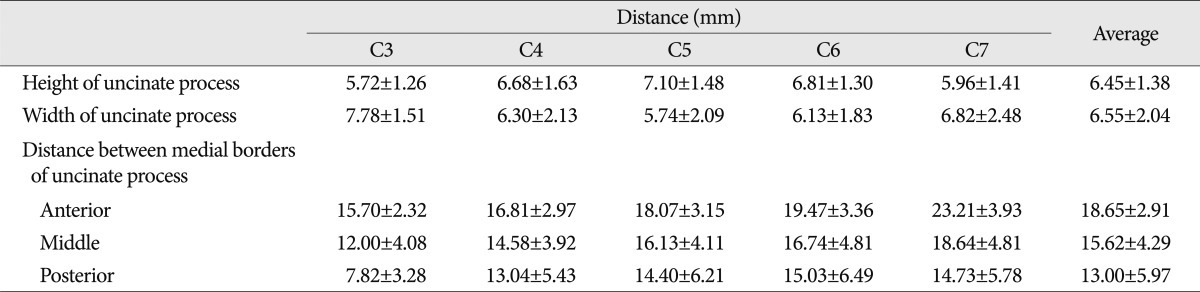
The height of the uncinate process was 6.45±1.38 (5.6-7.5) mm and the width was 6.55±2.04 (5.8-8.0) mm. It was shortest (5.72 mm) and widest (7.78 mm) at C3; while, at C5, it was tallest (7.1 mm) and narrowest (5.74 mm) (Table 1).
The distance between the uncinate processes of the vertebrae
On the transverse sections, the average distances between the medial borders of the uncinate processes from each vertebrae measured at the anterior, middle and posterior margins of the vertebral body were 18.65±2.91 (15.7-23.2) mm, 15.62±4.29 (12.0-18.6) mm, and 13.00±5.97 (7.8-15.0) mm, respectively. The distance between the uncinate processes tended to be narrower towards the posterior portion of the vertebral body. In addition, the distances of three different measuring points were wider at the lower cervical vertebrae except for the distance at the posterior of the seventh cervical vertebrae (Table 1).
Relationship between the uncinate process and vertebral artery
The distance from the uncinate process to vertebral artery was measured at three different points of the uncinate process : upper tip, lateral wall, and the most antero-medial point. The distance from the upper tip of the uncinate process to the vertebral artery was 4.32±0.84 (3.6-6.1) mm. The distance became shorter from C3 to C6 and widened at C7 which measured 4.5 mm on the right side and 3.8 mm on the left. The distance from the lateral wall of the uncinate process to vertebral artery was 2.04±0.36 (1.7-2.8) mm. This was shortest at C4 and longest at C7. This may be because the vertebral artery passes through the transverse processes only from C6 and above. The distance at the most antero-medial point of the uncinate process was 4.94±0.45 (4.2-5.7) mm. From C4 to C7, the angle between the posterior tip of the uncinate process and vertebral artery was 36.25±2.00° (32.2-42.4°), showing a slight variance (Table 2).
The relationship between the uncinate process and vertebral body immediately above it
The distance from the upper tip of the uncinate process to the inferior border of the vertebral body immediately above it was 2.46±0.33 (2.1-3.3) mm. This was shortest at the fifth cervical vertebrae and the longest at the seventh (Table 2).
The relationship between the uncinate process (posterior tip) and nerve root
The shortest distance from the posterior tip of the uncinate process to the nerve root was 1.68±0.19 (1.3-2.0) mm (Table 2).
Difference in the measurements between the right and left side uncinate process
The measurements which showed larger values for the left side than the right were as follows : the distance from the upper tip of the uncinate process to vertebral artery, the distance from the most antero-medial point of the uncinate process to vertebral artery, the distance from the upper tip of the uncinate process to Luschka joint, and the angle between the posterior tip of the uncinate process and vertebral artery. The measurements which showed larger values for the right side than the left were as follows : the distance from the lateral wall of the uncinate process to vertebral artery, the distance from the posterior tip of the uncinate process to nerve root, and the height and width of the uncinate process. Among these results, the distance from the upper tip of the uncinate process to vertebral artery, the angle between the uncinate process and vertebral artery, and the height of the uncinate process were significantly different between the right and the left side (p<0.05) (Table 3).
DISCUSSION
The uncinate process, present only in the cervical vertebrae, is located on the top of the vertebral body from C3 to C7. It is a bilateral upward bony projection arising from the postero-lateral and superior surface of the vertebral body that form raised lateral borders15). In 1858, Luschka11) named it as the "eminentia costaria" because it resembled an undeveloped costal bone, and in 1893, it was named "processus uncinatus" by Trolard20). Then, Payne and Spillane15) adopted the name "uncinate process" and reported that the processes were important in limiting lateral flexure. Luschka found a small space between the bottom of the upper vertebral body and the uncinate process, and reported that it was a joint space covered with synovial layer. This joint is now known as the "Luschka joint".
If lateral dissection was more progress during discectomy through the anterior approach, the Luschka joint can be exposed and the potential of damaging the nerve root or the vertebral artery14) is likely to be increased. From the measurements of this study, the shortest distance from the upper tip of the uncinate process to vertebral body immediately above, where the Luschka joint was located, was only 2.5 mm. Pait et al.14) came up with similar measurements (0-3 mm) and also reported that the distance widened to 6 mm after moving the cervical vertebrae. It was stressed that utmost caution should be exercised when handling lesions with the cervical vertebrae being moved, in order not to damage the nerve root or vertebral artery. They also suggested that the surgery should be performed from the lateral to medial of the uncinate process, because the shortest distance from the upper tip of the uncinate process to the vertebral artery was only 0.8-1.6 mm. From the authors' measurement, the distance was 3.6-6.1 mm, which was slightly different from the result of Pait et al.14). This may be caused by the different measurement reference points used; the authors measured the vertebral artery distance from the medial point of the uncinate process, while the prior studies measured the distance from the lateral wall of the process.
The vertebral artery, which is separate from the subclavian artery, runs upward and rearward, and passes through the transverse foramen of the sixth cervical vertebrae13). The transverse foramens, along with the vertebral artery, are usually located in a more posterior position from the sixth to the third cervical vertebrae12). In front of the transverse foramen, there is the anterior tubercle where the longus coli muscles are attached, and the inter-transverse muscles are located in-between. The uncinate process is located in the medial point. The nerve root passes through the posterior part of the cervical vertebrae. The uncinate process, which is adjacent to the vertebral artery and nerve root, is often exposed and operated on during the anterior cervical surgery. For radiculopathy from spondylosis, the recommended range of transverse decompression is, in general, 15-20 mm1). Cooper reported that this range of decompression would be safe because the vertebral artery is located in 5 mm after removing 20 mm of vertebral body on both sides, considering that the distance between the medial borders of the transverse foramens was about 30 mm3). However, in this study, this distance showed a wide variation, from 7.8-15.0 mm and, thus, it is recommended to determine the level of decompression for each patient after measuring his/her radiologic distance rather than generally applying the level of decompression.
In case of myelopathy, decompression between both uncinate processes is sufficient; however, in case of radiculopathy, more lateral decompression is required to decompress the neural foramen. This may damage the nerve root near the uncinate process, and the risk is even higher if a large spur causes anatomic confusion. If the removal of the spur is limited in order to avoid complications during the surgery, it can lead to insufficient decompression of the neural foramen. To facilitate the surgery without complications, the authors measured the shortest distance from the posterior tip of the uncinate process to the nerve root which was 1.3-2.0 mm, showing a slight variance among measurement points. In other words, when posterior tip of the uncinate process are exposed during the neural foramen decompression for radiculopathy, it should be considered that nerve root can be located 1.3 mm apart from the process while removing spur.
Anterior approach for discectomy has been widely used because of its successful results. Recently, microforaminotomy, a minimally invasive surgery, has been developed and is increasingly being adopted9). It is a technique that removes a part of the uncinate process and relieves pressure upon the affected nerve root, by approaching from lateral border to medial boarder of uncinate process. This can minimize damage to the affected vertebrae's biomechanical functions, because only the lesion is removed and the discs are preserved without intervertebral body fusion or fixation. However, care should still be taken to avoid damaging the vertebral artery and nerve root during the grinding of the uncinate process.
Lu and Ebraheim10) and Chang et al.2) studied the anatomical relationship between the longus colli muscles and vertebral artery in cadavers in order to prevent damaging these structures during surgery and thus, reduce complications. Lu and Ebraheim10) measured the distance from the medial border of the longus colli muscles to the medial border of the vertebral artery. They found that the longest distance between these structures were at the sixth cervical vertebrae (11.5 mm). The distance was relatively narrower in the upper cervical vertebrae and the shortest distance was 9.0 mm at the third cervical vertebrae. According to the measurements by Chang et al.2), the average distances in the 3-4, 4-5, 5-6 cervical vertebrae were 13.3-13.6 mm, and the average distance in the 6-7 cervical vertebrae was 14.7 mm. Although these two studies reported different measurement results, both agreed that the distance was narrower at the upper cervical vertebrae. These studies also suggested that extra careful operation is required at the seventh cervical vertebrae because the vertebral artery is located in front of the transverse process. However, if the logus colli muscle is removed during the surgery, it would naturally be difficult to determine the distance between the longus colli muscle and vertebral artery. Thus, the authors used the uncinate process as the reference point to determine its distance from the anatomical structures of interest during surgeries. Considering that the width of the uncinate process is 5.8-8.0 mm, the operator should be aware that the lateral wall of the uncinate process would be reached when he/she drills a hole of similar depth oriented horizontally and originating from the medial border of the uncinate process. According to Pait et al.14), the width of the uncinate process was 5.3-6.7 mm, which was slightly narrower than the authors' result. This difference is attributed to the different measurement perspectives used. The authors of the current study measured the longest width of the uncinate process from the transverse section of the specimen while Pait et al.14) measured the width of the uncinate process from the anterior view of the vertebral body. Since the distance from the lateral wall of the uncinate process to vertebral artery was only 1.7-2.8 mm, extra care is needed when the lateral wall is exposed.
Oh et al.12) showed that the distance from the medial border of the uncinate process to the medial surface of transverse process was less than 6 mm, a little longer than the current authors' measurement (4.9 mm). Since different anatomical measurement studies on cadavers often use dissimilar measurement points in addition to the already subjective views of the researchers, this study used the uncinate process as the reference point for measuring the various distances and angles for the anatomic structures of interest in order to improve the practicality of the information for the surgery. In this study, the shortest distance from the antero-medial point of the uncinate process to the vertebral artery was 4.7-5.7 mm. Considering that the first grinding point of the uncinate process is the most antero-medial point, drilling a 4.7 mm - deep hole through the uncinate process implies that the tip of the bit may very well reach the vertebral artery. Additionally, the lateral wall of the uncinate process is only 1.7-1.8 mm away from the vertebral artery. Understanding these anatomical relationships will help to detect the exposed points of the later wall of uncinate process and the vertebral artery. The angle between the posterior tip of the uncinate process and vertebral artery was 32.2-42.4°. It indicates that when the posterior tip of the uncinate process is exposed, the vertebral artery is located on the imaginary line along this angle, and the intersecting point between this line and 4.7-5.7 mm apart from the antero-medial point of uncinate process can be estimated as the location of vertebral artery.
Several researchers suggested various perspectives on the safety boundary. Jang et al.8) stated that the surgical procedure could be done with a hole of 7 mm diameter at 15 mm off-center of the vertebral body. Lu and Ebraheim10) stated that drilling a 5-6 mm deep hole, directed either vertically or horizontally, was safe at a point 5-6 mm medially from the lateral border of the uncinate process. Chang et al.2), whose study was based on measurements using the longus colli muscle as the reference point, reported that the medial wall of the vertebral artery was located within 13-15 mm when the vertebral body is removed around at 40° with respect to the medial border of longus colli muscle. Microforaminotomy in the cervical spine is a minimally invasive technique that involves a limited surgical view. The limited surgical view can cause confusion of the anatomical relationships. Consequently, comprehensive anatomical measurements in various perspectives should be consulted for successful surgery.
CONCLUSION
From the various measurements concerning the uncinate process in relation to its neighboring structures taken at the level of the third through the seventh cervical vertebrae and using the uncinate process as a reference point, the following conclusions can be drawn. Since confusion over the anatomical structures can easily occur due to the limited surgical view associated with anterior cervical surgery, the measurement results taken from the subaxial cervical vertebrae in this study will contribute to a successful surgery.





 XML Download
XML Download