

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Intracranial hypotension syndrome (IHS) is characterized by a postural headache that is aggravated in the erect or sitting position and relieved in the supine position. It is often associated with one or more of the following symptoms : nausea, vomiting, dizziness, diplopia, photophobia, hearing impairment, neck stiffness, and blurred vision6).
Acquired or secondary intracranial hypotension is less common but has been reported after spinal procedures such as lumbar discectomy and dural puncture for myelogram, spinal anesthesia. Incidental durotomy is a frequent complication of lumbar spinal surgery. Treatment options range from conservative therapy to surgical correction.
We report a case of a 54-year-old man who was successfully treated with epidural blood patches for intracranial hypotension due to CSF leakage into the lumbosacral area after L4-5 discectomy.
CASE REPORT
A 54-year-old male admitted to the ER complaining of headache
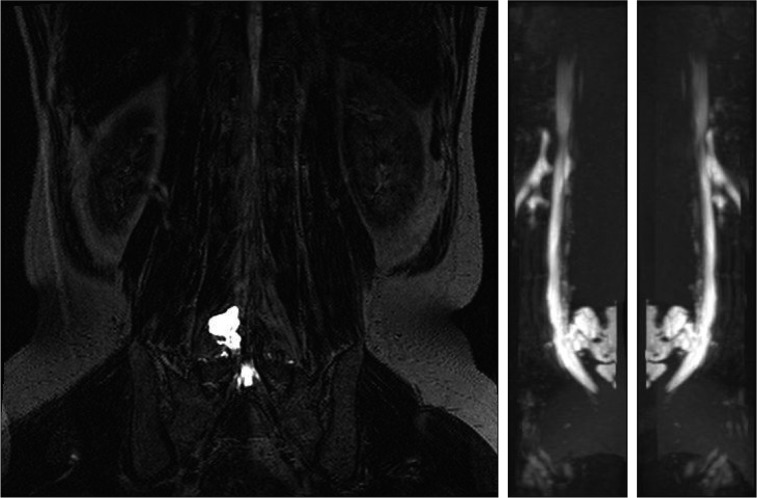
from 13 days ago. It did not occur when lying down but became intensely squeezing around the occipital area within 10 seconds after being seated or standing. Symptoms were accompanied by nausea and vomiting. Visual analog score (VAS) was 8 at standing. Past medical history was insignificant other than undergoing L4-5 laminectomy and discectomy at a local hospital 15 days ago. Physical examination did not display any neurologic findings such as neck stiffness and laboratory results as well as brain MRI findings were not remarkable. Under the strong impression of intracranial hypotension, he admitted to neurology department and underwent conservative therapy including absolute bed rest (ABR) and hydration. A MR myelogram was performed, showing a pseudomeningocele accompanied by large CSF leakage in the lumbosacral area (Fig. 1).
Because resolution of symptoms was unsatisfactory, an epidural blood patch was placed on the sixth admission day. After placing the patient in a prone position, a 22 gage touhy needle was inserted through the L5-S1 epidural space through a paraspinal method. After confirming the epidural space by the loss-of-resistance technique, a dye was injected to confirm the epidural space with the C-Arm. Then the epidural patch was placed with 12ml of autologous blood.
VAS one day after intervention was reduced from 6 to 2. After three days of ABR following the procedure, the patient practiced changing positions by sitting. Symptoms were not aggravated when standing up. Five days after the procedure, the patient did not complain of any symptoms (VAS 0). Follow up MR myelogram showed decreased pseydomeningocele size caused by CSF leakage (Fig. 2).
We decided to perform one more procedure of epidural patch placement because of the residual CSF leakage 6 days after the first intervention. A total of 10 mL autologous blood was injected, and the patient was discharged the next day. Follow up for six months confirmed no recurrence of symptoms (Fig. 3).
DISCUSSION
Intracranial hypotension syndrome can occur spontaneously. Acquired or secondary intracranial hypotension is less common but has been reported after spinal procedures. Guerin P et al. reported that the incidence of incidental durotomy during spine surgery was 3.84% in patients who underwent spinal surgery at a single spine unit5). In one study looking into medicolegal aspects of spine surgery, 146 malpractice cases were reviewed and incidental durotomy was second most frequent complication in such cases4). The study has shown that potentially serious problems such as pseudomeningocele, CSF fistula formation, meningitis and arachnoiditis with subsequent chronic pain are all related to dural tears and CSF leakage after spinal surgery.
Dural tears that occur during surgery can be treated with primary repair when recognized. Good long-term clinical results were noted in all patients with durotomy repaired at identification and are comparable to long-term results of patients undergoing similar surgical procedures but without durotomy. However, Cammisa et al.1) reported the incidence of clinically significant durotomy occurred during surgery but not indentified at the time was 0.28%, and patients had subsequent surgical repair of dural defects because of failure of conservative therapy. In one study which investigated incidental durotomy during spine surgery and its treatment, in addition to primary repair, drain, bed rest, hydration, antibiotics had been used for treatment by spine surgeon7). However to our knowledge, there have been no previous studies which compared the effects of epidural blood patch for the treatment of incidental durotomy with other treatments.
Epidural blood patch has been employed over the last five decades in the treatment of postdural puncture headache (PDPH) and has proven to be beneficial. The mechanism by which an epidural blood patch (EBP) relieves PDPH is not known. The "plug" theory for symptom resolution proposes that the blood injected during EBP forms a gelatinous plug, sealing the dural hole and preventing further CSF leak into the epidural space. In the absence of continued loss, regeneration of CSF restores CSF pressure and alleviates the headache3). The "pressure patch" hypothesis emphasizes the impact of injected blood or other fluid (crystalloid or colloid) on the pressure dynamics of the CNS. The injected fluid increases epidural pressure which, in turn, elevates subarachnoid CSF pressure by compressing the dura8).
The optimal volume of blood that must be injected is controversial but recommended volumes have increased over time. Crawford's initial experience using 6-15 mL produced a 30% failure rate while later experience with 20 mL produced a 96% success rate, so 20 mL became the recommended volume and has since become commonly cited as a "target volume" to enhance patch efficacy2). However, the effects of EBP in intracranial hypotension are mostly focused on post-dural puncture during CSF tapping or spontaneous intracranial hypotension. There are only few reports on EBP after incidental dural tear during spine surgery.
EBP has been shown to be effective in patients with spontaneous dural tear. Even patients with rather large amount of CSF leakage and patients with severe complications such as intracranial hematomas have been effectively treated with EBP, so we considered EPB for postoperative incidental durotomy due to such evidence. Two trials of EBP that relieved symptoms and improvement were also shown in cisterongraphy. The effects of EBP in postoperative intracranial hypotension cannot be discussed after one successful clinical trial, but additional trials and studies can provide the basis of EPB treatment in such cases.
When incidental durotomy was recognized postoperatively, conservative therapy or surgical correction has been the therapeutic choice. Surgical correction can be considered when there is no response to conservative therapy. EBP is as less invasive therapeutic alternative. However, because there has been no report on indication for EBP according to the degree of dural injury or the size of peudomeningocele, additional research is needed.
In our case, the patient underwent L4-5 spine surgery at a local orthopedic, but dural injury was not recognized at that time. After admitting to our hospital, he was diagnosed with intracranial hypotension caused by incidental durotomy during surgery. There was no significant resolution of symptoms after conservative therapy including the five days of bed rest and hydration. After two procedures of epidural blood patch, the patients became asymptomatic.


 XML Download
XML Download