

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hemifacial spasm (HFS) is a movement disorder characterized by involuntary contractions of the facial muscles. Although the mechanism of HFS is not yet well established, vascular compression of the facial nerve root exit zone (REZ) is one likely mechanism given the effectiveness of microvascular decompression (MVD) in the treatment of the disorder1,7,9). Moreover, the vascular compression theory has been accepted as the etiology of rare secondary HFS in some cases of cerebellopontine angle (CPA) tumors, aneurysms, and arteriovenous malformations (AVMs)5,7,10,13,17,18). However, another theory for the mechanism of HFS, hyperexcitability of the facial nucleus, has also been suggested. This theory was inspired by various cases of brain stem gliomas, 4th ventricle tumors, brain stem hemorrhages, and lacunar infarctions without direct vascular compression2,6,21,22).
We present a case of HFS in the setting of coinciding brain stem hemorrhage and proximal ligation of the contralateral vertebral artery (VA) for the treatment of a fusiform aneurysm of the distal VA and discuss the possible etiologies of HFS in this patient.
CASE REPORT
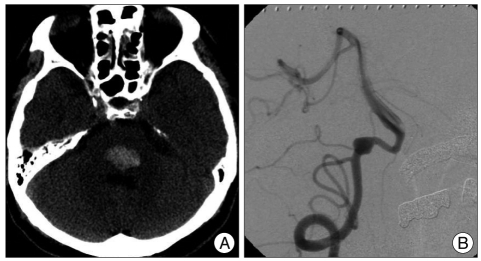
A 51-year-old male presenting with abrupt onset drowsiness was admitted to our hospital. A neurological examination revealed mildly confused orientation, gaze limitation to the left side in both eyes, mild palsy of the left face, and right hemiparesis. The patient had a history of hypertension which was being medically managed. Brain computed tomography (CT) revealed a hematoma in the posterior portion of the lower pons with minimal mass effect (Fig. 1A). After 2 months of conservative management, his mental status and gaze limitation were completely recovered while the facial palsy and hemiparesis were improved but still remained.
Magenetic resonance angiography (MRA) was performed to evaluate for a possible lesion causing an intracranial hemorrhage (ICH); a fusiform aneurysm was found in the right VA. Although the aneurysm was located adjacent to the pontine hematoma, it appeared unlikely to be causing an ICH because the hematoma was totally encased within the pons and there was no evidence of subarachnoid hemorrhage on serial brain CT and MR. On angiography, the fusiform aneurysm was located distal to the origin of the posterior inferior cerebellar artery (Fig. 1B). Because there was no neurological deterioration during a thirty minute balloon test occlusion, we performed proximal ligation of the VA via a retromastoid suboccipital craniotomy. The procedure was performed without any complications and the patient was discharged and received physical therapy in local clinics.
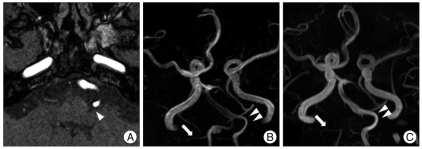
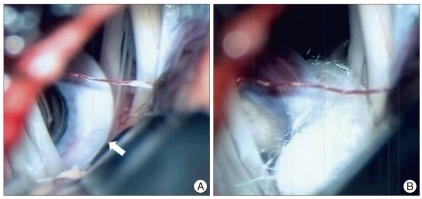
Eight months after the operation the patient visited our hospital complaining of involuntary left facial twitching. The spasm had initially begun in the left orbicularis oculi muscle during physical therapy. Despite two years of medication, the frequency of the spasms increased, the severity of the spasms increased, and the spasms spread to involve other ipsilateral facial muscles. During careful consideration of the cause of these spasms we identified a hemodynamic difference between the pre- and post-ligation MRAs. The left VA, which was compressing the facial nerve REZ, did not change architecturally but enlarged in diameter (Fig. 2). Although pontine ICH is also considered a potential cause of HFS, the long interval between the ICH and the onset of HFS prompted us to perform MVD in this patient. The facial nerve REZ was subsequently found to be compressed by an elongated VA (Fig. 3). Immediately after decompression the patient was free from symptoms and has not had a recurrence during 2 years of follow-up.
DISCUSSION
Although the mechanism of HFS is not yet clearly defined, vascular compression of the facial nerve REZ is generally considered the primary etiology of HFS9,11). Offending vessels are most often found on preoperative radiologic evaluation or during surgery; MVD of these offending vessels has yielded successful outcomes in large serial studies1,8). In several rare secondary causes of HFS, including CPA tumors, aneurysms, and AVMs, compression of the facial nerve REZ by altered vasculature is also considered the etiology of HFS5,7,10,13,17,18).
Another theory for the mechanism of HFS, hyperexcitability of the facial nucleus, has also been suggested15,20). Specifically, in cases of brain stem gliomas, 4th ventricle tumors, brain stem hemorrhages, and lacunar infarctions without vascular compression, facial nucleus hyperactivity has been suggested as the etiology of HFS2,6,21,22). Moreover, Chang et al.4) suggested that some unknown factors, in addition to vascular compression, may contribute to the etiology of HFS because HFS did not always resolve despite sufficient decompression. Previously, a case of pontine ICH secondary to head trauma presented with HFS without any vascular compression22). In this case, the HFS developed 2 days after the ICH; the HFS subsequently resolved with systemic steroid injection. Interestingly, our patient had both possible causes of HFS, pontine ICH and vascular compression.
Increased hemodynamic stress of the VA after contralateral VA occlusion has been suggested in several cases3,12,14). There have been two reported cases of de novo dissecting aneurysm of the VA that occurred 3 weeks and 5 months after balloon occlusion of the contralateral VA. Mizutani and Aruga14) reported a case of enlargement of a pre-existing VA dissecting aneurysm after contralateral VA occlusion which presented as facial spasm 6 years after VA occlusion.
A meaningful relationship between an increase in hemodynamic stress and the development of HFS has been suggested by some authors; two cases of VA aneurysms causing ipsilateral HFS resolved after proximal occlusion of the VA16,19). One case consisted of a VA dissecting aneurysm that was occluded by endovascular coil embolization and the other case consisted of a VA fusiform aneurysm treated with surgical ligation. In both cases the spasms disappeared immediately after proximal occlusion without any need for further treatment of the spasms. In our case, there was no development of a dissecting aneurysm in the contralateral VA after proximal VA ligation; however, preoperative- and 20-month postoperative-MRA demonstrated increased signal intensity and enlarged VA diameter, suggesting increased hemodynamic stress (Fig. 2B, C).
In our case, we had to consider both nucleus hyperexcitability from a pontine ICH and vascular compression by altered hemodynamics as potential causes of the HFS. The patient had not experienced spasm prior to the ligation, although the facial nerve REZ was affected by the VA on preoperative MRA. However, we ultimately decided to perform MVD because of the relatively long interval from the ICH to onset of the HFS and because a MRI performed after the onset of the HFS showed that the hematoma had already resolved. The spasm completely disappeared immediately after decompression of the offending VA. Therefore, we concluded that the increased hemodynamic stress on the left VA following contralateral VA occlusion had applied pressure on the facial nerve REZ and triggered the onset of the HFS in this patient.
CONCLUSION
To the best of our knowledge, this is an extremely rare and unique case of HFS. We suggest that hemodynamic changes themselves could be causative of HFS without pathological vascular alterations. Furthermore, even in cases where there are other possible causes of facial nucleus hyperexcitation, evaluation for vascular abnormalities should be performed.
 XML Download
XML Download