

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Spinal epidural abscesses (SEA) are rare pathologies and the most frequently cause is Staphylococcus Aureus. The incidence of spinal epidural abscesses account approximately 1 in every 10000-hospital admissions29). In addition to Staphylococcus aureus, other bacteria or fungi species such as Candida glabrata, Actinobacillus, Pseudomonas, Mycobacterium tuberculosis, Nocardia, Pneumococcus, Salmonella enteritidis and Brucella species can cause SEA6,21,23). Diabetes mellitus, intravenous drugs, alcohol abuse, and immunosuppression predispose to infections resulting in SEA6,21,23,25,31).
Brucellosis is a systemic, zoonotic disease caused by an aerobic, gram negative and non-encapsulated cocobacillus, which may affect many organ systems5,33). Out of six, four brucella species, Brucella abortus, Brucella suis, Brucella canis, Brucella melitensis can cause human diseases. Brucella melitensis is the most virulent species. Humans are infected by direct contact with infected animals or materials and ingestion of animal products, particularly raw milk and cheese14,15). Osteomyelitis usually occurs at the vertebrae especially at the lumbosacral area. Involvement of the epidural space is rare, but the formation of SEA was reported in less than 1.5% of the cases with neurological complications and generally associated with spondylitis16,23,28). The frequency of spinal involvement usually seen at the lumbar spine, thoracic and cervical spine respectively1,7,26,30).
Osteoarticular involvement is the most common complication, which was reported up 10 to 85% in most series1,7,10,19,26,30). Sacroileitis and arthritis represent the acute form and frequently respond to the standard theraphies. It has been reported that the spinal column is generally affected with subacute and chronic forms of brucellosis1,22). Furthermore, spinal brucellosis usually affects elderly patients, whereas sacroileitis and arthritis are usually reported in the first three decades of life1,7). Infection of the epidural space results from hematogenous dissemination or local extension of the infection from adjacent structures, which might be originally infected from hematogenous spread. Approximately half of epidural abscess result from hematogenous spread to the epidural space16,23,28).
CASE REPORT
Case 1
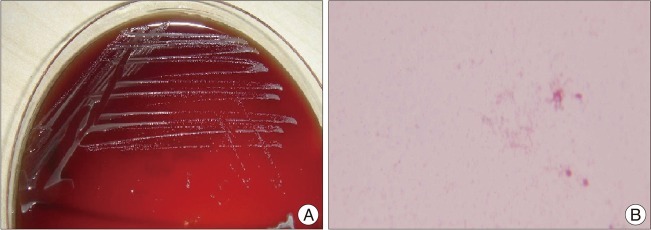
A 61-year-old, male farmer was admitted to the hospital with complaints of weight loss for more than a month, acute severe neck and right shoulder pain of ten days duration. Pain progressively had worsened and became incapacitating before admission. Fever with rigors, fatigue, malaise and profuse night sweating were added to the symptoms. There was no significant predisposing basal illness or factor in history except consumption of fresh goat cheese. Neurological examination revealed 3/5 motor weakness at the shoulder abduction, C4-5 radicular hypoesthesia, hyperactive deep tendon reflexes and no meningeal irritation signs. The results of the blood tests revealed positive Wright agglutination reaction at a titer of 1/40. White blood cell count (WBC), erythrocyte sedimentation rate (ESR) and C-reactive protein values (CRP) were 8700 mm3, 32 mm/h, 30.7 mg/dL respectively. Blood culture was negative. Magnetic resonance imaging (MRI) studies revealed anteriorly spinal cord compression due to T1-weigted iso-hypointense, T2-weighted hyperintense epidural fluid collection originating from C4-5 disc space. A right anterior cervical approach was performed. A needle was inserted to the C4-5 disc space to confirm by C-arm scopy. Spontaneous drainage of yellowish, purulent material from the disc space (Fig. 1C) was observed after insertion, and culture samples were taken immediately. After achieving the neural decompression due to drainage of abscess, C4-5 simple discectomy was completed without instrumentation because there were no clinical and/or radiological instability or collapse at disk space. A rapid recovery occurred in neurological sign and symptoms of the patient after the operation. Broad spectrum antibiotics consisted from 1 gr IV ceftriaxone BID and 2 g IV ampicilline-sulbactam TID at early postoperative period before isolation of Brucella melitensis at eosin methylene blue (EMB) agar, which took 6 days (Fig. 2). Just after achieving the receipt of surgical sample cultures' results, treatment protocol was substituted to a regimen consisting of PO doxycycline 200 mg/day and PO rifampicin 600 mg/day for 3 months. Control MRI was performed at the postoperative 3rd month visit and complete recovery was demonstrated (Fig. 3).
Case 2
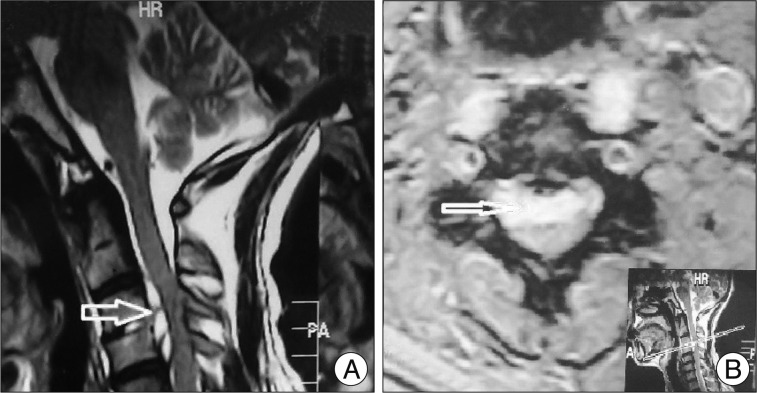
A 63-year-old, male farmer was admitted to hospital with severe neck pain and hypoesthesia on his upper extremity lasting for 5-month. Pain was unresponsive to the medical treatment. In the history, he had weight loss, night sweats, fatigue and severe malaise for 5-month. There was no significant predisposing basal illness or factor in history except consumption of fresh dairy products. Neurological examination revealed C3-4 radicular hypoesthesia without motor weaknes, hyperactive deep tendon reflexes, no meningeal irritation signs. Wright aglutination reaction tests revealed positive at titer of 1/160 which was. WBC, ESR and CRP values were 7.06 mm3, 12.0 mm/h, 3.78 mg/dL respectively. MRI studies revealed epidural abscess at spinal C3-4 level. T2-weigted non-enhanced sagittal and axial magnetic resonance images revealed C3-4 anterior cervical spinal cord compression due to a hyperintense lesion which was considered as fluid intensity (Fig. 4). Incapacitating severe pain with long duration and unsatisfactory medical treatment leaded us to perform a right anterior cervical approach. C3-4 anterior micro-discectomy was performed and culture samples were taken immediately during the abscess drainage. Then polietheretherketone (PEEK) cage was placed in to the C3-4 disk space due to risk of decrease in disk space height. Neurological symptoms and findings of the patient were rapidly recovered after the operation. Postoperatively, triple antibiotics regimen were given, which consisted of 1 g IV ceftriaxone BID, PO doxycycline 200 mg/day and PO rifampicin 600 mg/day until isolation of Brucella melitensis. Treatment protocol was substituted to a regimen consisting of PO doxycycline 200 mg/day and PO rifampicin 600 mg/day for 3 months. Control MRI was performed at the postoperative third month visit and complete recovery was demonstrated (Fig. 5).
DISCUSSION
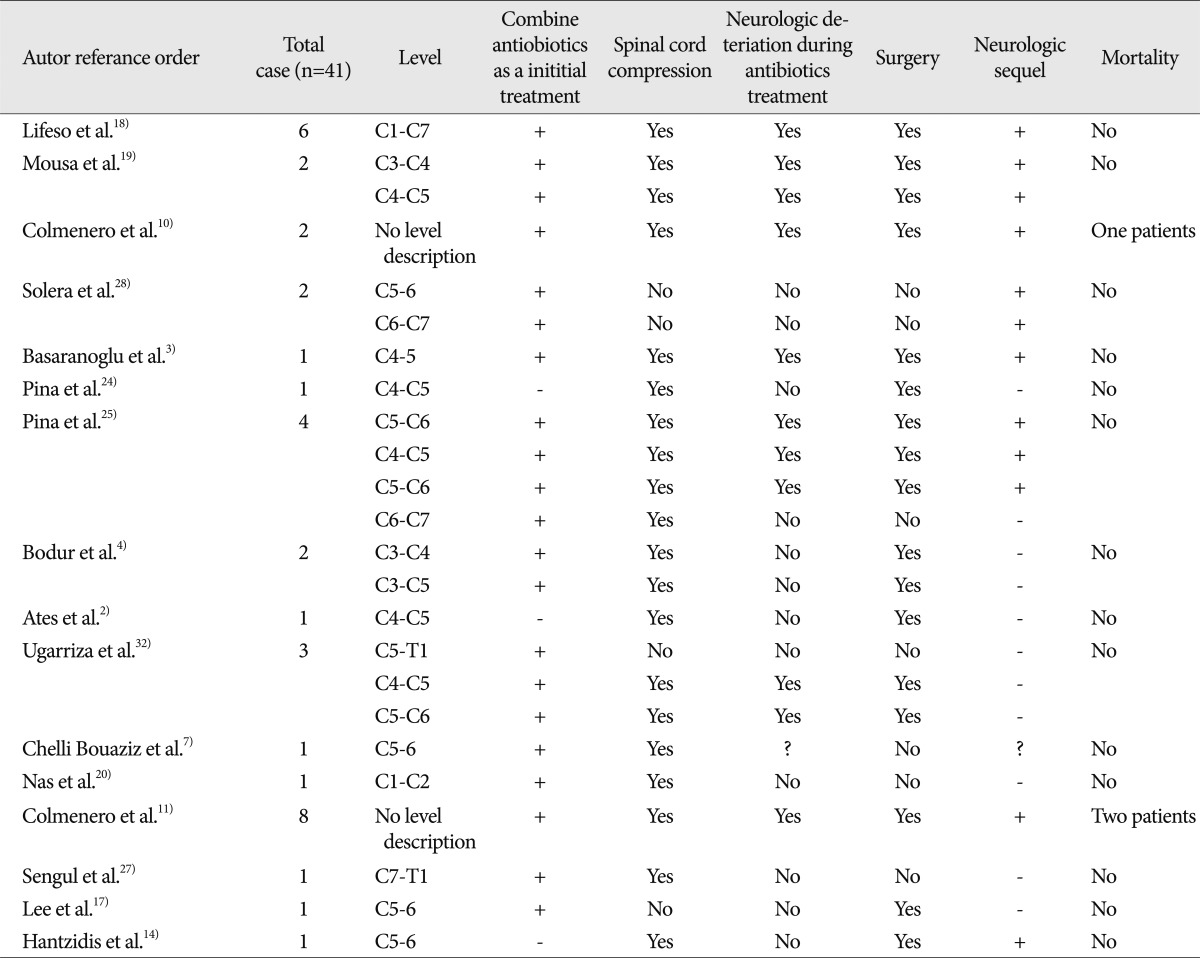
Cervical spinal epidural abscess is an extremely rare condition with brucella species that is responsible for about 0.1% of cases25). Literature research yielded sixteen reports, which are deal with only cervical involvement due to the brucellosis (Table 1). Mortality is seen only in three patients. In a retrospective analysis of 1028 patients, it was revealed that the most frequent involvement was osteoarticular involvement, which was found in 260 cases (25%); followed by spondylitis, which was found in the 32 patients (3.1%)5). Patients with spondylitis are more likely to be older and to have longer durations of symptoms before the therapy28).
Brucellar spondylitis is described in two forms as focal and diffuse. The focal disease is seen at the anterior superior portion of an endplate, which is known to have rich blood supply. The diffuse form involves the vertebral body, adjacent disc, and epidural space. Disease spread via the vascular communication and ligaments7,16,22,23,28).
In one of the retrospective multicentre studies with 219 patients, it was reported that, 105 (48%) of these patients had brucellar osteomyelitis and cervical localization was seen in 16 (7.3%)9). In another retrospective study on 263 patients, Colmenero et al.10) reported that 65 patients had osteoarticular complications; and of these patients, 38 (58%) had brucellar spondylitis and cervical localization was seen in 2 (3%). Mortality was seen in only one case secondary to respiratory complications due to the cervical medullar cord compression.
Treatment of brucellosis must control the illness effectively and prevent complications including relapses. Combined medical treatment with a prolonged course is recommended. Currently, the recommended combinations are doxycycline 200 mg/day, and rifampicin 15-20 mg/kg per day, or doxycycline 200 mg/day plus streptomycine 1g/day i.m. as an initial treatment regimen. The optimal duration of therapy is unknown, but at least 3 to 6 months would be beneficial in the osteoarticular brucellosis7). However, there is no standard therapy protocol in chronic brucellosis5,33). First line antimicrobial regimen is doxicycline+streptomycine (200 mg/day/12 weeks and 1 g/day/2-3 weeks, respectively). If there are adverse reactions or contraindications, alternative combination of the antibiotic treatment may be doxycycline+rifampin or co-trimoxazole+rifampin or ciprofloxacin+rifampin or ciprofloxacin+streptomycin1).
Although, Solera et al.28) reported that initial treatment requires antibiotic therapy, there are a few cases, in which cervical epidural abscess was treated successfully by combined antibiotic regimen without surgery in the presence of spinal cord compression signs. Pina et al.25) reported four cases of cervical spinal epidural abscess due to the brucellosis. Antibiotic therapy was chosen as initial treatment, but three patients underwent surgery due to neurologic deterioration, whereas only one patient had been treated successfully with antibiotics.
Management of cervical epidural abscess due to Brucella species remains controversial in terms of antibiotic therapy alone. According to the literature, antibiotic therapy with combination of agents is preferred frequently as initial treatment3,4,7,10,11,17-20,25,27,28,32) in contrast some authors suggest surgical approach as an initial treatment8,9,12-14,18,30). Although neurological sequel is reported frequently, there are only three reports deal with first line treatment option of surgical intervention2,14,24).
Vertebral osteomyelitis with/without SEA is a serious, potential complication of brucellosis, which often require surgical treatment11). In order to prevent neurologic complications, accurate and early diagnosis is essential25). Although, medical treatment might be enough at early stage of the brucellosis, in older (50-60 years) cases with unsatisfactory respond to medical treatment (antibiotic therapy combined with analgesics), neurologic weakness (tetraplegia or tetraparasia), first motor neuron findings (pathologic reflexes and hyperreflexia on the upper and lower extremities) and long duration of the complaints, it should be kept in mind that disease could be at an advanced stage (subacute or chronic); therefore surgical management should be indicated8,9,12-14,18,30). Thus, early surgical approach can be provide some benefits such as, achieving neural decompression; rapid relief in symptoms and obtaining fresh sample for microbiologic culture and microscopic analysis for differential diagnosis before deterioration of neurological and clinical parameters1,4,11,19,32).
Surgical techniques may vary including simple discectomy, aggressive corpectomi plus anterior expandable cage or iliac bone autograft plus anterior plate fixation and simple discectomy plus PEEK Cage fusion.
It might be speculated that first line treatment protocol should be antibiotic therapy with combination of agents, if there are no neurological compression sign and symptoms due to spinal cord compression1,8,30). Although Case 2 had severe, incapacitating neck and shoulder pain and hyperreflexia without neurological deficit and in contrast Case 1 had neurological deficit, long duration of the complaints and benefits of early spinal cord decompression leaded us to prefer surgical treatment subsequently combined with antibiotic therapy as initial treatment in both cases.
In conclusion, however, the first line treatment option of the ostearticular involvement of brucellosis with/without spinal epidural abscess is antibiotic therapy, it should be kept in mind that the first line treatment must be surgical intervention in case of neurological signs and symptoms due to the spinal cord compression, clinical and/or radiological instability and no respond to anbiotic and/or analgesic therapy in order to prevent neurological sequel. Early diagnosis and appropriate early antimicrobial therapy combined with surgery is associated with an excellent prognosis. There are no strict limitations in terms of accurate treatment options; it relies on experience of the surgeon and clinical and/or radiological findings of cases individually.



 XML Download
XML Download