

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Meralgia paresthetica (MP) is a mononeuropathy resulting from the compression of the lateral femoral cutaneous nerve (LFCN) as it crosses between the anterior superior iliac spine (ASIS) and the inguinal ligament to enter the thigh20,28). The nerve receives sensory input from the skin of the anterolateral thigh (Fig. 1A). Affected patients consequently experience a very prominent painful dysesthesia and, less commonly, vasomotor disturbance in the cutaneous distribution of the nerve. The term MP was first coined by Roth21) in 1895. However, despite its long-term recognition, very few studies have been published on the surgical management and outcome of this condition10,17,18,23,26).
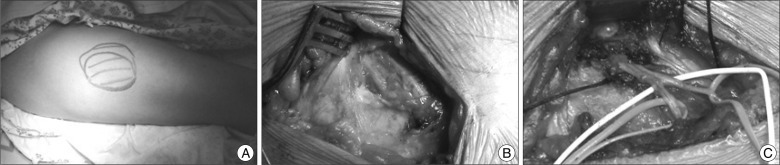 | Fig. 1Operative findings of decompression with neurolysis. A : A clinical photo showing the maximal painful dysesthetic area of right lateral theigh. B : Initial exposure of the course of lateral femoral cutaneous nerve. Note two branches, anterior and posterior branches of lateral femoral cutaneous nerve. C : Final operative photograph showing complete decompression along the course of lateral femoral cutaneous nerve. Decompression of the nerve was performed at the level of the iliac fascia, the inguinal ligament, and the fascia of the thigh distally.
|
Two types of operative techniques, decompression with neurolysis and transection of LFCN, have been proposed to be effective for MP23,27). Transection of the nerve at its exit from the pelvis is a simple and effective procedure provided the nerve can be found,26,28). However, such a procedure results in anesthesia over the lateral thigh23). Symptomatic relief expected of neurolysis has not been consistently reported in the literature3,14,17,18,23). In an effort to provide clarification, we report long-term results of neurolysis for MP from our collected series of 11 cases.
Go to : 
MATERIALS AND METHODS
Selection criteria
Over an 8-year period (2003-2010), all patients who underwent neurolysis for MP were included in this study. These patients were referred by general physicians with distressing symptoms notwithstanding conservative management for some weeks to months. The diagnosis of MP was typically delayed until patient visit to our outpatient department. Most patients diagnosed as MP were treated successfully without surgery. These non-operative measures included usage of nonsteroidal anti-inflammatory drugs (NSAIDs), injection of steroid and local anesthetics, advice on weight loss, and avoidance of local physical constricting factors. Neurolysis was performed when adequate symptomatic relief could be achieved by at least 3 months of non-operative treatment.
Diagnosis of MP
The diagnosis of MP was confirmed with at least three repeated blocks of the LFCN. In four of 11 patients, electrodiagnosis was conducted and a decrease in the amplitude of the sensory nerve action potential (SNAP) was detected with side-to-side amplitude difference.
Neurolysis
Under general anesthesia, a transverse incision was made 1 cm below the ASIS along the skin crease. Dissection was carried out down to the fascia lata to expose the nerve under loupe magnification. Particular attention was paid to its anatomic variability. The subfascial plane was exposed carefully to identify the nerve. The nerve was followed proximally to the inguinal ligament, and a blunt probe was used to demonstrate the tunnel between ASIS, inguinal ligament, and origin of Sartorius (Fig. 1B). The inferior leaf of the inguinal ligament was lifted, divided, and splayed. This decompressed the nerve anteromedially. The nerve was then mobilized and the fascial ridge between the ASIS and Sartorius origin, over which the nerve bridges, was divided, decompressing the nerve posterolaterally (Fig. 1C). Complete lysis was achieved by freeing the nerve at three levels23) : 1) the tendinous arc from the iliac fascia, 2) the inguinal ligament anteriorly and a sling of fascia posteriorly, and 3) distally at the deep fascia of the thigh along each division. A probe was then introduced parallel to the nerve distally to identify any constricting distal aponeuroticofascial tunnels. With hemostasis obtained, the wound was closed in two layers. No drains were left. The patient was discharged home on postoperative day 3.
Outcome and statistics
The outcome of surgery was assessed at follow-up visits 3 months after the procedure. Results were graded according to a three-tiered ranking (complete, partial, or no relief) as adopted in other series10,17,18,23,26). Complete relief was defined as complete resolution of the chief complaints. Partial relief was defined as partial resolution of the symptoms or complete resolution of some symptoms with persistence of others. No relief was defined as no change or worsening in the symptoms. Patients not achieving complete relief were scheduled for follow-up visits at an interval of 3-months for further assessment. A chi-square test was used to assess the relationship between obesity, sex and outcome. Unless noted, results are presented as (mean±standard deviation). Significant values represented p≤0.05.
Go to :
RESULTS
Demographics
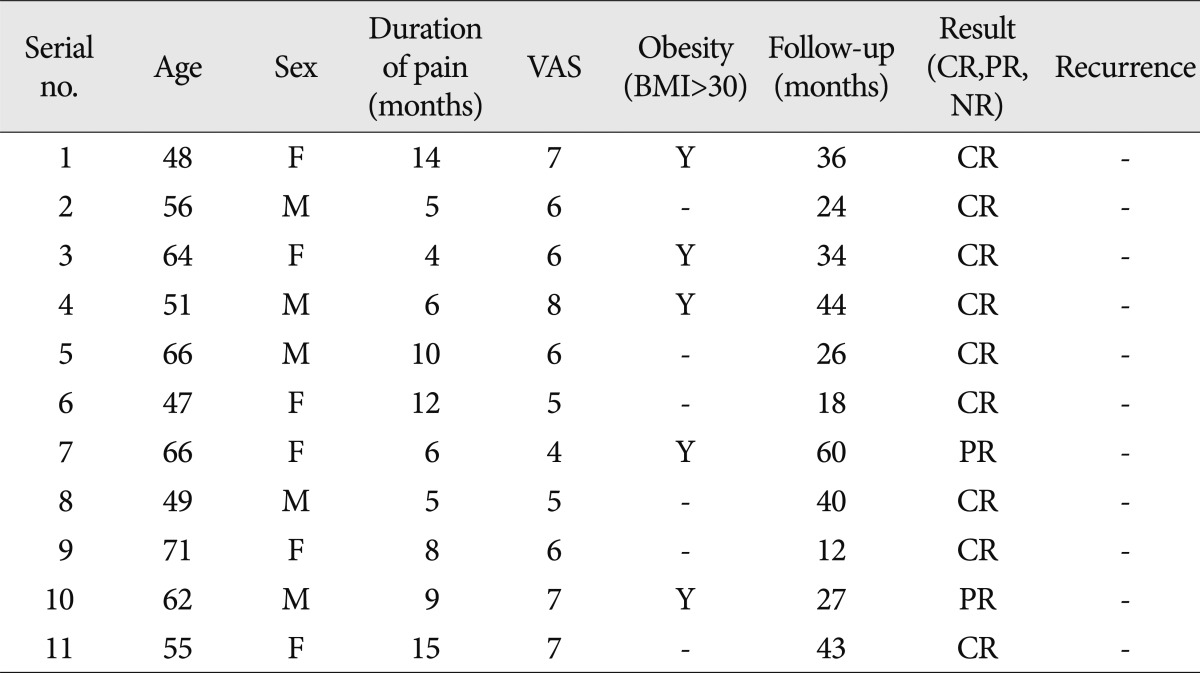
Table 1 summarizes the demographics and outcome of neurolysis in our series. The mean age of the patients was 57.7±8.4 years. Five of the 11 patients were male. The mean duration of pain before operation was 8.5±3.8 months, and mean preoperative visual analogue scale (VAS) was 6.1±1.1. The mean duration of follow-up was 33 months (range, 12-60 months).
Outcome
Nine of the 11 patients (81.8%) treated by neurolysis had complete relief of symptoms and two patients (18.2%) had partial relief in the long-term follow-up. Even the patients with partial relief were capable of independent management with intermittent medication involving NSAIDs. Repeated blocks of the LFCN were not needed in patients with partial relief. There was no complication related to surgery. There was no correlation between gender and obesity with surgical outcome (p=0.182 and p=0.887, respectively). There was no significant difference in age, duration of symptoms and preoperative VAS between patients with complete relief and partial relief (p=0.266, p=0.690, and p=0.445, respectively).
Go to :
DISCUSSION
The syndrome involving a burning, tingling, and numb sensation in the anterolateral area of the thigh, with variable reduction of sensation in the distribution of the lateral femoral cutaneous nerve, was first described by Bernhardt4) in 1895 and named meralgia paresthetica (MP; derived from the Greek word meros meaning thigh and algos, meaning pain) by Roth20) in the same year. MP has at least 80 etiologies and can be categorized as spontaneous or iatrogenic1,5,7,9,12,13). Spontaneous causes include mechanical factors such as obesity, pregnancy, and other conditions associated with increased intraabdominal pressure28). The wearing of belts, corsets, and tight trousers can also result in direct pressure on the LFCN6), and pelvic benign masses such as uterine fibrinoids as presenting as MP have been reported24,25). Other causes of spontaneous MP include radiologically degenerative pubis symphysis, limb length discrepancy, and osteoid sarcoma in more than one-third of pediatric patients following treatment13).
In the classic form of MP, the symptoms are fairly stereotypical and the diagnosis should be fairly straightforward for the astute clinician9,19). However, diagnosis of MP is not always straightforward in clinical practice19). This condition can be confused with, and in a small group of patients it can coexit with, lumbosacral radicular pain11,19,23). In our cases, the diagnosis of MP was fairly delayed and was not diagnosed until interviews conducted in our outpatient clinic. We speculate that this delay in diagnosis of MP in our country may have been related to poor understanding of this entity by some of the attending primary physicians and orthopedic and neurosurgical professionals. When there is doubt about the diagnosis following history-taking and physical examination, electrodiagnostic testing can be used. Side-to-side amplitude difference of the SNAP of the LFCN is a more sensitive predictor of MP than the absolute amplitude of the SNAP. In fact, a side-to-side amplitude ratio exceeding 2.3 combined with a SNAP <3 microvolts yields a specificity >of 98 %21).
In patients where a clinical diagnosis of MP has been made, a diagnostic block may be made with 8 mL of 0.25% bupivacaine7,22). All patients who underwent neurolysis in our series responded temporarily with repeated blocks of LFCN, and we performed differential blockade of LFCN at least three times before making a decision to decompress the LFCN.
Surgical techniques for MP include neurolysis of the constricting tissue, neurolysis and transposition of the LFCN, and transection with excision of a portion of the LFCN. Each has its own advantage and disadvantages. Neurolysis is a physiologic procedure that seeks to preserve the integrity of the LFCN. However, reported results of neurolysis vary from 60% to 95% due to presence of neuroma and anatomical variations in the course of the LFCN3,16,17,23). Only two reports have described neurolysis combined with transposition2,14) and this approach has not been tested in a clinical trial12). Transection is another effective means to produce good results28). However, sectioning of the LFCN can produce a permanent anesthetic area in the anterolateral thigh and there is a risk of neuroma formation.
Regarding neurolysis for MP, conflicting results with failure rates as high as 40% and success rates of 90% to 95% have been reported3,17,18,23,27). Why surgery works for entrapment of other peripheral nerves such as the median and ulnar nerve, but may not work for LFCN is unresolving and intriguing. This dichotomy may be due to the difficulty in establishing a correct diagnosis of MP17), inability to locate LFCN due to its anatomical variability3), and inadequate decompression2). In this regard, several measures have been advocated23). Because the presentation of MP can be confused with other conditions, such as facet joint syndrome and trochanteric bursitis, electrodiagnostic studies and diagnostic block of LFCN should be performed for confirmation of diagnosis. The high variability of the location of LFCN needs to be particularly borne in mind during nerve exploration. Complete neurolysis of LFCN should be ensured with proximal and distal extension of decompressive maneuvers. In particular, the iliac fascia is to be divided when appropriate tension bands are often noted in compressing the nerve in its pelvic course. In addition, a sling of fascia posterior to the nerve in the region of inguinal ligament has been sought23).
Siu and Chadran23) reported the biggest series of neurolysis (45 cases) in MP surgery. In their 45 neurolysis procedures, 42 cases with follow-up of 4.1 years displayed complete and partial symptom improvements were noted in 33 (73%) and nine (20%) cases, respectively. No recurrence was noted. Analysis of clinical variables demonstrated that the duration of symptoms preoperatively did not affect the rate of complete symptom relief, but obese patients (body mass index >30) was six-times more likely to have incomplete surgery at the long-term follow-up.
The presence of a neuroma and the frequency of anatomical variation in the course of LFCN may render neurolysis difficult. Therefore, transection of the LFCN is another effective means of treating refractory MP. Williams and Trzil28) reported excellent relief in 23 of 24 cases of transection. They stressed that sectioning of the LFCN offers uniformly good results and should be easily reproducible once adequate identification of the nerve is accomplished, and patients are willing to accept permanent anesthesia on an area of the anterolateral thigh in exchange for relief of their symptoms. Ivins14), in another series of 14 adult patients with a follow-up over 3-6 years, reported the effectiveness of transection in case of recurrence of MP after initial relief by neurolysis. With these favorable results of transection, they advocated primary transection in adult patients experiencing symptoms for more than 1 year and patients who have persistent or recurrent symptoms. van Eerton et al.26) evaluated transection and neurolysis in 21 refractory MP patients and found that transection (complete relief of symptoms in nine of 12 patients) was superior to neurolysis (complete relief of symptoms in three of 10 patients).
In our series, neurolysis was effective in relieving medically refractory MP. Neurolysis provided complete relief in nine patients (81.8%) and partial relief (18.2%) in two patients. There was no failure and recurrence in our series. Although previous authors stressed the relationship between obesity and recurrence of symptom, we could not find any correlation. With limited numbers of our series we cannot explain this finding. Since most papers dealing with surgeries for MP involved studies with Caucasians, a racial difference might be the reason. In a Korean report dealing with the surgical result of MP16), the authors investigated the effectiveness of surgery in nine cases of neurolysis and two cases of transaction in iatrogenic MP caused by iliac bone graft harvesting for spinal surgery. Even in iatrogenic MP, transection and neurolysis was effective in relieving painful symptoms of MP in 10 out of 11 patients16). Among the nine cases of neurolysis, complete relief was achieved in three patients, and partial relief was accomplished in four patients. Our results with neurolysis seems superior to this report, however, there was a difference in the characteristics of the enrolled patients. Our study deals MP patients with spontaneous cause, whereas the earliest study15) dealt with iatrogenic MP following surgery. However, even in iatrogenic MP following surgery, it seems that neurolysis could bring adequate relief of symptoms of MP.
Go to :
CONCLUSION
Neurolysis can be an effective means of treating medically refractory MP. To achieve a good outcome in neurolysis for MP, an accurate diagnosis with careful examination and repeated blocks of the LFCN, along with electrodiagnosis is essential. Possible variation in the course of the LFCN and thorough decompression along the course of the LFCN should be kept in mind in planning the decompression surgery for MP.
Go to :
 XML Download
XML Download