

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pedicle screw instrumentation in the lumbar spine has become popular because rigid fixation is achieved quickly, providing for early patient mobilization after surgery. Modern fusion techniques, including the use of pedicle screws, structural interbody grafts and biologics, have resulted in significant improvements in radiographic evident segmental fusion; however, this has not translated into comparable improvements in successful clinical outcomes after lumbar fusion surgery4,21). Beside this, rigid fusion causes the chronic back pain associated with back muscle atrophy and limitation of motion. Additionally, the accelerated degeneration of spinal motion segments adjacent to rigidly fused segment(s) has become increasingly recognized as a drawback of spinal fusion procedures5,7,14,18). Fixed sagittal imbalance, flat-back syndrome, and pseudoarthrosis are also potential complications associated with rigid fusion of the lumbar spine9).
Based on studies in which patients with partial fusion showed the same clinical outcomes as patients with solid fusion, it might be hypothesized that a reduction in, rather than an elimination of, segmental motion results in the alleviation of pain2,5,12,17). These findings suggest the need for alterative procedures and techniques that do not require fusion for the treatment of painful degenerative spine disease. Therefore, various kinds of dynamic stabilization systems have designed to stabilize the segment while preserving motion and unloading the disc and facet joint3,15).
The NFlex controlled stabilization system is a novel pedicle based dynamic stabilization that incorporates the insertional techniques of traditional pedicle screw fixation devices, while potentially providing the segmental stabilization with preservation of some motion at stabilized segments.
In an earlier clinical study using the NFlex device, it was proved as clinically effective with few complications during a short-term follow-up1). In this study we describe the extended two-year clinical experience with the NFlex controlled stabilization system focusing on the clinical outcomes and complications.
MATERIALS AND METHODS
Device description
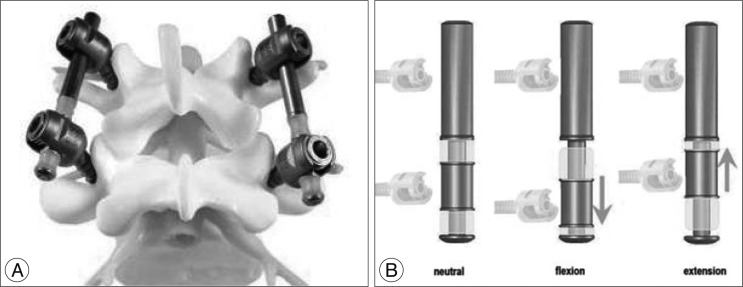
The NFlex controlled stabilization system (Synthes Spine Inc., West Chester, PA, USA) consists of polyaxial titanium alloy pedicle screws that are fixed to a semi-rigid polycarbonate urethane-sleeved rod. The integrated polycarbonate urethane (PCU) spacer is surrounded by a central titanium ring, to which a pedicle screw is locked. The controlled pistoning of this spacer along the axis of the central titanium core provides a shock absorber effect, reducing the overall rigidity of the construct.
The rods are low profile, may be used in single- or multi-level applications, and require a relatively short distance between screws of only 9 mm. The rod may be attached to pedicle screws in the standard fashion, with one pedicle screw attached to the titanium ring of the sleeve and one or more pedicle screws attached to the solid portion of the titanium rod (Fig. 1)28).
In the unaltered lumbar spine, flexion is necessarily coupled with elongation and extension is coupled with compression of the posterior segments; therefore, any device hoping to provide support through physiologic translational motion (flexion-extension) would be required to elongate and compress as well (Fig. 2). Thus it was designed to accommodate this physiologic motion via a bumper element. The PCU spacer (bumper elements) is not bonded to the titanium components of the rod. Therefore, when the distance between the pedicles (DBP) increases and decreases during the translational movement (flexion and extension), the rod is able to elongate and compress to accommodate this change, as well as toggle to accommodate angulation. Compressive loads are borne primarily by the spacer, as opposed to the titanium core. The titanium core provides resistance to translation of one vertebra relative to the adjacent vertebra. Biomechanical study of this device demonstrated that in all loading modes, the N-Flex device provided a decompressed lumbar segment with sufficient stability (i.e., greater than the intact case) but significantly less rigid than a similar segment stabilized with a solid rod, suggesting the applicability of this implant as a dynamic fixation device in clinical practice6,28).
Patient population & clinical application
Five institutes participated in a retrospective assessment of 72 consecutive patients who underwent NFlex controlled stabilization between September 2006 and July 2007, at one level with or without rigid fusion at a contiguous level. Of these 72 patients, 65 were available for 2-year follow-up. The study group consisted of 26 men and 39 women with an average age of 54.5 years (range 19-86).
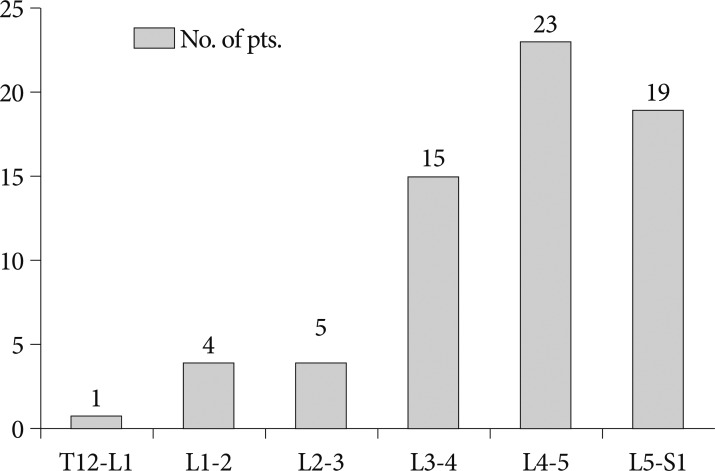
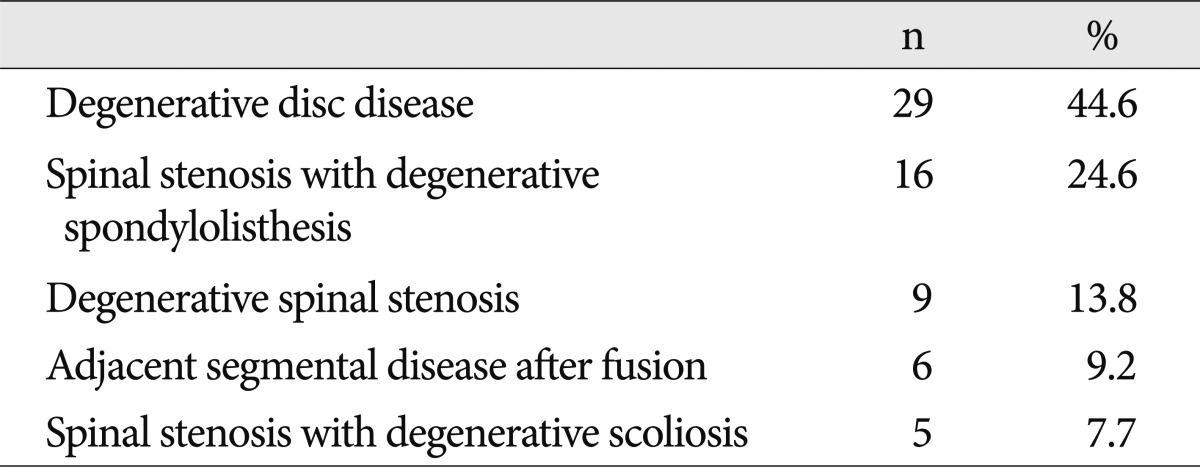
The NFlex controlled stabilization system was applied for a non-fusion stabilization, or hybrid fusion, which is one or more segment fusion with one segment non-fusion stabilization at an adjacent segment. The non-fusion stabilization was used for patients with degenerative disc disease (DDD), spinal stenosis with instability (single or multi-level), degenerative spondylolisthesis (Grade 1), adjacent segments diseases, and multi-level degenerative stenosis with scoliosis. Hybrid fusion was applied for single or multi-level fusion indicated patients with substantial pathologies at an adjacent level, but not enough to warrant fusion. Patients with profound osteoporosis (T-score <-2.5), isthmic spondylolisthesis, bilateral spondylolysis, bilateral facetectomy or insufficiency, fracture, infection, and metastatic spine tumors were not indicated. In this study group, device was applied for DDD in 29 patients (44.6%), spinal stenosis with degenerative spondylolisthesis in 16 patients (24.6%), degenerative spinal stenosis in 9 patients (13.8%), adjacent segment disease (ASD) after fusion in 6 patients (9.2%), and spinal stenosis with degenerative lumbar scoliosis in 5 patients (7.7%) (Table 1). Nine patients had prior lumbar surgeries, including 2 discectomies, and 6 lumbar fusion procedures. Non-fusion application was done in 25 patients and hybrid fusion was done in 40 patients.
Surgical procedure
The NFlex controlled stabilization was implanted using standard surgical procedures for standard posterior lumbar spinal surgery. Standard midline incisions and subperiosteal retraction of the paraspinal muscles exposing the affected segment was used in most cases. It some cases, however, bilateral paraspinal (Wiltse) approach were used in order to minimize muscle disruption. If indicated, decompression of the spinal canal was performed first. Insertion of the pedicle screws was performed under radiographic control using an intraoperative fluoroscopy. It is important not to interfere with facet joint. The entry point of pedicle screw must be located at the external junction of the facet joint and transverse process. Care was taken to place the screws lateral to the facet joints, at 30-45° lateromedial angle and parallel to the upper end plate of the corresponding vertebrae.
A special bender is used to contour the rod. This instrument allows bending within a few mm of the dynamic section of the rod, while protecting this area from being contoured and potentially damaged. Contoured dynamic rods were connected to pedicle screws with usual fashion.
Preoperative assessment
All patients underwent a complete preoperative history and physical examination. Preoperative imaging studies included anteroposterior (AP) and lateral static plain radiographs, as well as dynamic flexion/extension X-rays. Lumbar computed tomography (CT) and magnetic resonance imaging (MRI) was also performed in most cases. Patients completed Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) questionnaires at pre- and postoperative evaluations.
Clinical evaluation
The patients generally returned for follow-up evaluations at 3 and 6 weeks (one center assessed patients at 4 weeks), 3 months, 6 months, 12 and 24 months. In some cases, follow-up evaluations were conducted through phone interviews. A thorough neurologic examination was performed pre-operatively and at most post-operative points, as were static and dynamic lumbar plain films to evaluate for implant integrity. VAS and ODI scores were routinely collected.
RESULTS
Perioperative data
The levels treated with dynamic stabilization are presented in Fig. 3. All patients were treated with a construct that provided a single dynamic level (non-fusion). Two patients underwent two single-level dynamic constructs at non-contiguous levels (L3-4 and L5-S1). Instrumented rigid fusion was performed at contiguous levels in 40 patients (the so called "hybrid fusion"), placed either cephalad or caudal to non-fusion stabilized segment. Twenty-five patients received non-fusion dynamic stabilization only without fusion segments. Twenty-eight patients received a single-level rigid fusion combined with one level dynamic stabilization. Eight patients received a two-level rigid fusion combined with one level dynamic stabilization, and 4 patients received a 3-level rigid fusion, plus one level dynamic stabilization. Dynamic stabilization was used at the contiguous superior level in 33 (82%) of patients receiving the "hybrid" fusion, and was placed at the inferior end of the fused segment(s) in 7 (18%) of patients receiving the hybrid fusion. The most common pathology was for DDD at 1 or 2 levels.
Clinical outcome
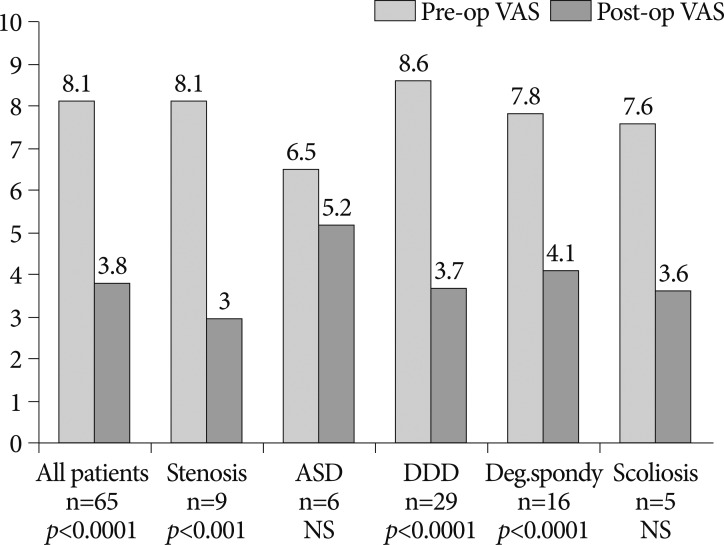
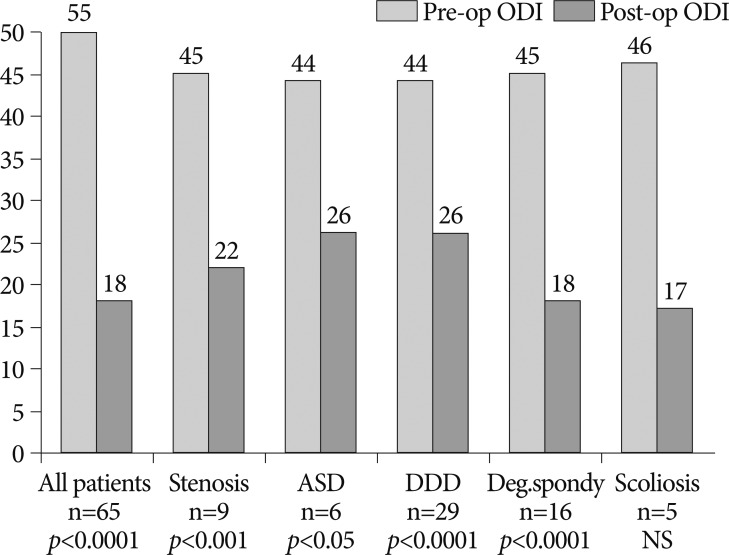
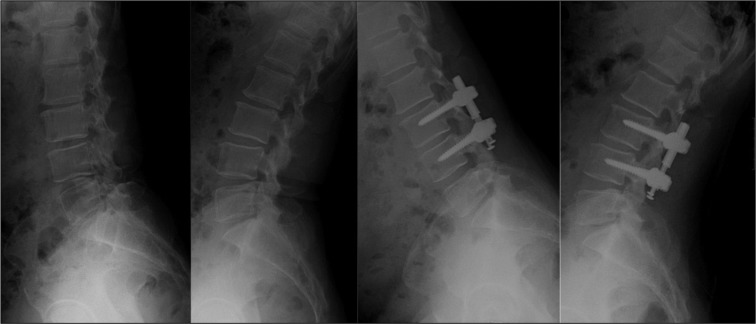
The mean follow-up period was 25.6 months (range 23-34 months). The mean VAS score improved from 8.1 preoperatively to 3.8 postoperatively (p<0.001), representing a 53% improvement. There was a statistically significant improvement in VAS across all indications, with the exception of pain scores in patients with prior fusions treated for ASD and degenerative lumbar scoliosis. There was a favorable trend in these subgroups, however, as the ASD patients had a mean improvement of 20% and the scoliosis patients had a mean improvement of 53% Functional status also showed significant improvement, with a mean pre-operative ODI score of 44.5 improving to 21.8 (p<0.001) postoperatively, representing a 51% improvement. The level of ODI improvement was similar across all indications and statistically significant with the exception of patients with scoliosis. Although the 5 patients with scoliosis showed a favorable trend with a mean improvement in ODI of 62%, statistical significance was not achieved. These results may have been affected by the small number of patients in the ASD and scoliosis subgroups. In addition, patients with severe disability or worse (ODI 41 or greater) at follow-up comprised only 8% of the total, whereas 69% of the total had severe disability pre-operatively. Improvements in pain (VAS) after surgery are presented in Fig. 4 and improvements in functional status (ODI) are presented in Fig. 5. The case illustrations were shown in Fig. 6 and 7.
Complications
There were no significant intra- or perioperative complications related to the device. Three patients were noted to have device related complications postoperatively, however. There was one case with a rod fracture. This occurred in a 280 lb. male that had a prior 3 level fusion from L3-S1, that was topped off at L2-3. The rod fracture was discovered at 1-year follow-up. The patient was not symptomatic. One patient underwent a re-operation for a loose locking cap on the pedicle screw. Of the 372 screws implanted, one was observed to have loosening. This patient was treated with a dynamic level at L1-L2, but no pedicle screws could be placed in L2. Consequently, the dynamic segment spanned L1-L3. These circumstances likely created an unusually long lever arm, likely causing the screw to loosen. Non-device related complications included : one re-operation due to advanced osteoporosis, cage migration at a non-dynamic (fusion) level; device removal due to infection in a patient with lupus; one patient requiring adjacent level surgery; and one patient who succumbed from causes not related to spinal disease or surgery. It should be noted that all symptomatic patients were evaluated for the presence of implant-related complications.
DISCUSSION
Still the fusion is the gold standard of surgical management in lumbar degenerative disc diseases8). But many reports have been documented inevitable side effects of the fusion such as chronic back pain, and adjacent segment degeneration9). To overcome these undesirable effects, motion preservation technologies such as total disc replacement and posterior dynamic stabilization system have been introduced. Non-fusion posterior dynamic stabilization systems have gained popularity recently. It is hypothesized that abnormal load transmission across a degenerated spinal motion segment leads to abnormal segmental motion, altered biomechanics and, subsequently, pain19,25). When used in a non-fusion application, the goal of dynamic stabilization is to control, rather than eliminate, segmental spinal motion in order to reduce abnormal load transmission across an intervertebral disc and/or facet joint, while avoiding the drawbacks associated with rigid fusion. This is accomplished by limiting segmental motion to a range close to normal and/or by preventing the spine from adopting positions or postures that lead to abnormal load transmission. Limiting segmental motion may also be useful to control motion in the iatrogenically destabilized spine; to increase anterior load sharing to augment interbody fusion; and to provide less rigid stabilization in the aging spine3,15). Additional goals of dynamic stabilization are to cause minimal disruption and to preserve future surgical options.
Of several dynamic stabilization devices, especially pedicle based dynamic stabilization system (PBDS) has the property of intrinsic dynamic nature contrary to other static devices such as interspinous spacer. Subsequent clinical trials in the treatment of degenerative lumbar diseases using pedicle-based dynamic stabilization system were made. Many of them reported successful outcome16,20,24,27,29). One of the most extensively-used posterior dynamic stabilization systems is the Dynesys® dynamic stabilization system (Zimmer Spine), in which pedicle screws are connected across spinal motion segments with non-elastic bands to provide controlled motion. Early clinical outcomes have shown dynamic stabilization using this system to be effective in lessening pain and disability at in patients with degenerative spondylolisthesis and central or lateral canal stenosis. Other pedicle-based dynamic stabilization systems have developed and reported their clinical outcomes13,22,26). But clinical outcomes were disputed despite theoretical advantages over the rigid fusion11,23). One of reasons for discrepancies between theoretical advantage and clinical outcomes is due to design flaw in PBDS. The ideal PBDS should simulate the normal functional spinal unit, which has normal kinematics, normal load transfer pattern with load sharing, and active change of center of rotation. Beside these, normal spine has a unique pattern of motion on sagittal plane as well as coronal and axial plane. The distance between upper and lower pedicle (DBP) is changing during the flexion-extension. Thus, PBDSs can be compatible to this change of DBP. Most PBDSs in current market designed to have fixed DBP during translational movement when it is implanted. This design flaw can contribute to abnormal kinematics, abnormal loading, metallic failure and unwanted clinical outcome.
NFlex is the first PBDS with the compatibility for DBP changing. This device consists of polyaxial titanium pedicle screws that are fixed to a semi-rigid polycarbonate urethane-sleeved rod. The integrated PCU spacer is surrounded by a central titanium ring, to which a pedicle screw is locked. The PCU spacer is not bonded to the titanium components of the rod. Therefore, when the DBP changing during translation, the rod is able to elongate and compress to accommodate this change, as well as toggle to accommodate angulations. Compressive loads are borne primarily by the spacer, as opposed to the titanium core. The controlled pistoning of this spacer along the axis of the central titanium core provides translational motion, and a shock absorber effect, reducing the overall rigidity of the construct28). Earlier clinical and radiographic studies using this device revealed compatible outcomes from the traditional treatment and preserved the limited extent of ROM at the stabilized segment1). Although Dynesys system is currently widely used, it is troublesome and complicated in the procedure of inserting of polycarbonate urethane spacer and polyester cord of Dynesys to pedicle screw. NFlex controlled stabilization system has same diameter rod at both ends like usual rod. This dynamic rod is a semi-rigid polycarbonate urethane-sleeved and it can be fixed usual polyaxial titanium alloy pedicle screws. Though this surgical procedure is exactly same to traditional pedicle screw fixation, it is easy to insert the dynamic rod. The NFlex dynamic rod was tested for static and fatigue durability according to the American Society for Testing Materials specification number F1717 out to 10 million cycles. And the result was shown a higher level of strength than several commercially available rigid pedicle screw systems.
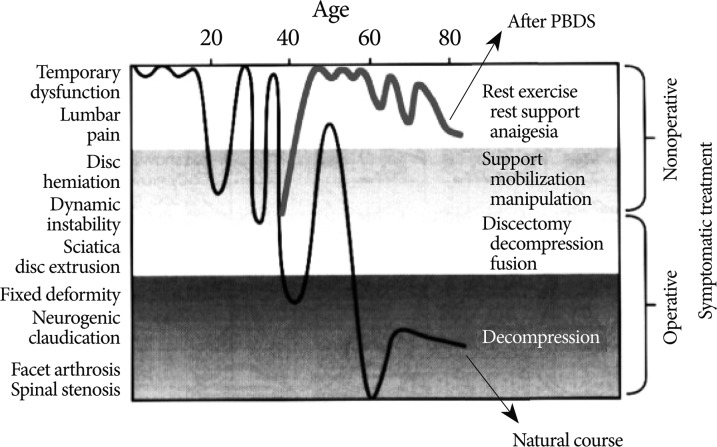
Mullholland et al.19) stated that a dynamic stabilization is a system that would alter movements favorably and load transmissions of a spinal motion segment, without the intension of fusion of the segment. This leaves the spinal segment mobile, its intention is to alter load-bearing patterns of the motion segment and to control any abnormal motions at the segment. Actually, the dynamic stabilization system was named as an instrumentation that permits axial loading to promote the fusion. Still this term is in use as that meaning. Thus use of this term would not be suitable for the system that alters the load-bearing pattern and control motion. Furthermore, current PBDS has no dynamic nature, it just limits the ROM with a limited amount of load sharing, which means that it does not reflect the dynamic nature of functional spinal segments. Galbusera et al.10) stated that "dynamic" may be a misleading word from an engineering point of view, since it suggests a time or velocity dependency which does not exist. For this reason, the authors prefer the term "controlled stabilization" in stead of "dynamic stabilization." Another disputable point is the definition for the dynamic stabilization. Actually, the definition by Mullholland and Sengupta was made on the basis of chronic back pain in DDD. However, current applications for the dynamic stabilization are quite diverse. In fact, non-DDD applications (such as spinal stenosis, spondylolisthesis, and recurrent disc herniation) were more common in the literature. In this viewpoint, the definition of the dynamic stabilization system in non-DDD applications should be different from that in DDD applications. In such cases, the spine was decompressed and then the dynamic stabilization was added for the enforcement of the weakened spine by decompression. In this situation, the dynamic stabilization is a supportive device that can strengthen the decompressed spine. Therefore, the basic concept of the dynamic stabilization in degenerative spinal disease is an "internal brace" that can add the stability to a weakened decompressed spine. By stabilizing the decompressed spine, a dynamic stabilization can help prevent or delay further degeneration of the spine with controlled motion. Thus, the dynamic stabilization system would be defined as a system that would stabilize the decompressed (weakened) spinal motion segment without fusion and control some range of motion, and lead to a new degenerative process (Fig. 8).
In an earlier clinical study using NFlex stabilization system1), authors have found that the NFlex dynamic stabilization system, when used as a nonfusion dynamic stabilization system, provides improvements in pain and function scores compared to those found in use of the Dynesys system, although the follow-up is much shorter (average 8.1 months). In addition, the preliminary data compared favorably to the ODI scores of the posterolateral fusion group in a randomized prospective clinical trial, as the percentage of NFlex patients with severe disability was only 13% (compared to 47% in the posterolateral fusion group). Finally, from the small number of patients that have been measured, 53% have demonstrated partial preservation of normal ROM. Furthermore, there have been no rod-related adverse events and the option of later converting a dynamically stabilized segment to a fusion is preserved.
In the present study, the authors presented the clinical outcomes in 65 patients who underwent NFlex controlled stabilization. As like the earlier clinical study1), the NFlex system has proven effective in improving pain and function scores after two years. We observed one case of rod failure in this series; however, this failure was identified in March 2008, 1 year post-operatively. The rod manufacturer engaged the authors in an analysis of this event, along with a small number of similar events, to more clearly identify relevant patient pathology and intraoperative considerations. This thorough, proactive approach led to more detailed patient selection and surgical technique guidance. Importantly, preloading the dynamic end of the rod could compromise the dynamic portion of the titanium ring and polymer sleeve construct, and overload the titanium core. Both patient pathology and intraoperative technique can contribute to preloading. Specifically, certain patient pathologies, such as sagittal or coronal deformity, spondylolisthesis, facet insufficiency or hypermobility may contribute to excessive loading, and should be avoided at the dynamic level. The segment intended for stabilization must provide enough stability to load share with the rod. Intraoperatively, patient positioning in neutral spinal alignment should be maintained throughout the procedure. Manipulating the dynamic end of the rod by persuasion, or applying compression or distraction, will preload the rod, and should be avoided.
This study focused only on the clinical outcomes after the application of the NFlex controlled stabilization system. Unfortunately, detailed radiographic results including ROM after operation, the overall rate of screw loosening, and preventing effects of adjacent segment degeneration were not studied. Overall clinical outcomes of this study were comparable to traditional treatments. However, the clinically relevant benefits of a less rigid segment are yet to be seen. Over time, sustained clinical improvement, and absence of implant related complications or re-operations will be important and perhaps differentiating factors in support of these devices. Long term level I evidence will not be available for many years, so the rationale for utilizing dynamic stabilization will continue to be based on the belief in a theoretical benefit from controlling, rather than completely eliminating motion, supported with biomechanical data and the ongoing compilation of level III evidence.
CONCLUSION
Pedicle-based dynamic stabilization using the NFlex controlled stabilization system seems effective in improving pain and function scores, with sustained clinical improvement after two years. The incidence of adverse events and re-operation was not inconsistent with the authors' experience with rigid fusion. With appropriate patient selection and surgical implantation, dynamic stabilization may be considered an effective alternative to rigid fusion based on medium term follow-up.


 XML Download
XML Download