

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since its introduction, hypoglossal-facial nerve anastomosis (HFNA) has been used as a favorable option for injured facial nerve (FN) reanimation. However, this operation results in donor nerve deficits, such as hemiglossal atrophy. Several modified surgical techniques, including anastomosis from the split hypoglossal nerve (HGN) or descending branch of the HGN to the FN, have been designed to reduce hemiglossal atrophy. Moreover, other modifications have also been made, such as hemihypoglossal-facial anastomosis and hypoglossal-facial nerve interpositional jump graft to overcome complications caused by classical methods6,8,18,22).
First, a detailed understanding of the anatomy of the submandibular region, including the route of the HGN and useful anatomical landmarks for HFNA and surrounding structures, is important to reduce procedural complications and the risk of nerve damage. It is difficult to define the proximal part of the HGN located immediately beneath the base of the skull, as the HGN in this area is readily confused with accessory nerves or the vagus nerve. Thus, it is necessary to dissect the submandibular region for identification of the HGN. Several anatomical studies of the submandibular region have been reported3,16,17,23), but there have been no previous reports of such studies in Korean subjects. This study focused mainly on the relationships among the FN, HGN, and surgical landmarks such as the mastoid process tip (MPT), the digastric muscle posterior belly (DMPB), and the common carotid artery (CCA), which can be easily identified during surgery. The anatomical data on the relationships between the anatomical landmarks, FN, and HGN may be helpful to find the FN and HGN more easily and to reduce the risk of procedural complications.
MATERIALS AND METHODS
Fifteen adult cadavers (9 males and 6 females) with a mean age of 62.2 years (range : 48-81) were fixed with formalin solution. A total of 29 specimens were obtained from 15 cadavers. Due to the anatomical destruction of the left submandibular region in one male cadaver (No. 15), the left specimen of this cadaver was excluded.
First, suboccipital and neck muscles were removed carefully, and the FN, digastric muscle, carotid artery, and nerve trunks were exposed. The mastoid process was dissected, and the FN was identified. After identification of the FN beneath the mastoid process, the FN was further dissected in the direction of the stylomastoid foramen (SMF). The SMF was located in the dorsal portion of the styloid process, which was the exit point of the FN. Subsequently, the FN was dissected and traced distally to the posterior part of the parotid gland. The parotid gland was removed almost completely for FN dissection.
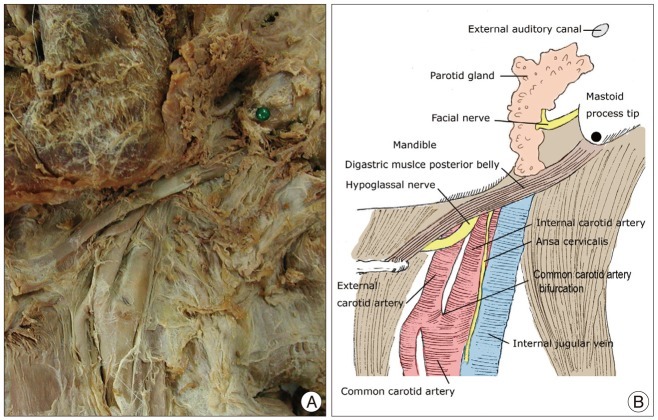
To determine the relationships among the FN, HGN, and surrounding structures, the MPT, the bifurcation of CCA, and the DMPB were designated as the anatomical landmarks of the submandibular area (Fig. 1).
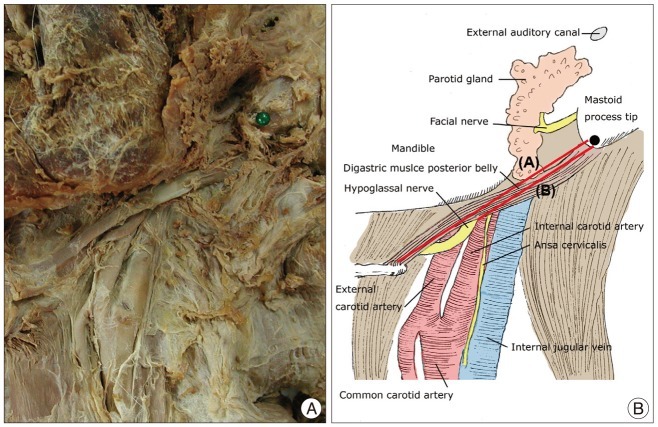
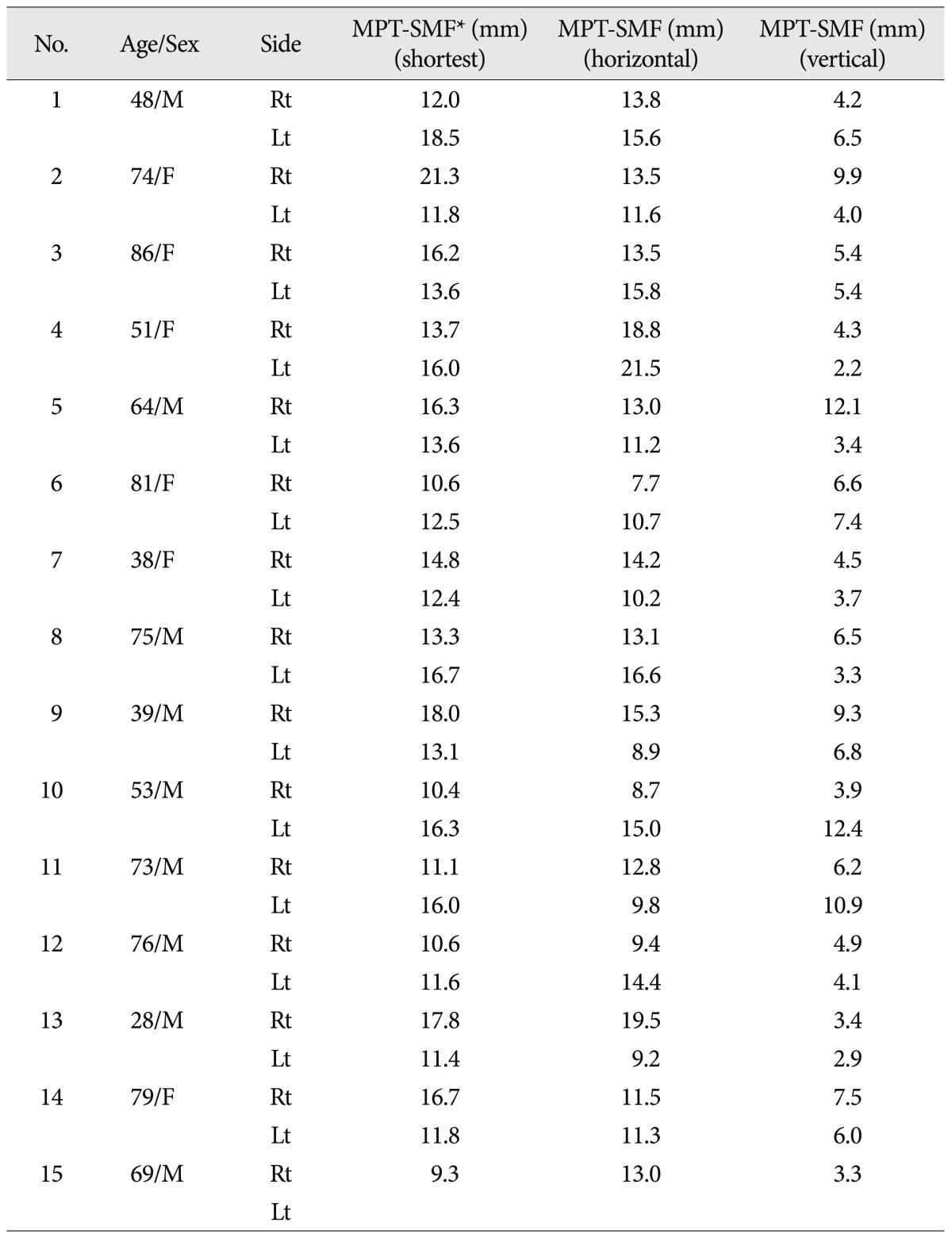
Based on the MPT, the following measurements were obtained : 1) the shortest distance to the SMF, which was the exit point of the FN; 2) the horizontal distance to the SMF; and 3) the vertical distance to the SMF (Fig. 2).
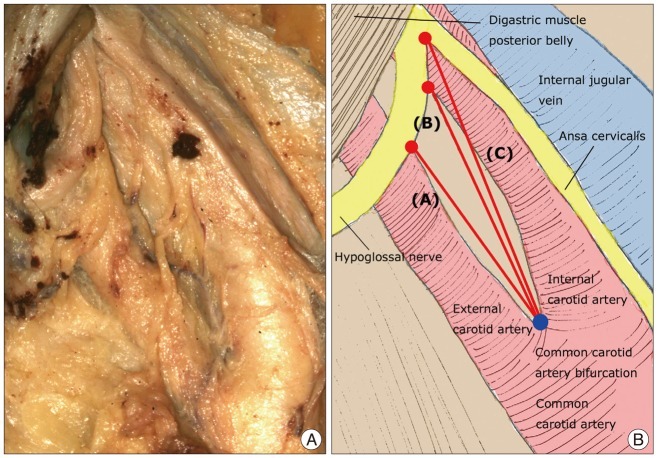
Based on the DMPB, the following measurements were obtained : 1) the whole length of the DMPB running from the digastric groove (DMPB origin) to the fibrous loop for the intermediate digastric tendon; and 2) the distance from the DMPB origin to the crossover point between the DMPB and the HGN (Fig. 3). The following measurements were also obtained based on the common carotid artery bifurcation (CCAB) : 1) the distance from the CCAB to the crossover point between the HGN and the ventral margin of the internal carotid artery (ICA); 2) the distance from the CCAB to the crossover point between the HGN and the dorsal margin of the external carotid artery (ECA); and 3) the distance from the CCAB to the HGN bifurcation (Fig. 4).
A standard meter and goniometer were used to obtain measurements, and all measurements were made by one trained physician to minimize interobserver measurement errors. The data were used in a comparative analysis of sex and right/left differences. The data are presented as means±standard deviations for continuous variables and frequency (percentages) for categorical variables. Statistical analyses were performed using SPSS for Windows version 14.0 (SPSS, Inc., Chicago, IL, USA). Differences between groups were compared with Student's t-test for continuous variables. In all analyses, p<0.05 was taken to indicate statistical significance.
RESULTS
Gross anatomical structure of the submandibular area
The origin of the DMPB, the digastric groove, was found in the ventral portion of the mastoid process after removal of the sternocleidomastoid muscle. The location and depth of the FN trunk, located in the posterior portion of the parotid gland, were variable. The FN trunk was usually located in the ventral portion of the MPT, but was found in the caudal portion of the MPT in some cases. If small FN branches were found initially in dissection of the posterior part of the parotid gland, pursuit of the course of the small FN branch proximally would be a good guideline to find the main FN trunk. Dissection of the FN proximally in the posterior parotid gland exposed the distal FN trunk and pes anserinus, which was the ramification point of the FN trunk in the parotid gland.
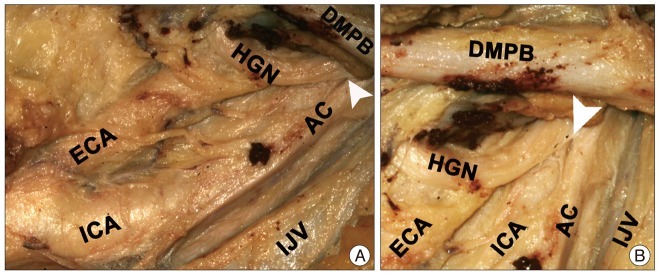
The HGN was located under the internal jugular vein (IJV) and was seen after the IJV was retracted posteriorly. The HGN was between the dorsal part of the ICA and the ventral part of the IJV. The HGN ran parallel with the accessory nerve and the vagus nerve in the high cervical area, which was confusing. The HGN branched off under the DMPB, making a new branch called the ansa cervicalis, and crossed a branch of the ICA (Fig. 5).
Distance between the MPT and the SMF
Table 1 shows the measurements based on the MPT. Table 2 and 3 shows the results corresponding to sex and to each side, respectively.
Shortest distance from the MPT to the SMF
The shortest distance between the MPT and the SMF was 14.1±2.90 mm. The shortest distance in males was 13.83±2.93 mm, and that in females was 14.28±2.94 mm. This difference between males and females was not statistically significant (p=0.684). The difference between the shortest distance on the right side (14.14±3.51 mm) and that on the left side (13.95±2.30 mm) was not statistically significant (p=0.866).
Horizontal distance from the MPT to the SMF
The horizontal distance from the MPT to the SMF was 13.6±2.8 mm. There was no significant difference (p=0.719) between the horizontal distance in males (12.9±3.06 mm) and that in females (13.36±3.84 mm). The horizontal distance on the right side was 13.19±3.22 mm, and that on the left side was 12.99±3.60 mm. This difference was not statistically significant (p=0.875).
Vertical distance from the MPT to the SMF
The vertical distance from MPT to SMF was 5.8±2.8 mm. The vertical distance in males was 6.51±3.50 mm, and that in females was 5.58±2.07 mm. The vertical distance on the right side was 6.13±2.60 mm, and that on the left side was 5.64±3.01 mm. The differences related to sex (p=0.416) and side (p=0.641) were not statistically significant.
According to the above measurements, the SMF was located 13.6±2.8 mm anteriorly and 5.8±2.8 mm superiorly from the MPT.
Morphometric relationship between the DMPB and the HGN
Table 4, 5, and 6 show the morphological measurements according to sex and side in the 29 specimens from 15 cadavers. The DMPB was located from the digastric groove to the fibrous loop of the intermediate digastric tendon. The whole length of the DMPB was 57.8±8.1 mm on average. The distance from the DMPB origin to the exit point of the HGN under the DMPB was 35.8±5.7 mm and corresponded to about 65.5% of the DMPB from the digastric groove.
Whole length of the DMPB
The whole length of the DMPB was 57.8±8.1 mm and was not significantly different between males and females (54.53±13.38 mm and 58.84±7.28 mm, respectively, p=0.318). The whole length of the DMPB was significantly greater on the right side than that on the left side (62.2±6.01 mm and 52.93±7.28 mm, respectively, p=0.001).
Distance from the DMPB origin to the crossing point of the DMPB caudal border and the HGN
The distance from the DMPB origin to the crossing point of the DMPB caudal border and the HGN was 35.8±5.7 mm. There was no significant difference between the distances measured in males and those in females (37.18±5.94 mm and 33.84±4.88 mm, respectively, p=0.121). The distance on the right side was 37.19±4.95 mm, and that on the left side was 34.31±6.21 mm. This difference was not statistically significant (p=0.956).
Relationship between the DMPB and the HGN
The HGN appeared under the DMPB, and the crossing point corresponded to about 65.5% of the whole length of the DMBP from the digastric groove. The whole length of the DMBP was longer in females than in males, but the difference was not statistically significant (p>0.05). However, the length was significantly greater on the right side than on the left side (p<0.05).
Morphometric relationship between the carotid artery and the HGN
The HGN crossed the ICA ventral part obliquely, and the distance from the CCAB to the crossing point was 18.5±6.7 mm. The HGN also crossed the dorsal part of the ECA, and the distance from the CCAB to this crossing point was 15.5±5.1 mm. Table 7, 8, and 9 show the distances from the CCAB to the crossing point between the ICA and the HGN, and between the ECA and the HGN according to sex and side.
Distance from the CCAB to the crossing point between the ventral portion of the ICA and the HGN
The distance from the CCAB to the crossing point between the ventral portion of the ICA and the HGN was 18.5±6.7 mm. The distance was not significantly different between males and females (19.05±5.38 mm and 17.66±8.49 mm, respectively, p=0.592). There was also no significant difference between the distances on the right and left sides (18.41±7.50 mm and 18.55±6.08 mm, respectively, p=0.956).
Distance from the CCAB to the crossover point between the dorsal portion of the ECA and the HGN
The distance from the CCAB to the crossover point between the dorsal portion of the ECA and the HGN was 15.5±5.1 mm. There was no significant difference between the distances in males and females (15.76±5.07 mm and 14.03±6.62 mm, respectively, p=0.777). There was also no significant difference between the distances on the right and left sides (15.35±6.58 mm and 14.72±4.84 mm, respectively, p=0.468).
Distance from the CCAB to the HGN bifurcation
The HGN ran caudally between the ICA and the IJV. The HGN gave rise to the ansa (HGN bifurcation) on the ICA and curved obliquely toward the ECA. The distance from the CCAB to the HGN bifurcation was 26.6±7.5 mm. The distance was 28.43±5.91 mm in males and 24.03±9.02 mm in females, and it was 27.61±8.74 mm on the right side and 25.54±6.14 mm on the left side. There were no significant differences according to sex (p=0.124) or side (p=0.468).
In this study, the location of the CCAB showed inter-individual variation, and the parameters associated with the CCAB showed a large degree of deviation. However, most HGNs were detected within the area between the DMPB and CCAB. Considering all parameters associated with the CCAB, the HGN appeared under the DMPB, and the crossing point corresponded to about 65.5% of the whole length of the DMPB from the digastric groove.
DISCUSSION
The FN appears from the SMF beside the styloid process. It lies medial, deep, and slightly anterior to the middle of the mastoid process at the lower end of the tympanomastoid fissure. After the FN ramifies the posterior auricular and branches to the posterior digastric and stylohyoid muscles, it runs obliquely inferiorly and laterally into the substance of the parotid gland. It divides into the temporofacial and cervicofacial divisions at a point vertically below the lowest part of the bony external auditory meatus (Fig. 1)7).
The HGN typically emerges between the ICA and the IJV to descend in the lateral groove between them to a point not far above the CCAB. It then gives rise to the superior root of the ansa cervicalis and curves forward across the lateral surfaces of both the internal and external carotid vessels. In this course, it usually passes downward until just lateral to the origin of the occipital artery and then turns forward, being held at the turn by the sternomastoid branch of the occipital artery so that it hooks around these vessels before it runs forward above the hyoid bone4). After turning forward, the HGN crosses the ventral portion of the ICA, the dorsal portion of the ECA, and the DMPB (Fig. 1, 2).
HFNA has been considered an effective means of reanimating the paralyzed facial nerve. However, classic HFNA involves sacrificing the normal HGN, causing hemitongue atrophy. Many modifications have been made to this technique to avoid hemitongue atrophy. May et al.14) introduced a hypoglossal-facial nerve interpositional jump graft. However, direct HFNS was more effective for restoring facial function. Cusimano and Sekhar5), Sekhar et al.20), and Arai et al.1) reported anastomosis of a split hypoglossal nerve to the facial nerve. These methods preserved hypoglossal function with mild or moderate hemiglossal atrophy. To minimize disruption of hypoglossal nerve function, hypoglossal-facial nerve side-to-end anastomosis was developed17).
HFNA remains the most commonly used technique, and many modifications have been made to achieve nerve dissection without injury. However, it is difficult to dissect the submandibular region without damaging the FN and the HGN. Several studies have shown that it is difficult to identify and expose the FN during dissection as the FN is surrounded by dense connective tissue10,21). As the FN and the HGN are located in complex areas, surgeons must be well acquainted with the anatomy to prevent procedural damage. Many authors have suggested that detailed anatomical knowledge is necessary to achieve successful anastomosis1,2,13,16). Gardner et al.9) suggested that the DMPB should first be found to identify the FN. Malone and Maisel12) cautioned that using a nerve stimulator to identify the FN may be misleading because of false negative responses. Sawamura and Abe17) used a method involving initial exposure of the MPT to search for the FN. Salame et al.16) recommended following the styloid process until the SMF emerged to identify the FN. Asaoka et al.3) reported that the FN usually appeared on the ventral portion of the MPT. Some reports suggested that landmarks may be used for safe FN dissection. Three of the above-mentioned studies used bony landmarks for FN dissection3,16,17). Two studies used the MPT, and the other used the styloid process. The MPT is a relatively large structure and is located superficially. Moreover, the MPT is not surrounded by any dangerous structures and allows the surgeon to gain a solid general understanding of the local anatomy. For these reasons, the MPT was used as a landmark in this study. Kempe11) noted previously that it is a common error to go deep to look for the nerve. Salame et al.16) introduced several parameters associated with the FN and surrounding structures. They used 23 formaldehyde-fixed adult cadavers (13 female and 10 male) aged 51 to 74 years at the time of death and dissected bilaterally (46 dissections). The distance was 17.22±3.18 mm between the SMF and the MPT. Jones19) estimated the depth from the MPT to the SMF as 2 cm. In the present study, the distance was 14.1±2.9 mm between the SMF and the MPT. Morphometric measurements in the present study were slightly shorter than those reported by Salame et al.16) because of differences in the proportion of males to females and the numbers of specimens between the two studies. However, the age spectrum was similar between the present study and that of Salame et al.16) The numerical discrepancies between these two studies may have been due to differences in proportion of males to females as well as to racial differences. It can be inferred that other parameters, such as horizontal and vertical distances between the MPT and SMF, would show numerical differences. Further investigations are required to determine the relationship between the SMF and the MPT. This FN dissection-related database will be helpful for predicting the FN exit or route prior to surgery.
HGN dissection is more complicated, as the location of the HGN is much deeper than that of the FN, and there are many variations in the HGN branching patterns. Moreover, there are no bony landmarks around the HGN. Therefore, the digastric muscle, the ICA, and the IJV were used as landmarks for HGN dissection. Martins et al.13) suggested that the HGN should be dissected at the lowest portion of the cervical incision, inferior and medial to the DMPB. Vacher and Dauge23) suggested that access to the sternocleidomastoid muscle region should be achieved initially. Rebol et al.15) reported that the HGN was located in the neck under the digastric muscle. Arai et al.1) proposed that the HGN should be exposed deeply to the plane of the digastric muscle and superficially to the carotid vessels. Asaoka et al.2,3) suggested that the HGN could be found by retracting the IJV posteriorly. In the extreme-high cervical area, the HGN runs parallel to the vagus and accessory nerves on the dorsal portion of the ICA. Roberto et al.13) dissected the HGN inferior and medial to the DMPB and reported that it was located near and superior to the CCAB, identified by its pulsation. Although the CCA appeared in variable locations in this study, CCAB was a continuous valid landmark in HGN dissection. The digastric muscle was a good enough landmark to find the HGN, as mentioned in many previous reports1,3,9,13,16,19,23). However, most of these studies did not use only the DMPB as a landmark. As mentioned above, the carotid vessels, jugular vein, and DMPB are used together as landmarks3,13,23) as the high cervical and submandibular anatomy is very complicated and variable. According to this study, although the location of the CCAB was not the same due to interindividual variations, the HGN was mostly detected in the area between the DMPB and the CCAB. The HGN appeared under the DMPB, and the crossing point corresponded to about 65.5% of the whole length of the DMPD from the digastric groove. The HGN was located within the area between the CCAB and the DMPB. Considering the complicated anatomy of the cervical and submandibular region, the use of only one surgical landmark is not recommended. The DMPB and the CCAB represent good landmarks during submandibular dissection to identify the HGN.
Although a great deal of effort was made to acquire accurate measurements, this study still has several limitations. Formalin-fixed cadavers were used in this study, and therefore, the muscles and tissues were firmly fixed. Therefore, there could be differences in tissue extension or muscle length depending on the neck rotation angle, and there is no way to correct this variation. Thus, there will always be differences in these measurements depending on surgical position when applied under clinical conditions.
These measurements will help not only in finding the FN and HGN but also in defining the appropriate site for anastomosis during surgery. Additionally, nerve injury and operation time will be reduced, thereby benefiting patients.
CONCLUSION
The FN in submandibular region was found about 8 mm anterior and about 5 mm superior to the MPT. Thus, the MPT represents a good landmark for FN dissection. The HGN is located under the DMPB about 65.5% of the whole length of the DMPB from its origin (35.8±5.7 mm from the digastric groove). HGN intersects with ICA and ECA at distances of 18.5±6.7 mm and 15.5±5.1 mm from the CCAB, respectively.
This study provids useful information regarding the morphometric anatomy of the submandibular region and the presented morphological data on the nerves and the surrounding structures will aid in understanding the anatomical structures more accurately to reduce the risk of complications associated with HFNA.









 XML Download
XML Download