

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gunshot wounds to the upper cervical spine are rare in South Korea due to gun control. Due to the location and nature of these injuries, patients can present with concomitant airway damage, esophageal perforation, vascular injury, or spinal cord injury6). These conditions may present impending threats to the patient's survival. Therefore, gunshot wounds to the upper cervical spine without neurological deficits are rarely observed. To our knowledge, there is no published report that describes surgical removal of a bullet from the anterior arch of the C1 vertebra in South Korea. In this report, we describe our experience with the surgical removal of a bullet located in the C1 anterior arch using a transoral approach.
CASE REPORT
A 48-year-old man was admitted to the emergency room because of a self-inflicted single gunshot wound to the mouth. The patient was awake and alert without dyspnea or broken teeth.
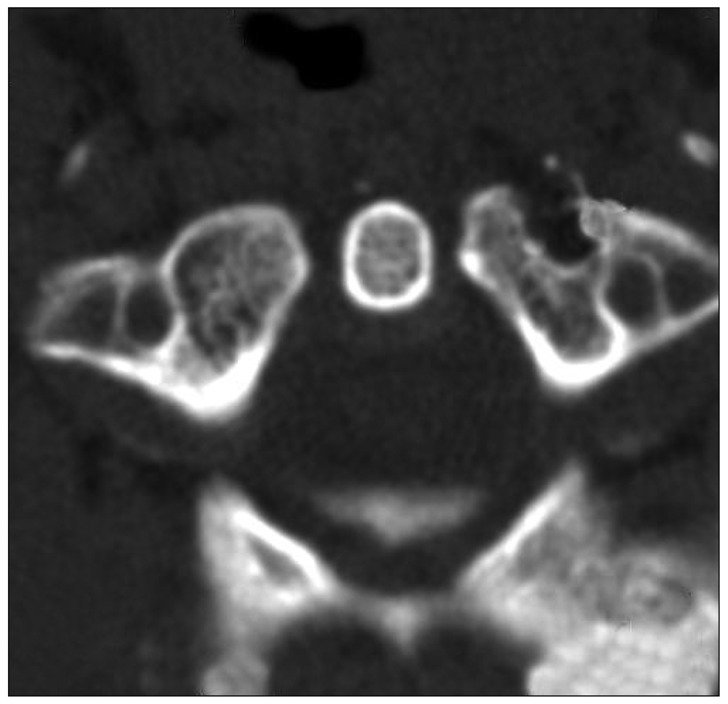
There was no evidence of neurological deficits or major vessel injury. A review of the patient's past medical history showed that he suffered from depressive disorder for 6 years and had received treatment for this condition. During the physical examination, the patient was alert and fully oriented. Aerodigestive involvement was not detected, and no neurologic abnormalities were found in the cranial nerves or cerebellar system. The bullet had passed along the right side of the mouth and exit wound was on the dorsal portion of the hard palate. A second entry wound was on the oropharynx at the C1 level. A single bullet lodged in the anterior arch of C1 was found on the simple lateral radiograph and computed tomographic (CT) scans (Fig. 1). Fortunately, the dural sac, trachea, esophagus, and vertebral artery were undamaged.
Emergent surgery using a transoral approach was performed to remove the bullet. The patient was placed on the operating table with the head in extension while under general anesthesia and with orotracheal intubation. A self-retaining oral retractor was placed over the teeth and expanded to keep the mouth open. To obtain an operational view, the soft palate was divided with an incision along the midline extending from the junction with the hard palate to the base of the uvula. The uvula was tracted using a red rubber catheter. An incision was made in the posterior pharyngeal mucosa from the base of the clivus to the upper border of the third cervical vertebra. Pharyngeal mucosa, pharyngeal constrictor musculature, and longus colli and longus capitis musculature were sequentially incised. A lead bullet about 1 cm in length was removed from the C1 anterior arch. There was no cerebrospinal fluid leakage and the C1 was not fragmented. Watertight closure of the posterior pharynx was performed in two layers. The soft palate is then carefully approximated in three layers (Fig. 2). At the 9-month follow-up, the patient had no neurologic sequelae and dynamic (flexion and extension) radiographs and CT scans did not reveal any instability.
DISCUSSION
Various clinical findings can accompany gunshot penetration into the cervical spine. In our patient, he had been injured by gunshot from an air pistol that used low velocity bullets. In general, low velocity bullets cause relatively little soft tissue trauma due to their low residual kinetic energy after penetrating the skin. If a bullet strikes a bone, most of its energy may be spent in fracturing that bone6). The consequences of gunshot entry into the upper cervical spine are frequently devastating, including spinal cord injury, vertebral artery injury, and even death resulting from airway dysfunction4,5,7). Moreover, a projectile can cause tissue trauma without coming into direct contact with the tissue through the concussive effect of the bullet2). The clinical presentation of patients with major vascular injury, multiple penetrating wounds, or other life-threatening injuries typically obscures subtle signs of aerodigestive penetration1). Patients with cervical spine gunshot injuries rarely sustain a fracture alone without neurologic deficits or retain vertebral missile fragments. Some authors have recommended a non-surgical approach for treating gunshot wounds in the cervical spine with the belief that further manipulation increases the chance of additional tissue trauma subsequent infection11). However, missiles retained in the anterior portion of C1-C2 vertebrae can cause both short-term and long-term complications even in stabilized patients who do not show signs of neurological deficits4). These complications include migration of the bullet fragments, central nervous system infections, osteomyelitis, or abscess formation. Migration anteriorly would lead to possible aspiration of the foreign body, and dorsal migration would lead to possible spinal cord compression or inflammation of the epidural space6). Atlanto-occipital subluxation is another possible complication if an extensive inflammatory reactions result in ligamentous laxity12). Romanick et al.10) reported frequent infection in civilians sustaining colonic injury resulting from low velocity, low thoracic, and lumbar spinal gunshot penetration. They recommended early bullet removal and debridement of the spine and missile tract because it was felt that the bullets could become coated with bacteria and serve as a nidus of infection4,10). Moreover, lead poisoning can result from a retained bullet or missile although this is relatively rare3,8,9). These factors make the prompt surgical removal of bullets a reasonable treatment option. Therefore, early surgical removal of the bullet and debridement was performed in our patient without incurring any neurological complications.

 XML Download
XML Download