

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is the most prevalent chronic respiratory disease, and the third leading cause of death in 2017.1 It was the 11th leading cause of disability-adjusted life years (DALYs) in 1990 but reached the 6th in 2019, increasing the burden of disease.2 COPD was the third leading cause of DALYs in Korea,3 with a 5-year mortality rate of 25.4%.4 However, according to a large-scale epidemiological study, the rate of COPD underdiagnosis is significantly high at 81.4%.5
Early detection and treatment of COPD are critical for improving COPD-related health outcomes and reducing burden of disease. As a result, it is possible to consider performing prebronchodilator spirometry in primary care for COPD diagnosis.6 The most reproducible and objective measurement of airflow restriction is spirometry, which measures the volume of air entering and exiting the lungs.6 COPD diagnosis could be confirmed via post-bronchodilator spirometry in anyone suspected of COPD.7 However, many clinical guidelines recommend performing spirometry on only people with respiratory symptoms or a history of exposure to COPD risk factors.67 Whereas screening spirometry for asymptomatic adults without respiratory symptoms is not recommended.89
A systematic review (SR) study on screening spirometry for asymptomatic adults to detect undiagnosed early-stage COPD was conducted by the US Preventive Services Task Force (USPSTF).10 In this previous study, the accuracy of screening questionnaires and office-based screening pulmonary function testing and the efficacy and harms of screen-detected COPD treatment were identified in asymptomatic adults through a SR.10 There was no direct evidence for judging COPD screening benefits for asymptomatic adults using questionnaires and office-based screening pulmonary function testing and the benefits of screen-detected COPD treatment.10
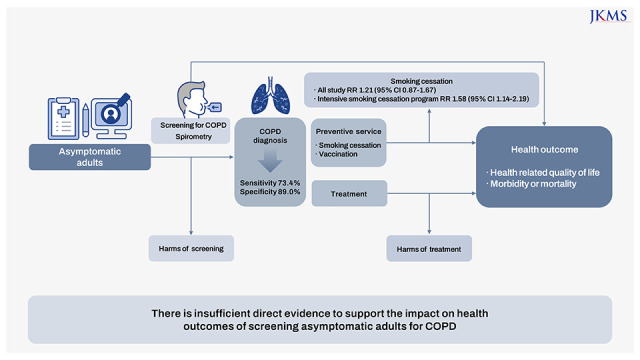
However, respiratory disease concerns have increased significantly as a result of worsening air pollution and population aging, both of which are risk factors for COPD.6 The risk of COPD may increase in high-income countries, especially as the population ages faster as a result of longer life expectancy. Nonetheless, there is a lack of public awareness of COPD.11 When people are diagnosed with COPD, more than half of their lung function was usually impaired.12 In the United States, 72% of participants in the National Health and Nutrition Examination Survey (NHANES) with obstructive pulmonary disease were not diagnosed,13 and only 44.2% of patients with self-reported COPD took any medication.14 Furthermore, in the Korea National Health and Nutrition Examination Survey (KNHANES), only 2.8% of COPD patients identified through spirometry have been diagnosed by physicians, and only 1.6% have been treated.15 Therefore, there is a growing demand for introducing COPD screening into the national health screening program. The purpose of this study is to evaluate the benefits and harms of screening for COPD in asymptomatic adults. Unlike the previous SR study, Guirguis-Blake (2016), we limited the COPD screening method to spirometry, and the COPD treatment included three representative COPD pharmacotherapies and pulmonary rehabilitation. The studies selected through SR were then analyzed by meta-analyses.
METHODS
Search strategy
In this study, seven key questions (KQs) were developed based on the previous SR study, but with the interventions typically utilized in South Korea limited10 (Fig. 1). In a previous SR study for KQs 1-5, prebronchodilator spirometry, questionnaires or risk assessment tools, peak flow meter, and postbronchodilator spirometry were all included as interventions.10 However, we only used prebronchodilator spirometry as an intervention for KQs 1-5 in this study. This is because COPD diagnosis requires spirometry,6 and post-bronchodilator spirometry is difficult to perform in the primary clinical setting, where most screening are conducted, due to facility and personnel constraints in South Korea. For KQs 6 and 7, previous SR study included long-acting β-agonists, long-acting anticholinergics, and inhaled corticosteroids (ICS) as interventions.10 We focused on three representative COPD pharmacotherapies for KQs 6 and 7 that are commonly used in Korea (tiotropium; umeclidinium/ vilanterol combination; fluticasone/ vilanterol combination). Pulmonary rehabilitation was also included in the interventions for KQs 6 and 7, according to pulmonology specialists’ suggestions.
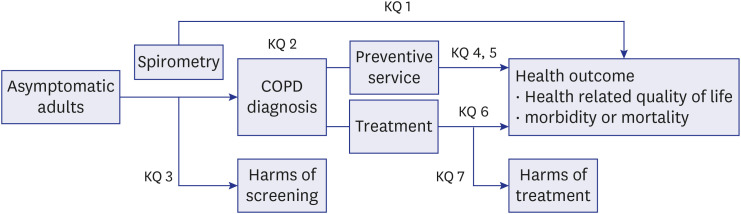
Fig. 1
Analytic framework.
[KQ 1] Screening asymptomatic adults for COPD via spirometry results in improved COPD-related health outcomes (health-related quality of life or morbidity or mortality)?
[KQ 2] What is the diagnostic accuracy of screening spirometry in diagnosing COPD in asymptomatic adults?
[KQ 3] What are the adverse effects of screening spirometry in diagnosing COPD in asymptomatic adults?
[KQ 4] Does screening spirometry for COPD to asymptomatic adults improve smoking cessation rates?
[KQ 5] Does screening spirometry for COPD to asymptomatic adults improve vaccination rates?
[KQ 6] Does treatment for asymptomatic mild or moderate COPD patients detected via screening spirometry improve COPD related health outcomes?
[KQ 7] Does treatment for asymptomatic mild or moderate COPD patients detected via screening spirometry have adverse effects?
COPD = chronic obstructive pulmonary disease.
![]()
Search and review were performed, combining the seven KQs mainly into three parts. First, we searched for studies that performed screening spirometry for COPD on asymptomatic adults aged over-40 to identify primary benefits and harms (KQs 1-3). In the second search, we confirmed whether screening spirometry for COPD to asymptomatic adults made differences in the efficacy and utilization rates of preventive services (KQs 4, 5). In the third search, we identified the efficacy and harms of treatment in asymptomatic mild or moderate COPD patients detected via screening spirometry (KQs 6, 7).
We searched for articles three times in the following databases: MEDLINE, EMBASE, Cochrane Library, and regional databases (KoreaMed, KMbase, RISS, KISS, NDSL) with the time frame from inception to January 2020 (KQs 1-3), February 2020 (KQs 6, 7), and March 2020 (KQs 4, 5). The search terms used in the study are presented in the Supplementary Data 1.
Study selection
According to the inclusion criteria (Supplementary Data 2) set in advance, four independent reviewers conducted a full article review after screening with titles and abstracts for the searched literature. The inclusion criteria were prepared to consider the Korean health care system characteristics from the previous SR.10 Studies with asymptomatic adults aged over-40 were included throughout KQs 1-7. Exceptionally, in KQs 4 and 5, the age restriction was not applied since the objective of these KQs was to confirm the difference in preventive services when accompanying spirometry regardless of COPD diagnosis. In line with the previous SR, KQ 4 targeted only current smokers, and KQs 6 and 7 were limited to mild COPD (forced expiratory volume in 1 second [FEV1] ≥ 80% predicted) or moderate COPD (FEV1 50–79% predicted) patients.10 Likewise, asymptomatic adults was defined similarly: not COPD patients; COPD patients whose symptoms are not detected by the patient or physician; patients with nonspecific symptoms that are not perceived to be related to COPD.10 In this study, even though they had mild symptoms such as cough, those not diagnosed with COPD were considered the corresponding target population because their symptoms were not recognized to be related to COPD. The COPD screening tests for KQs 1-3 were limited to prebronchodilator spirometry measured as FEV1/ forced vital capacity (FVC) or FEV1/forced expiratory volume in 6 seconds (FEV6), reflecting Korean real-world screening circumstances.16
In KQs 6 and 7, frequently used pharmacotherapies for COPD were identified via National Health Insurance claims data to set search terms for COPD treatment. Three representative pharmacotherapies for COPD were selected by consulting pulmonology specialists. Pulmonary rehabilitation with aerobically demanding exercise for more than four weeks was included as an additional treatment.17 Since no studies were targeting screening-detected asymptomatic mild or moderate COPD patients in the search results, we added the expanded population (patients with mild or moderate COPD) to the additional questions, KQs 6-1 and 7-1 done in the previous SR.10 The results of KQs 6-1 and 7-1 were presented only in Supplementary materials (Supplementary Figs. 6, 7, 8, 9, Supplementary Tables 4, 5, 6, 7, 8).
In KQs 1, 4, and 6, the study design was limited to randomized controlled trials (RCTs) and SRs. In KQ 2, diagnostic accuracy studies and SRs using post-bronchodilator spirometry as a reference standard were selected. In KQ 3, the study design was limited to RCTs, large screening registries or database observational studies, cohort studies, and SRs. In KQ 7, RCTs, large screening registries, SRs, and supplemented information reported by the US Food and Drug Administration were included.10
Data extraction and risk of bias assessment
Four independent reviewers reviewed the literature according to the inclusion criteria, and any discrepancies or uncertainties were resolved through consensus. One reviewer independently extracted the data in the standardized abstraction form, while the other two reviewers confirmed the data.
The risk of bias was evaluated using Quality Assessment of Diagnostic Accuracy Studies 2.0 (QUADAS-2)18 for the included diagnostic accuracy studies of KQs 1-3 and the Cochrane Risk of Bias19 for the included RCTs of KQs 4-7. Two independent reviewers evaluated included studies, and disagreements were resolved through discussion.
Statistical analysis
Hierarchical summary receiver-operating characteristic (HSROC) curves, including the confidence and the prediction regions, were constructed for diagnostic accuracy studies. The gap between the confidence and prediction region changed according to the degree of homogeneity of the study population. Summary estimates for sensitivity and specificity of included studies were estimated using the metandi command in Stata 14 (Stata-Corp, College Station, TX, USA). Those estimates were calculated by reflecting the heterogeneity of the study population and screening tools in the subgroup analysis.
Treatment efficacy and harms were presented as the following summary estimates: mean difference for continuous outcomes, odds ratios for the number of patients with one or more exacerbations and the number of patients with one or more adverse events, the rate ratio for the number of exacerbations, and risk ratio (RR) for abstinence rate. Outcomes were assessed using a random effect model. Still, a fixed-effect model was also used when the number of included studies was small, or the heterogeneity between studies was low (I2 ≤ 25%). Treatment efficacy and harms were calculated using the metandi command in Stata 14. Heterogeneity between studies was identified using forest plot and I2 statistics (≥ 50%).
RESULTS
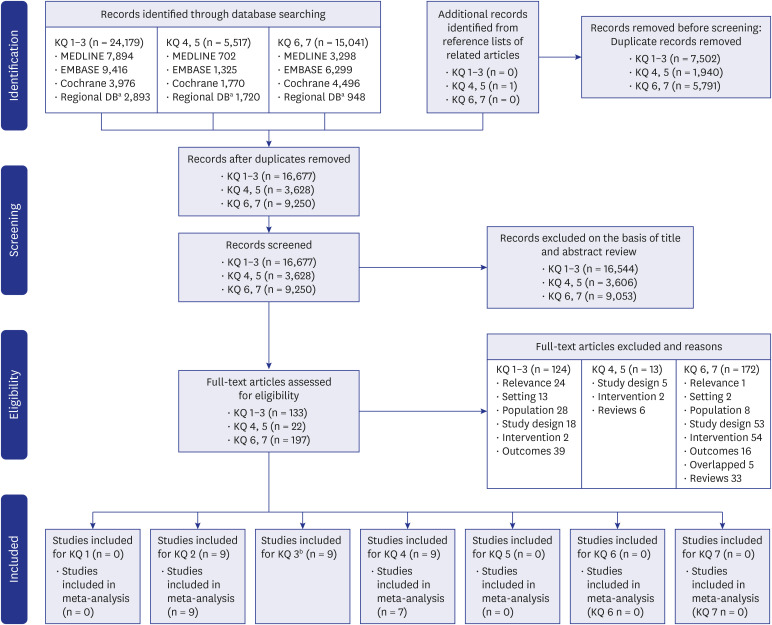
Eighteen studies met the inclusion criteria (Fig. 2), of which sixteen studies were included in meta-analyses.
Effect of screening on health outcome
[KQ 1] Screening asymptomatic adults for COPD via spirometry results in improved COPD-related health outcomes (health-related quality of life or morbidity or mortality)?
No studies have been found confirming the effect of screening COPD via spirometry on health outcomes.
Screening spirometry
[KQ 2] What is the diagnostic accuracy of screening spirometry in diagnosing COPD in asymptomatic adults?
[KQ 3] What are the adverse effects of screening spirometry in diagnosing COPD in asymptomatic adults?
Two studies2021 confirming the diagnostic accuracy of prebronchodilator FEV1/FVC measured with a spirometer and seven studies22232425262728 confirming that of the prebronchodilator FEV1/FEV6 with a handheld spirometer were identified (Table 1). Out of these, seven studies20212224252628 were published in a period not covered by the previous SR or were newly added in this updated study while adjusting the inclusion criteria.
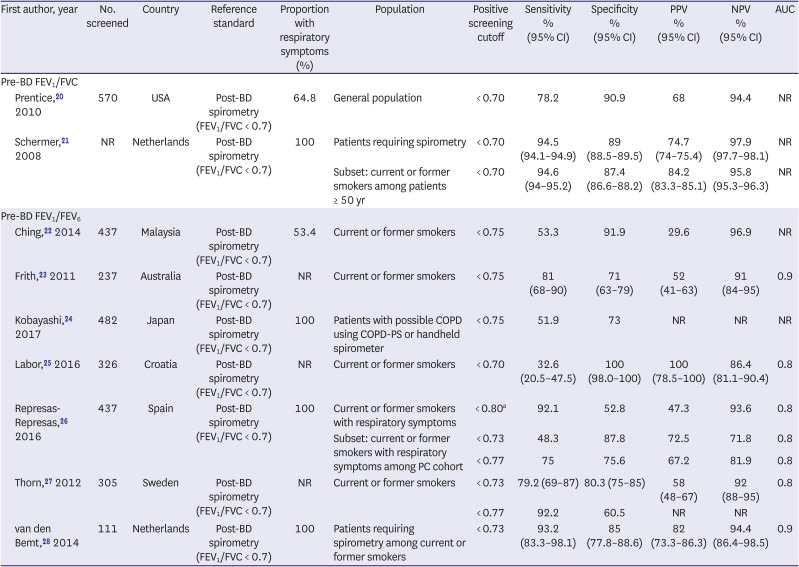
Table 1
Diagnostic accuracy values for screening spirometry (key question 2)
| First author, year | No. screened | Country | Reference standard | Proportion with respiratory symptoms (%) | Population | Positive screening cutoff | Sensitivity % (95% CI) | Specificity % (95% CI) | PPV % (95% CI) | NPV % (95% CI) | AUC | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-BD FEV1/FVC | ||||||||||||
| Prentice,20 2010 | 570 | USA | Post-BD spirometry (FEV1/FVC < 0.7) | 64.8 | General population | < 0.70 | 78.2 | 90.9 | 68 | 94.4 | NR | |
| Schermer,21 2008 | NR | Netherlands | Post-BD spirometry (FEV1/FVC < 0.7) | 100 | Patients requiring spirometry | < 0.70 | 94.5 (94.1–94.9) | 89 (88.5–89.5) | 74.7 (74–75.4) | 97.9 (97.7–98.1) | NR | |
| Subset: current or former smokers among patients ≥ 50 yr | < 0.70 | 94.6 (94–95.2) | 87.4 (86.6–88.2) | 84.2 (83.3–85.1) | 95.8 (95.3–96.3) | NR | ||||||
| Pre-BD FEV1/FEV6 | ||||||||||||
| Ching,22 2014 | 437 | Malaysia | Post-BD spirometry (FEV1/FVC < 0.7) | 53.4 | Current or former smokers | < 0.75 | 53.3 | 91.9 | 29.6 | 96.9 | NR | |
| Frith,23 2011 | 237 | Australia | Post-BD spirometry (FEV1/FVC < 0.7) | NR | Current or former smokers | < 0.75 | 81 (68–90) | 71 (63–79) | 52 (41–63) | 91 (84–95) | 0.9 | |
| Kobayashi,24 2017 | 482 | Japan | Post-BD spirometry (FEV1/FVC < 0.7) | 100 | Patients with possible COPD using COPD-PS or handheld spirometer | < 0.75 | 51.9 | 73 | NR | NR | NR | |
| Labor,25 2016 | 326 | Croatia | Post-BD spirometry (FEV1/FVC < 0.7) | NR | Current or former smokers | < 0.70 | 32.6 (20.5–47.5) | 100 (98.0–100) | 100 (78.5–100) | 86.4 (81.1–90.4) | 0.8 | |
| Represas-Represas,26 2016 | 437 | Spain | Post-BD spirometry (FEV1/FVC < 0.7) | 100 | Current or former smokers with respiratory symptoms | < 0.80a | 92.1 | 52.8 | 47.3 | 93.6 | 0.8 | |
| Subset: current or former smokers with respiratory symptoms among PC cohort | < 0.73 | 48.3 | 87.8 | 72.5 | 71.8 | 0.8 | ||||||
| < 0.77 | 75 | 75.6 | 67.2 | 81.9 | 0.8 | |||||||
| Thorn,27 2012 | 305 | Sweden | Post-BD spirometry (FEV1/FVC < 0.7) | NR | Current or former smokers | < 0.73 | 79.2 (69–87) | 80.3 (75–85) | 58 (48–67) | 92 (88–95) | 0.8 | |
| < 0.77 | 92.2 | 60.5 | NR | NR | ||||||||
| van den Bemt,28 2014 | 111 | Netherlands | Post-BD spirometry (FEV1/FVC < 0.7) | 100 | Patients requiring spirometry among current or former smokers | < 0.73 | 93.2 (83.3–98.1) | 85 (77.8–88.6) | 82 (73.3–86.3) | 94.4 (86.4–98.5) | 0.9 | |
CI = confidence interval, PPV = positive predictive value, NPV = negative predictive value, AUC = area under the receiver operating characteristic curve, BD = bronchodilator, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, NR = not reported, FEV6 = forced expiratory volume in 6 seconds, PC = primary care, COPD = chronic obstructive pulmonary disease, COPD-PS = COPD Population Screener.
aDiagnostic accuracy values applied to FEV1/FEV6 < 0.73 was not reported.
![]()
In four studies,21242628 spirometry was conducted on COPD suspected cases. In the remaining five studies, spirometry was performed on a general population of persons not suspected of COPD. The study population of four studies except for one20 was current or former smokers. The average age of the study population was 40–50 years in eight studies, and that of the remaining one21 study was over 21 years, but the results of more than 50 years were presented separately.
FEV1/FVC’s sensitivity range measured by prebronchodilator spirometer was 78.2–94.6%, and the specificity range was 87.4–90.9%.2021 Prebronchodilator FEV1/FEV6’s sensitivity range measured with a handheld spirometer was 32.6–93.2% and the specificity range was 52.8–100%,22232425262728 which showed generally lower diagnostic accuracy than FEV1/FVC. As the cutoff of FEV1/FEV6 increased within the same study, the sensitivity increased while the specificity decreased.2627
When evaluating the methodological quality of included studies, the risk of bias and applicability concerns were low in the index test and reference standard domains (Supplementary Fig. 1). In the patient selection domain, patient selection methods and included patients in some studies21232428 were not suitable, resulting in a high risk of bias and applicability concerns. The risk of bias was high in the flow and timing domain in some studies,222427 because the rate of receiving reference tests was low and the time interval between the index test and reference test was not reported (Supplementary Fig. 2).
When multiple cutoffs were presented within one study, meta-analysis was performed using the sensitivity and specificity calculated from the cutoff closest to prebronchodilator FEV1/FEV6 < 0.73, since FEV1/FEV6 < 0.73 was used as a substitute for FEV1/FVC < 0.7 2930 in this study. The pooled sensitivity and specificity for all studies (n = 9) were 73.4% and 89.0%, respectively (Supplementary Table 1). When plotting the HSROC curve for the entire study, the gap between the confidence and the prediction regions was vast, and there were two studies2124 markedly separated from the curve (Supplementary Fig. 3A). The study populations in these two studies were those who were COPD suspected. In five studies2022232527 of having subject to the general population, not those COPD suspected, the sensitivity and specificity were 69.5% and 93.0%, respectively. Out of these five studies, the sensitivity and specificity of the four studies22232527 using FEV1/FEV6 were 65.4% and 92.8%, respectively. When plotting the HSROC curve using four or these five studies for the general population, the confidence and prediction regions were almost identical (Supplementary Fig. 3B).
Harms of screening spirometry were identified in only false positives and false negatives in nine diagnostic accuracy studies.202122232425262728 When calculating the results from the cutoff closest to FEV1/FEV6 < 0.73, the false-positive rate was 0–28.6%, and the proportion of COPD diagnosis missed was 5.4–67.4% (Supplementary Table 2). As the cutoff of FEV1/FEV6 increased within the same study, the false positive rate increased while the proportion of COPD diagnosis missed decreased.
Targeted preventive services
[KQ 4] Does screening spirometry for COPD to asymptomatic adults improve smoking cessation rates?
[KQ 5] Does screening spirometry for COPD to asymptomatic adults improve vaccination rates?
Nine studies were identified comparing the smoking cessation effect of the smoking cessation intervention after conducting screening spirometry with feedback on the spirometry results, and the smoking cessation intervention without spirometry, or without feedback on the results even if spirometry was performed (Table 2).313233343536373839 The primary outcome was a self-reported or biochemically validated smoking abstinence rate or the number of quit attempts. Four35363739 of these studies were published before 2000. Some studies31343639 excluded from the previous SR were included in this study while revising the inclusion criteria. One study38 was published in a period not covered by the previous SR. The mean age of the study population varied from 30 to 50, and the male proportion was 37–99%, which differed among studies. The average smoking history also showed various distributions, ranging from 16.6–62.8 pack-years. The range of point prevalence of smoking cessation was 6.5–24.4%, and the sustained abstinence rate was 8.7–42.3%. The biochemically validated smoking abstinence rate was 6.5–20%, and the self–reported smoking abstinence rate was 8.7–42.3%. Within the same study, the self–reported smoking abstinence rate was higher than the biochemically validated one.35 As a result of the risk of bias assessment for included studies, the risk of bias was low in blinding outcome assessment and selective reporting domains (Supplementary Fig. 4). In several studies (n = 6),313233353839 the risk of bias in the allocation concealment domain was unclear because allocation concealment methods were not reported. In the blinding of participants and personnel domain, the risk of bias was high as most studies were not double-blinded. It seems that blinding of participants and personnel is difficult due to the nature of the smoking cessation intervention study. In the incomplete outcome data domain, the risk of bias in five studies3435373839 was unclear since the reasons for missing outcome data or analysis methods (intention-to-treat or as-treated analysis) were not reported (Supplementary Fig. 5).
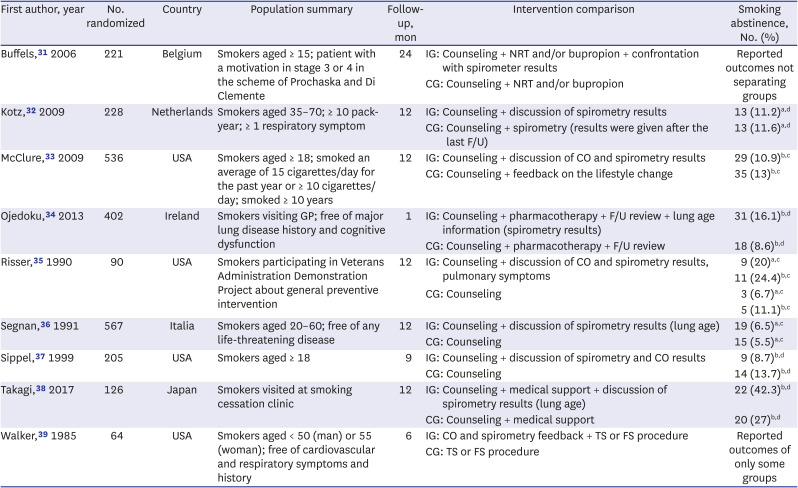
Table 2
Study characteristics and smoking cessation effect (key question 4)
| First author, year | No. randomized | Country | Population summary | Follow-up, mon | Intervention comparison | Smoking abstinence, No. (%) |
|---|---|---|---|---|---|---|
| Buffels,31 2006 | 221 | Belgium | Smokers aged ≥ 15; patient with a motivation in stage 3 or 4 in the scheme of Prochaska and Di Clemente | 24 | IG: Counseling + NRT and/or bupropion + confrontation with spirometer results | Reported outcomes not separating groups |
| CG: Counseling + NRT and/or bupropion | ||||||
| Kotz,32 2009 | 228 | Netherlands | Smokers aged 35–70; ≥ 10 pack-year; ≥ 1 respiratory symptom | 12 | IG: Counseling + discussion of spirometry results | 13 (11.2)a,d |
| CG: Counseling + spirometry (results were given after the last F/U) | 13 (11.6)a,d | |||||
| McClure,33 2009 | 536 | USA | Smokers aged ≥ 18; smoked an average of 15 cigarettes/day for the past year or ≥ 10 cigarettes/day; smoked ≥ 10 years | 12 | IG: Counseling + discussion of CO and spirometry results | 29 (10.9)b,c |
| CG: Counseling + feedback on the lifestyle change | 35 (13)b,c | |||||
| Ojedoku,34 2013 | 402 | Ireland | Smokers visiting GP; free of major lung disease history and cognitive dysfunction | 1 | IG: Counseling + pharmacotherapy + F/U review + lung age information (spirometry results) | 31 (16.1)b,d |
| CG: Counseling + pharmacotherapy + F/U review | 18 (8.6)b,d | |||||
| Risser,35 1990 | 90 | USA | Smokers participating in Veterans Administration Demonstration Project about general preventive intervention | 12 | IG: Counseling + discussion of CO and spirometry results, pulmonary symptoms | 9 (20)a,c |
| 11 (24.4)b,c | ||||||
| CG: Counseling | 3 (6.7)a,c | |||||
| 5 (11.1)b,c | ||||||
| Segnan,36 1991 | 567 | Italia | Smokers aged 20–60; free of any life-threatening disease | 12 | IG: Counseling + discussion of spirometry results (lung age) | 19 (6.5)a,c |
| CG: Counseling | 15 (5.5)a,c | |||||
| Sippel,37 1999 | 205 | USA | Smokers aged ≥ 18 | 9 | IG: Counseling + discussion of spirometry and CO results | 9 (8.7)b,d |
| CG: Counseling | 14 (13.7)b,d | |||||
| Takagi,38 2017 | 126 | Japan | Smokers visited at smoking cessation clinic | 12 | IG: Counseling + medical support + discussion of spirometry results (lung age) | 22 (42.3)b,d |
| CG: Counseling + medical support | 20 (27)b,d | |||||
| Walker,39 1985 | 64 | USA | Smokers aged < 50 (man) or 55 (woman); free of cardiovascular and respiratory symptoms and history | 6 | IG: CO and spirometry feedback + TS or FS procedure | Reported outcomes of only some groups |
| CG: TS or FS procedure |
IG = intervention group, CO = carbon monoxide, TS = taste satiation, FS = focused smoking, CG = control group, NRT = nicotine replacement therapy, F/U = follow-up, GP = general practice.
aBiochemically validated smoking abstinence; bSelf-reported smoking abstinence; cPoint prevalence of smoking cessation; dSustained abstinence.
![]()
The abstinence rate was calculated as the RR using the number of people who successfully quit smoking in the intervention and control groups (Supplementary Table 3). The number of quit attempts was calculated as the RR using the number of people reporting that they tried to quit smoking. Among the included studies (n = 9), meta-analyses were performed except for two studies3139 with incomplete outcomes. The relative effect of smoking cessation intervention compared with or without screening spirometry on the abstinence rate was 1.21. However, it was not statistically significant (RR, 1.21; 95% confidence interval [CI], 0.87–1.67). In studies with smoking cessation interventions that provided smoking cessation medicines or intensive counseling, the relative effect of smoking cessation intervention with screening spirometry was 58% greater (RR, 1.58; 95% CI, 1.14–2.19) than without screening. This result can be interpreted as screening spirometry, and its feedback became effective only when the smoking cessation programs are systematically provided at public health centers or medical institutions.
None of the other subgroup analyses for the abstinence rate were statistically significant. Meta-analysis of the number of quit attempts was not statistically significant, either.
In addition, no studies have been found to report the effect of screening spirometry on the vaccination rate.
Treatment efficacy and harms
[KQ 6] Does treatment for asymptomatic mild or moderate COPD patients detected via screening spirometry improve COPD related health outcomes?
[KQ 7] Does treatment for asymptomatic mild or moderate COPD patients detected via screening spirometry have adverse effects?
Studies targeting COPD patients detected via screening spirometry have not been identified.
DISCUSSION
This study updated the previous SR study by systematically reviewing the literature of databases from their inception to January 2020. Key questions and inclusion/exclusion criteria were revised to reflect the Korean health care system setting. Also, in this study, meta-analyses were conducted, with the heterogeneity of the study explored through subgroup analysis even though meta-analyses were not performed due to heterogeneity between included studies in previous SR study. No studies have not been identified examining whether screening spirometry for COPD affects health outcomes, consistent with the previous SR.
Table 3 summarizes the evidence for KQs 1-7. The screening method was limited to prebronchodilator spirometry while revising inclusion criteria for exploring diagnostic accuracy, unlike the previous SR. As a result, seven studies were added to the previous SR’s studies. When calculating the sensitivity and specificity by meta-analysis for all included studies (n = 9), the gap between the HSROC curve’s confidence and the prediction regions was wide. Meanwhile, confining studies targeting the general population, and not those COPD suspected, made the two regions almost identical, and the sensitivity decreased slightly, but the specificity increased.
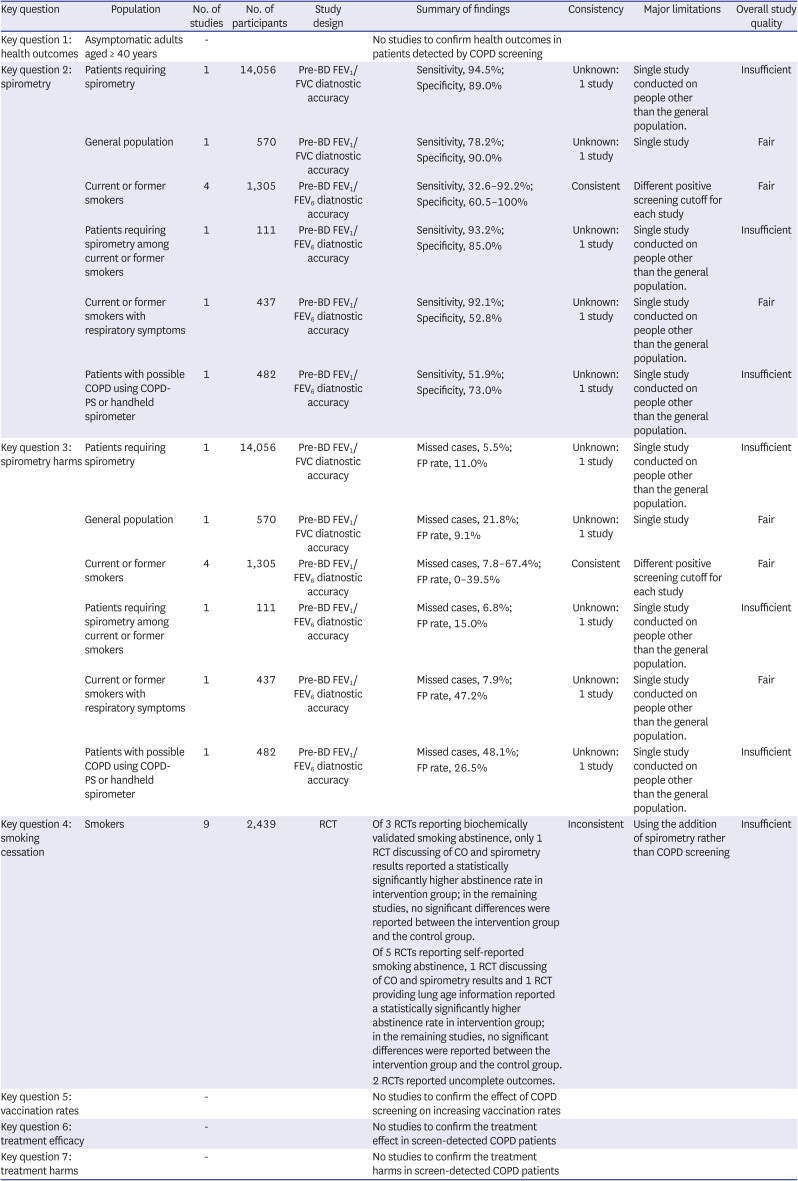
Table 3
Summary of evidence table
COPD = chronic obstructive pulmonary disease, BD = bronchodilator, FEV1 = forced expiratory volume in 1 second, FVC = forced vital capacity, FEV6 = forced expiratory volume in 6 seconds, COPD-PS = COPD Population Screener, FP = false positive, CO = carbon monoxide, RCT = randomized controlled trial.
![]()
Since smoking cessation is almost the only intervention for patients with an early diagnosis of mild or moderate COPD by screening, whether or not the abstinence rate increases following screening is an important indicator in reviewing the benefits of a COPD screening program. In searching for studies confirming screening spirometry’s effect on smoking cessation, five additional studies were included because the study quality was not considered in this study, unlike the previous study, and the search period was extended. The risk of bias in included studies (n = 9) was unclear or high in some domains. Meta-analyses results indicate that screening spirometry and its feedback increased the abstinence rate only the smoking cessation programs are provided similar to the smoking cessation program provided by the smoking cessation clinic. On the other hand, other subgroup analyses did not show a statistically significant effect on the abstinence rate and the number of quit attempts.
Treatment efficacy studies limited to COPD patients detected through screening spirometry were not identified as before. The previous SR study revealed that even with early COPD detection, the treatment efficacy confirmed in clinical trials was limited.10 Besides, the effectiveness may be smaller in patients with mild or moderate COPD detected by screening, and among the treatment, ICS-containing medication may have side effects.10 However, there is a lack of information on treatment-related harm from trials, implying that most treatments have no major adverse effects.10 Considering that there are many undiagnosed COPD patients worldwide including South Korea,540 the opportunity cost of including spirometry in the national health screening may not be enormous. In the case of South Korea, after government announced in 2021 that it would consider adding lung function tests for COPD screening to the list of the national health screening programs in the 3rd National Health Screening Plan (2021–2025), it has not been decided yet, but it is still being reviewed.
Meanwhile, in the evidence for smoking cessation, it was suggested that active smoking intervention is necessary after patient detection since the effect of screening spirometry occurs only when a smoking cessation program is provided through smoking cessation medicines or intensive counseling. Active cessation interventions are important because smoking is a major risk factor for COPD,6 and the interaction between smoking duration and age increases COPD severity.41
This study has the following limitations. First, there are restrictions on directly comparing the results of this study with those of the previous SR study because the inclusion/exclusion criteria used in the review are not entirely identical. However, the inclusion/exclusion criteria revision was done to reflect the actual clinical circumstances. For example, the screening method was limited to prebronchodilator spirometry, three representative pharmacotherapies were selected as treatment, and pulmonary rehabilitation was added in this study. Second, it should be noted that the methodological quality of the studies used in meta-analysis is uneven since the study quality was not considered as an exclusion criterion to get further information in this study, unlike the previous SR. Considering this problem, we tried to identify the differences between meta-analysis results through subgroup analysis according to publication year, especially for the studies related to smoking cessation with low quality. However, neither of the studies before and after 2000 showed statistical significance. Third, even though we tried to perform subgroup analyses for several factors, taking into account the heterogeneity between studies in meta-analyses, only a few of them were possible. This is because the number of included studies in most Key Questions was not sufficient. Lastly, even though seven KQs were established, direct evidence was identified only in KQs 2-4. In order to achieve more rigorous results with respect to the effectiveness of COPD screening in asymptomatic adults, more studies should be conducted on the final health outcomes of COPD screening in asymptomatic adults and the treatment effect of COPD patients identified through screening.
In this update to the systematic review, no direct evidence for the impact on health outcomes of screening asymptomatic adults for COPD was identified consistent with the previous SR. COPD screening’s effect on smoking cessation was presented only when a smoking cessation program is provided through smoking cessation medicines or intensive counseling. No direct evidence for confirming treatment efficacy targeting COPD patients detected via screening spirometry have been identified similar to the previous SR. Further research is necessary to confirm the benefits of COPD screening.
 XML Download
XML Download