

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patient safety is affected by various factors, such as the patient, task, individual and team characteristics, working conditions, organizational factors, and institutional context.1 Patient safety, therefore, calls for a systematic approach that emphasizes the role of not only the individual healthcare professional but also the organization.2
Patient safety culture (PSC) refers to a shared value of patient safety by the healthcare community and society in general, which is practiced on a regular basis and reproduced in a stable way. PSC can be measured by factors related to institutional compensation, support, and acceptance.345 Organizations that have a positive safety culture characteristically have communication based on trustworthiness from sharing confidence about the importance of safety and perception about mutual trust based on interactions between departments, organizations, and the organizational structure and system.3 A positive culture is essential for reducing patient harm and providing a safe work environment, including encouraging disclosure of patient safety incidents and supporting second victims.678 Although a strong PSC is essential for improving the quality of care, the strategic priorities, structure, funding, and governance of patient safety implementation differ across settings, cultures, contexts, and resources. In addition, it is difficult for healthcare professionals, who are overloaded with complex clinical multitasking, to learn additional competencies in patient safety that they can integrate into their practice. The WHO proposed The Global Patient Safety Action Plan 2021–2030 as a guide for the different stages of creating the capacity and capability to reduce avoidable harm in healthcare.9 Despite the importance of such a PSC, medical institutions suffer from “sick system syndrome” in a hierarchical order and a lack of mutual respect and teamwork. For the ultimate improvement of patient safety, efforts based on understanding by relevant managers and agencies are needed.10
In South Korea, the Patient Safety Act was enacted in 2016 and the first comprehensive plan for patient safety was announced in 2018 to create PSC. In the current situation, with various efforts being made at the national level and based on the experiences of the Accreditation Programs for Healthcare Organizations in Korea, active communication between hospitals, the government, and other interested parties is necessary.11 Additionally, an in-depth examination about the perceived PSC that medical professionals actually experience in clinical settings to prevent “sick system syndrome” due to top-down procedures must be conducted.12
There have been several studies regarding PSC among medical professionals in Korea131415; however, there have been almost no in-depth qualitative studies that account for patient safety-related policy changes. Furthermore, identifying how patient safety-related policy changes are implemented in healthcare practice in the early days and how such changes are perceived by healthcare professionals is an important endeavor that can shed light on how policies translate into change, and identify areas for improvement.
Considering the implementation of the patient safety policies by the government, this qualitative study presents an in-depth understanding of the current PSC in South Korean hospitals, as perceived by physicians and nurses.
Go to : 
METHODS
This qualitative study examined PSC in South Korea as perceived by physicians and nurses in Seoul and Gyeonggi-do. It was conducted in accordance with the Consolidated Criteria for Reporting Qualitative Research.16 The research team consisted of 10 researchers who usually conduct research related to public health, particularly patient safety. Five researchers were experienced in qualitative research, and five have a doctoral degree in medical or healthcare science. Three were professors and seven were researchers.
Participants
A total of 25 healthcare providers, who understood the purpose of this research and were willing to share their substantial stories about the topic, were conveniently recruited. The recruitment process continued until a relevant representation of healthcare providers who experienced the policy at hospitals was reached, with the following inclusion criteria: physicians and nurses who 1) were working in general hospitals with 200 or more beds, which were subject to patient safety-related systems by the Patient Safety Act; and 2) had at least six months of work experience in the hospital at the time of recruitment.
Data collection
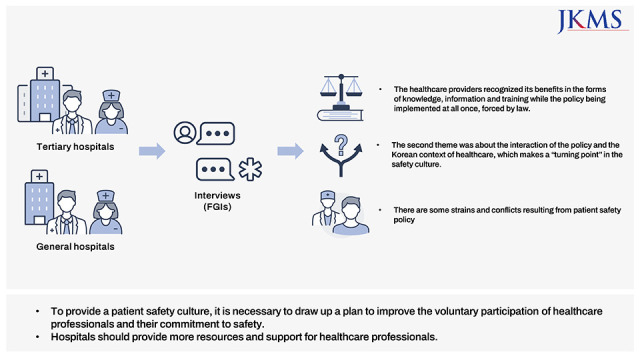
Focus group interviews (FGIs) were used for the study and it worked as an effective and trustworthy method to understand how the participants take in and respond to the safety policy through their interactions among themselves. An FGI guideline was developed based on findings from previous studies,171819 and included questions on PSC at the various levels, characteristics of PSC in South Korea, and factors considered important for building PSC (Table 1). Four FGIs arranged by occupation and institution type were conducted in January 2018: 1) physician group working at tertiary hospital; 2) nurse group working at tertiary hospital; 3) physician group working at general hospital; 4) nurse group working at general hospital. Each FGI was conducted until there were no more new comments, and each FGI lasted approximately two hours in a private space by two researchers.
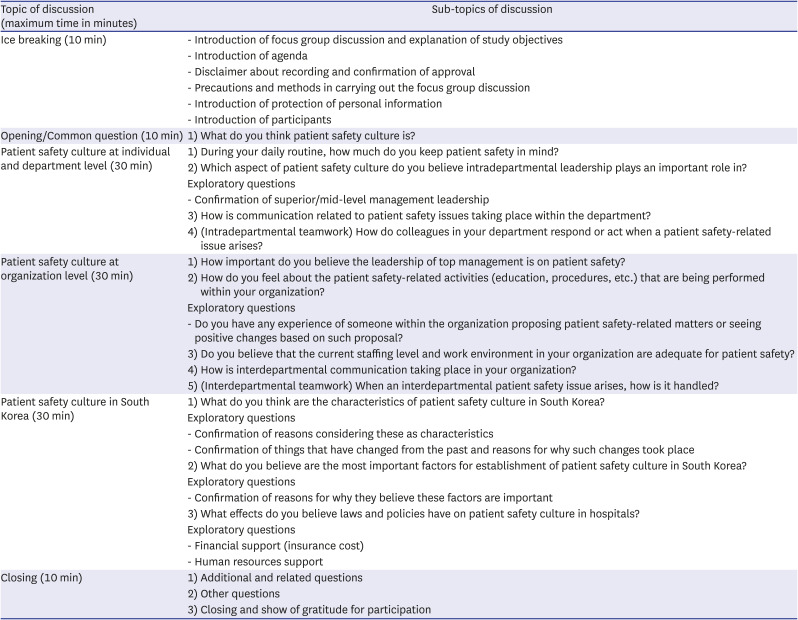
Table 1
The interview guideline used to collect data through focus group discussions
![]()
Data analysis
The data produced through the four FGIs were analyzed in two steps. First, the data were checked, examined, and reviewed by the whole research team. This process was done immediately after completing each FGI and debriefing session by the moderator, who was one of the researchers. This ensured that the important and significant findings were identified and included in relation to FGI data and the study’s purpose. Second, all transcripts of the four FGIs, which were recorded and transformed into written digital texts, were analyzed by conducting thematic analysis. Each researcher read all transcripts individually and performed open coding with the guidance from the debriefing session. The entire individual coding was verified during the group meeting of the research team, meaningful codes were refined, and three themes connecting all the codes were identified and underpinned by the data and the study’s focus. The thematic analysis of the FGI data was conducted in an inductive and interpretative way.
To ensure the rigor and trustworthiness of the qualitative study, this research was assessed based on the criteria offered by Lincoln and Guba.20 To establish truth-value, e-mails were sent to four participants to confirm the study results. Applicability was established by sharing the study results with four people who met the selection criteria of the study but did not participate in it. The four non-participants mostly agreed with the categories and replied that they were similar to their experiences. To establish consistency, seven researchers reviewed the data to prevent misinterpretation of participants’ responses. To establish neutrality, efforts were made to ensure that the experience, perception, and thoughts of the researchers related to PSC did not affect data analysis and interpretation of the results.
Ethics statement
This study was approved by the Institutional Review Board of National Evidence-based Collaborating Agency and the requirement for informed consent was waived (NECAIRB17-025).
Go to :
RESULTS
The characteristics of the participants are listed in Table 2. A total of three themes and seven categories were derived from open coding (Table 3).
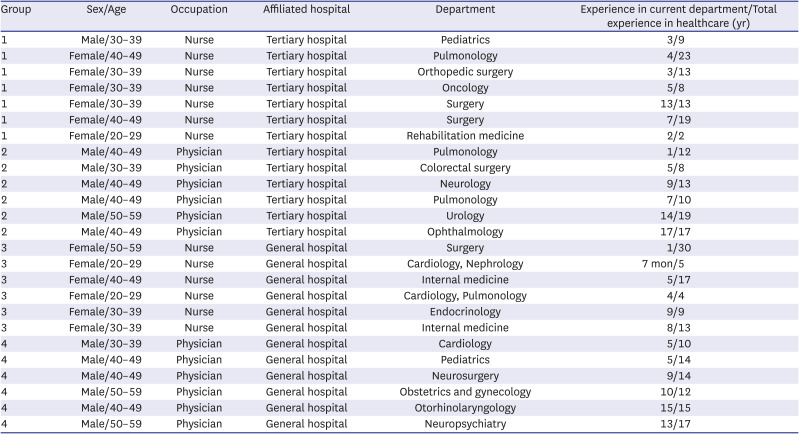
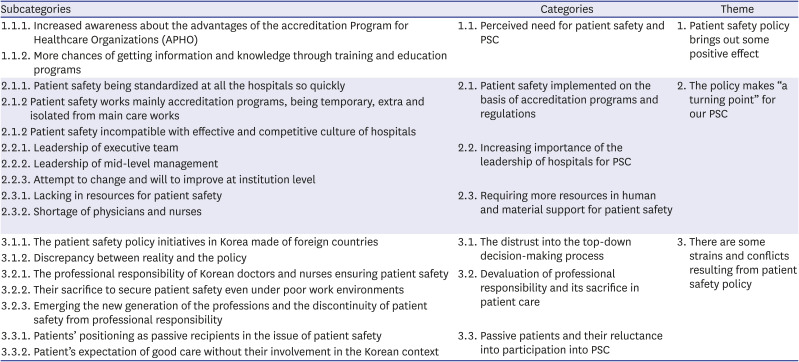
Table 2
General characteristics of participants
![]()
Table 3
Categories and subcategories that emerged from coding of data
![]()
Patient safety policy brings out some positive effects
Perceived need for patient safety and PSC
The majority of the participants felt that, in recent times, gradual changes were taking place owing to the active and enforced implementation of patient safety-related policies, activities, and education. Although there were some challenges with the implementation, it was said that positive changes had been brought about by enhanced patient safety. Participants reported that it was the preparation of the Accreditation Programs for Healthcare Organizations that established the patient safety-related systems at hospital level. Thereafter, different kinds of education and training programs, which were planned and delivered to members of hospitals including the participants, were given. They pointed out that they acquired a lot of knowledge and information about patient safety, which resulted in a change in their perception about patient safety. They seemed to be sure that such efforts were necessary to get attention to help patients, even as the workload increased considering these activities.
“Even though it is not totally ingrained... Perception is changing little by little... Even that would be a good thing.” (GH-P # 4)
“When things like that are emphasized, ultimately there are more steps and actions to go through… As you do those things, it tends to get better than not doing them.” (GH-N # 3)
The policy makes “a turning point” for the PSC
Patient safety implemented on the basis of accreditation programs and regulations
The participants stated that patient safety “culture” reminded them of common ground and values shared and practiced by all the members of the organizations. Similarly, they said the Accreditation Programs for Healthcare Organizations, which was necessary for patient safety and critical for hospitals to be considered safe, became the foundation for PSC so that they were encouraged to perform safe medical practices; additionally, their hospitals provided an environment to ensure patient safety. It was important that patient safety procedures and practices through the accreditation programs were standardized at all the hospitals at the same time, and that they were successfully implemented in hospitals without having a choice.
Meanwhile, the participants mentioned some limitations of patient safety through the accreditation programs. Mostly, they pointed out that safety-related activities were not integrated into the daily care routines at hospitals and so, safety was isolated and temporary, mainly working within the evaluation period of the Accreditation. For example, the participants expressed that although accreditation-related procedures and regulations exist, these are not implemented effectively. In particular, the formats tailored to meet the accreditation criteria were implemented only during the assessment period, after which things went back to being the way they were.
“The accreditation team actually came for an interim assessment. The fire doors were always blocked, but they were all opened during that time. Today, it is back to the way it was...” (TH-N # 3)
For the procedures and activities of the programs relating to culture, the participants stated that they dealt with the general character of the Korean culture, that is, “rush-rush mindset,” particularly with an emphasis on the “effective” and “competitive” culture at hospitals. They were concerned that those dominant characteristics of the culture would interfere with their efforts to establish PSC. The nurses expressed that the culture of “rush-rush” interfered with their attempts to perform patient safety activities for the patients, whereas the physicians pointed out that working in a culture that strives for proficiency, i.e., being unappreciative of good performance and being extremely critical of poor performance, was a challenge.
Increasing importance of the leadership of hospitals for PSC
Leadership becomes significant for patient safety. The participants expressed that while the perception of executives about patient safety had relatively improved, when compared to the pre-Accreditation period, it was insufficient, and that it was necessary for the hospital executive team to change their mindset. The nurses voiced that no matter how hard they tried, it was difficult to improve patient safety without a proper hospital environment and efforts on the part of the executive team. The physicians also emphasized that building awareness among the executive team was important because of the money and time needed to be invested into patient safety. The participants expressed that the leadership of the mid-level management, in addition to that of the executive team, was also important to establish PSC in the institution. They seemed to be important because they transform the ideas and willpower at the top level to practical and working plans at the bottom.
Requiring more resources in human and material support for patient safety
The majority of the participants mentioned that they needed more resources and support for patient safety. The patient safety-related activities, according to the participants, required the necessary human resources, related infrastructure, and financial support. The nurses emphasized the importance of financial support by describing their negative experiences, such as witnessing the discontinuity of good systems and patient safety-related equipment not being purchased owing to cost issues, and their positive experiences, such as new equipment being purchased after problems were pointed out following incidents. The physicians mentioned that patient safety needed to be improved through a proper reward system so that there is social awareness of patient safety, which deserved to be paid for their time and money.
“Supporting patient safety is very costly. No matter how much it is said that the barcode system is effective for patient safety, there is no barcode system in our hospital.” (TH-N # 6)
In addition, the participants expressed that the shortage of human resources, which was a chronic problem in the Korean context, put a lot of burden on the establishment of a PSC. The nurses noted that the frequent turnover and high number of patients per nurse were well known problems that needed resolution. In addition, they spoke about issues such as wage determination for staffing appropriate levels of personnel and recruitment of experienced nurses. The physicians also recognized their shortage in number as being challenges to the culture. There seemed to be significant differences in human resources and the supporting infrastructure by different types of hospitals; that is, the general hospital was hardly supported in terms of human and financial resources, and patient safety is more likely to be a blind spot.
There are some strains and conflicts resulting from patient safety policy
The distrust of the top-down decision-making process
The participants complained that most of the patient safety-related policies were implemented in a top-down approach. As a result, there were many difficulties and problems faced while applying them in real situations. Moreover, the additional tasks of having to record the patient safety-related activities increased administrative paper work, and the time spent on actual safety-related work was reduced. The participants expressed distrust in the healthcare policies and systems in South Korea. No policies that fit into the medical field and considered the consciousness of the medical personnel and the public has yet been prepared. However, some policies from other countries were benchmarked and applied to the Korean context, resulting in on-ground discrepancies.
“Safety should be the top priority, and that should be the culture... What I always recognize is that there is a significant discrepancy with reality.” (TH-P # 2)
“Hospitals and employees alike believe that hospitals are not that safe; everyone has to do a good job... Such an atmosphere or image already exists to a certain degree; but, under these circumstances and with this system, it will be difficult to show any more progress.” (TH-N # 2)
Devaluation of professional responsibility and its sacrifice in patient care
The participants stated that healthcare professionals in South Korea possessed a high level of job consciousness, ethical consciousness, and sense of responsibility. They had voluntarily made efforts at the individual level to enhance patient safety. Sometimes, they sacrificed their personal life for patient care, including patient safety, that was hardly appreciated at the organizational level. The situation worsened when they were exposed to excessive workload and staff shortage and they faced an overload of professional responsibility in a poor work environment.
Although the high level of professional responsibility was maintained for a long time in Korea, and partially ensured patient safety, there seem to be some changes that may occur when a new generation of healthcare professionals emerge. The participants stated that in the changing times, improvement in patient safety could not be brought about using the traditional way of forcefully demanding sacrifices from healthcare professionals. The nurses noted that with frequent resignations and high turnover, there was a shortage of moderately experienced nurses who could intervene and help reduce the gap between experienced and inexperienced nurses. The physicians voiced that the days of forcing a sense of responsibility and duty were over and the hierarchy within themselves had collapsed. They kept reiterating that it might be difficult to establish patient safety by forcing activities.
Passive patients and their reluctance to participate in a PSC
The participants emphasized that a PSC should not be limited to healthcare professionals but must include patients as well. They expressed that to build the culture, it would be necessary for patients to participate by taking ownership. Currently, they said there was a lack of awareness about patient safety among the patients. Considering this lack of awareness, they expressed that patients should also take ownership of patient safety. Through their lenses, patients seem to put themselves in a situation that made them passive recipients of care. They seem to want the physicians and nurses to know their name and symptoms in advance, without their involvement in the care. Additionally, they seem to think that good care, including patient safety, looks like parents’ love to children, where there is no room for their participation. It was understood that their reluctance to participate in patient safety came from the Korean culture called “jung,” which focused on affection without condition.
“No matter how well the healthcare professionals wash their hands and administer the medication, patients are still required to recognize how many germs they have and be aware of spreading their germs to others to ensure that patient safety culture takes place properly, which will result in a higher quality of healthcare.” (TH-N # 7)
“When I say ‘please state your name’ for the patient identification, they retort by saying you saw me yesterday and today and would see me again tomorrow, but you do not know my name? The Korean sense of ‘jung’.” (TH-N # 6)
Go to :
DISCUSSION
This study identified how healthcare professionals in South Korean hospitals perceive PSC at a time when patient safety-related policies are being rapidly introduced in the country. Based on the results, three themes and seven categories of perceptions about PSC were identified.
Farokhzadian et al.21 used the expression “the long way ahead of safety culture” to indicate that the path to integrating PSC in the organizational culture is long-winding, owing to the challenges associated with establishing PSC. In this study, more healthcare providers at hospitals agreed about the importance of patient safety than they did previously, and recognized some positive changes resulting from the implementation of the policies; however, not all members shared the same values and beliefs. In the early stages of developing patient safety systems, many changes may have taken place in a top-down way, mostly led by the government, and now the importance of patient safety is gaining importance in healthcare institutions.22 This study identified that the system might be distorted at the ground level. Systems and policies adopted at the national level influence PSC in healthcare institutions,23 and thus, policymakers and relevant government agencies must consider whether any policy can be implemented properly on the ground and ensure the engagement of frontline staff.
The healthcare professionals stated that the unique culture and characteristics of South Korea have an influence on PSCs. In particular, they expressed that it would be difficult to build a PSC in a work environment that prioritizes efficiency and believes in working in a “rush-rush” manner rather than complying with rules. Such social atmosphere affects the implementation of patient safety-related policies, and medical professionals face “sick system syndrome.” Therefore, countries that adopt patient safety-related laws and policies in the future need to verify the level of perceived PSC among medical professionals, as in the present study.
The culture within the occupation, such as the sense of responsibility that healthcare professionals bore,2425 was identified as an important element in PSC in this study. Moreover, the study also found that generational differences appeared with the changing times, and thus, a new approach was needed to build PSC. Additionally, leaders were identified as the entity that played a crucial role in building culture, similar to the previous studies that emphasized the role of leaders.212226 Insufficient human resources, excessive workload, and poor work environments were identified as factors that interfered with patient safety. Therefore, human and material support are essential for improving PSC.27
–
29 The perception and will of leaders who make decisions about support on patient safety significantly influence the perception and attitude of members.22
The participants revealed their hope to establish PSC and emphasized the patients’ efforts in the process, in addition to that of healthcare professionals and institutions. Patients need to play a central role in establishing and improving PSC.28 WHO emphasizes the involvement of patients and their families at every level of healthcare, from shared decision-making during care to policy-making and plans.9 Therefore, patient safety campaigns and educational programs targeting all South Korean citizens are needed.
This focus group study approached the PSC of South Korea with the emphasis on physicians and nurses who have 'learned' and 'experienced' in response to the national patient safety policy. It turned out that almost all the participants are long tenure workers in general hospitals or tertiary ones in the metropolitan areas. Additionally, they are mainly male physicians and female nurses, which exactly meets with the health care occupation-specific gender characteristics in South Korea. Despite its focus on the shared experiences responding to the policy, this study has some limitations to provide a general view on the PSC in South Korea because of not including the participants working in local and small hospitals. And the occupation-specific gender characteristics are not sufficiently recognized in the study enough to see how the gender context affects the participants' perceptions of the PSC. The studies following should consider the above limitations, and continue investigating the PSC in South Korea by expanding into the establishment stage of the policy from the early one in this study.
This study’s findings are helpful not only for building PSC in healthcare institutions but also as reference material at the government level during the execution of patient safety-related policies. Moreover, it is necessary for countries planning to adopt new patient safety-related policies to account for actual clinical settings and sufficiently communicate with people who will actually perform the actions mentioned in the policies, to allow the policies to be effectively implemented. Improving patient safety and establishing PSC require a multipronged approach that include not only voluntary efforts on the part of healthcare professionals but also active participation by patients, the introduction of appropriate activities at the institutional level, and government support.
Go to :
 XML Download
XML Download