

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vitiligo is an acquired and multifactorial pigmentation disorder with a complex pathogenesis that is not clearly elucidated. Various hypotheses have been proposed for the pathogenic mechanisms of vitiligo, but the most important hypothesis is thought to be the autoimmune mechanism. Vitamin D is synthesized in the skin and affects by binding a nuclear hormone receptor called the vitamin D receptor (VDR). VDRs are present in cells related to calcium and bone metabolism, as well as in other cell types such as keratinocytes, melanocytes, fibroblasts, and immune-related cells of the skin.1 Recent studies have shown that vitamin D has an immune-protective effect. The role of vitamin D deficiency and VDR gene polymorphisms has been established in many autoimmune diseases, including vitiligo, but the results are still controversial.12 In this study, we investigated the association between 25(OH)D levels, VDR gene polymorphisms, and vitiligo in Korean patients.
Go to : 
METHODS
Subjects
The study enrolled 172 patients with vitiligo who visited to the Dermatology Department of Kyung Hee Medical Center (Seoul, Korea) between June 2012 and October 2017. Vitiligo was diagnosed based on patient history and clinical evaluation. Patients with a history of phototherapy, vitamin D supplementation, other autoimmune diseases, or a history of smoking were excluded from the study. Data on vitamin D levels in healthy controls were collected from the Korea National Health and Nutrition Examination Survey (KNHANES) conducted in 2013.
For the analysis of the VDR gene polymorphism, 130 patients with non-segmental vitiligo (NSV) were enrolled. In addition, 453 age- and sex-matched controls from dermatology outpatients attending the same department were included in the study.
Clinical assessments
We collected data on age, sex, 25(OH)D level, duration, type of vitiligo, thyroid autoantibodies, family history, and the affected body surface area of 172 patients with vitiligo. Serum 25(OH)D levels were measured using the LIAISON 25 OH Vitamin D TOTAL Assay (DiaSorin, Saluggio, Italy), which employs a chemiluminescent immunoassay technology for the quantitative determination of the 25(OH)D levels in the human serum and plasma.
DNA extraction and genotyping
The peripheral blood samples were collected in tubes coated with ethylene-diamine-tetraacetic acid, and genomic DNA was obtained by using Roche DNA extraction kit (Roche, IN, USA). We used the Customer Axiom Exome Array by Affymatrix (Affymatrix, CA, USA) to genotype the selected SNPs. The experimental process was conducted by Theragen (Suwon, Korea).
Design of the customized DNA chip
We selected VDR genes from the NCBI gene database (https://www.ncbi.nlm.nih.gov/gene) and manually searched for all known SNPs in all the selected genes using the dbSNP database (https://www.ncbi.nlm.nih.gov/snp/). The exon and promoter regions were considered as candidate SNPs. Candidate SNPs were selected according to the following criteria: 1) SNPs located in the exon and promoter regions of each gene; 2) SNPs studied in previous GWASs or case and control studies with various diseases; 3) SNPs reported in Asians; 4) SNPs with > 10% minor allele frequency in Asians; and 5) > 0.1 heterozygosity. Finally, a customized chip was designed on the basis of these criteria.
Statistical analysis
An independent samples t-test was used to compare the mean vitamin D levels between the patients and the mean serum value of the Korean population. The significance level for the statistical tests was set at P < 0.05. For the analysis of VDR gene polymorphism, a chi-square test was performed to test the Hardy-Weinberg equilibrium (HWE) in the control group. Logistic regression models were used to analyze the relationship between each SNP and the susceptibility to NSV. The models were log-additive, dominant, and recessive. Odds ratios (ORs), 95% confidence intervals (CIs), and P values were determined. All statistical analyses were performed using SNPStats (http://bioinfo.iconcologia.net/index.php?module=Snpstats). This was tested at a significance level of 0.05.
Ethics statement
The present study protocol was reviewed and approved by the Institutional Review Board of Kyung Hee University Medical Center (approval No. 2016-07-059). Informed consent was waived because of the retrospective nature of the study.
Go to :
RESULTS
Analysis of the serum 25(OH)D levels in vitiligo patients
The characteristics of 172 subjects with ages ranging from 3 to 85 years (mean, 40.96 ± 22.22 years) and the mean serum 25(OH)D levels are listed in Table 1. The mean serum 25(OH)D level in the 172 patients with vitiligo and KNHANES (2013) was 18.75 ± 0.60 ng/mL and 17.28 ng/mL, respectively. The mean serum 25(OH)D level in vitiligo patients was not significantly different from the mean serum value of the Korean population (P = 0.087).
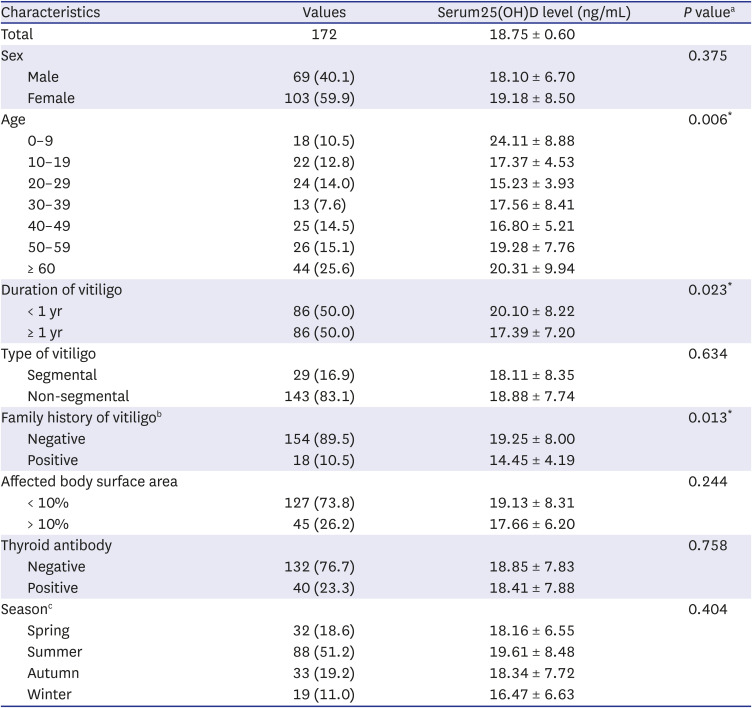
Table 1
Serum 25-hydroxyvitamin D levels (ng/mL) according to clinical features and laboratory findings
Values are presented as number (%).
aA P value < 0.05 is considered statistically significant; bFamily history includes first-degree relatives (parents, siblings, and children); cSpring is from March to May. Summer is from June to August. Autumn is from September to November. Winter is from December to February.
![]()
We also compared the mean serum 25(OH)D levels in patients with vitiligo according to the clinical features and laboratory findings (Table 1). There were no significant differences in the mean serum 25(OH)D levels according to sex, type, affected body surface area, thyroid antibody, and season. However, there were significant differences in the mean serum 25(OH)D levels according to age, duration, and family history of vitiligo. Serum 25(OH)D levels were significantly lower in the group who had vitiligo for at least 1 year compared with the group who had less than 1 year. In addition, the serum 25(OH)D levels were significantly lower in patients with a family history of vitiligo than in those without.
Genotypic frequencies in patients with NSV and unaffected controls
The genotype distributions of 37 SNPs of VDR gene in the control group were in HWE (P > 0.01, data not shown). The distribution of genotypic frequencies for each SNP is shown in Table 2. Among the 37 SNPs, four SNPs (rs2239186, rs4760648, rs4237855, and rs7299460) were statistically associated with NSV. We observed a difference in the genotype frequencies of rs2239186 in the dominant model (OR = 1.89, 95% CI = 1.10–3.23, P = 0.017), rs4760648 in the recessive model (OR, 0.54; 95% CI, 0.30–0.96; P = 0.029), rs4237855 in the log-additive and dominant model (OR, 0.67; 95% CI, 0.49–0.92; P = 0.012, log-additive model; OR, 0.56; 95% CI, 0.36–0.86; P = 0.009, dominant model), and rs7299460 in the recessive model (OR, 1.69; 95% CI, 1.03–2.76; P = 0.041). However, these associations were not significant after the Bonferroni correction.
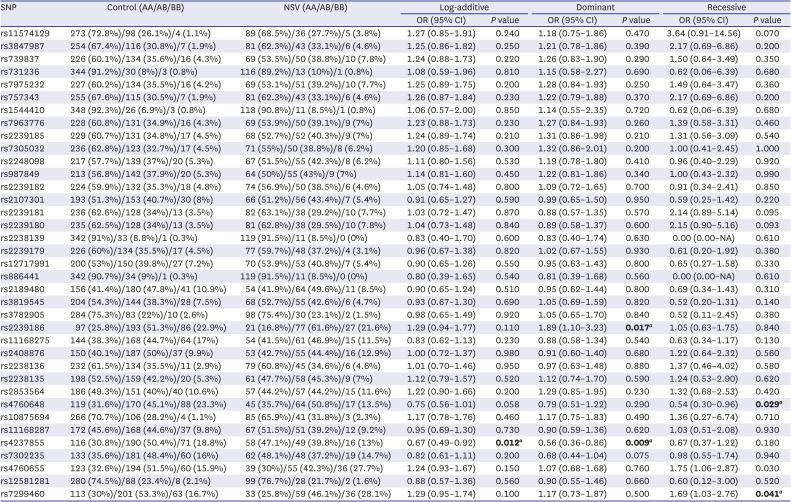
Table 2
Distribution of genotypes and allele frequencies of the VDR polymorphism in the vitiligo and control groups
VDR = vitamin D receptor, NSV = non-segmental vitiligo, OR = odds ratio, CI = confidence interval.
aA P value < 0.05 is considered statistically significant.
![]()
Go to :
DISCUSSION
Our understanding of the immunomodulatory effects of vitamin D continues to grow.2 Although there is in vitro and animal evidence that vitamin D can prevent autoimmune disease in humans, the data to support this hypothesis are still lacking.2 Despite the multitude of cross-sectional and case-control studies that demonstrate lower levels of vitamin D among individuals with autoimmune diseases, such as inflammatory bowel disease, multiple sclerosis, systemic lupus erythematosus, type I diabetes mellitus, and rheumatoid arthritis, compared to healthy controls, these studies are not able to address clear causality.23 Several previous studies have shown that 1,25(OH)2D3 inhibits the maturation and differentiation of dendritic cells, T-cell proliferation, and Th1 cytokine secretion. In addition, 1,25(OH)2D3 may increase the number of regulatory T cells and enhance the secretion of interleukin (IL)-10.4
The role of vitamin D in vitiligo remains unclear despite the presence of several studies attempting to explain it. Koizumi et al.5 have shown that vitamin D can exert immunomodulatory effects by inhibiting the expression of proinflammatory and proapoptotic cytokines, such as IL-6, IL-8, TNF-α, and TNF-γ, which can cause vitiligo. Sauer et al.6 reported that 1,25(OH)2D3 was shown to inhibit the apoptosis of human melanocytes through the formation of sphingosine-1-phosphate. In addition, there have been attempts to use topical vitamin D for the treatment of vitiligo. In one study, calcipotriol may stimulate melanin production by activating the melanocytes and keratinocytes.7
There have been a few previous studies examining the vitamin D levels in vitiligo, and the results have been controversial. Khurrum et al.8 reported that there was no difference in the vitamin D levels between the vitiligo patients and the control subjects. In contrast, Upala et al.9 identified a significant relationship between low 25(OH)D levels and vitiligo. In our study, the mean serum level of 25(OH)D in 172 vitiligo patients was not significantly different from the mean serum value of 25(OH)D in the normal Korean population. Alshiyab et al.10 reported that there was no significant difference in the levels of vitamin D between patients with vitiligo and healthy controls in Jordan. The serum levels of 25(OH)D were significantly lower in the group who had vitiligo for at least 1 year compared with the group who had vitiligo for less than 1 year. The lower 25(OH)D levels in patients with a longer disease duration may be explained by its consumption in chronic autoimmune inflammatory processes beyond the endogenous synthesis of vitamin D in the skin.6 It may also be possible that patients with vitiligo had been advised to avoid exposure to sunlight. In addition, the serum levels of 25(OH)D were significantly lower in the group with a family history of vitiligo than in the group without. A similar finding was observed by Sobeih et al.11, who found a significant negative correlation between serum 25(OH)D levels and the presence of a family history of vitiligo in an Egyptian population.
VDR gene polymorphisms affect the expression and function of VDR. Previous studies have shown an association between vitiligo and VDR polymorphisms. Birlea et al.12 detected an association between VDR-Apa I polymorphism and vitiligo. In a meta-analysis by Zhang et al., 13 it was suggested that VDR Apal locus increased the risk of patients with vitiligo. In another study, Aydingoz et al.14 observed that VDR TaqI gene polymorphisms and the haplotype BsmI/ApaI/TaqI/FokI/Cdx2 GCCCG may be a novel risk factor for vitiligo. In this study, the association between 37 SNPs of VDR gene including these polymorphisms and vitiligo was analyzed. There were no significant differences in the genotypic distributions of the VDR gene between patients with vitiligo and healthy controls. These results suggest that SNPs of the VDR gene do not contribute to the development of NSV in Korean patients with vitiligo.
In conclusion, there was no significant difference in the serum vitamin D levels. Furthermore, there were no significant differences in the VDR polymorphism between vitiligo patients and the normal control group. However, the small sample size was a limitation of this study. Further studies are needed to establish the relationship between serum vitamin D levels and vitiligo in individual patients.
Go to :
 XML Download
XML Download