

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which started in Wuhan, China, in December 2019, has been declared as a pandemic. COVID-19 is one of the deadliest infectious diseases that have emerged in recent history and continues to affect all countries worldwide.1 With the efforts of many researchers to eliminate the current pandemic, various characteristics of COVID-19 are being investigated. The distinctive difference between COVID-19 and other emerging infectious diseases is the presence of contagious asymptomatic infections, which have become widespread in the community, resulting in a pandemic.234 As soon as the novel coronavirus was identified, each country adopted various policies to prevent the import of COVID-19 abroad.5 Since the first confirmed case in Korea on January 20, 2020, the epidemic has rapidly spread in Korea, and policies such as the daily use of face masks, social distancing, and self-isolation for travelers from abroad have been legally stipulated and are still in progress.
Approximately 20% of COVID-19 cases progress to severe respiratory failure, with an overall mortality rate of 2.3%.6 In other studies, one-third of hospitalized patients were diagnosed with acute respiratory distress syndrome, and the in-hospital mortality rate reached 60% in New York at the early stage of the epidemic.78 Older age, male sex, and comorbidities including hypertension, diabetes, cardiovascular disease, chronic pulmonary disease, chronic kidney disease, cancer, and chronic liver disease were associated with increased susceptibility to SARS-CoV-2.7910 The proportion of asymptomatic patients was high among individuals aged > 80 years. Considering that the incidence of severe COVID-19 is high among older adults and many nursing hospital clusters in Korea have several older patients, the rate of disease transmission by asymptomatic patients may be high. Infectivity of SARS-CoV-2 is also reported to be associated with the variants.1112 Omicron (B.1.1.529) and delta variants (B.1.617.2) are related to higher infectivity than alpha (B.1.1.7), beta (B.1.351), and G614 (B.1) variants early in the emergence of variants of concerns.1314
Data on the infectivity of COVID-19 are limited. Considering that human-to-human transmission occurs even in asymptomatic patients and the median intubation period is 5 days,3 studies on the infectivity of COVID-19 are warranted to control the outbreak. Previous studies have reported that asymptomatic patients may have lower infectivity than symptomatic patients.1516 The major limitation of studies on the infectivity of COVID-19 is that it is difficult to investigate all infected patients. Hence, in this study, we aimed to evaluate the infectivity of patients diagnosed with COVID-19 using real-time polymerase chain reaction (RT-PCR) through a total investigation conducted in Gyeonggi-do, the largest province in Korea.
Go to : 
METHODS
Study design and population
In this prospective cohort study, we analyzed the infectivity of SARS-CoV-2 in Gyeonggi Province, Korea, from January to April 2020. Since the first detection of the confirmed case on January 20, 2020, Korea has been managing all confirmed patients and monitoring the close contacts of these patients. The monitoring and management program is structured and unified at the national level, and all close contacts are structurally classified into self-isolation, active monitoring, and passive monitoring groups according to their contact point and degree of protection; all these individuals were scheduled to undergo RT-PCR testing. This study analyzed the dynamics of transmission, including the infectivity of COVID-19 based on the total data including those of asymptomatic patients and contact data of confirmed patients in Gyeonggi Province, the largest province in Korea.
Definition
Confirmed COVID-19 patients were defined as individuals whose respiratory tract specimens tested positive for SARS-CoV-2 on RT-PCR. When the patients were diagnosed with COVID-19, the route of movement from 2 days before the onset of symptoms to the date of diagnosis was reported, and the investigators conducted contact tracing based on this report. All close contacts of confirmed COVID-19 patients underwent PCR for the detection of SARS-CoV-2 and were classified into close contact, active monitoring, and passive monitoring groups depending on the degree of contact. Secondary confirmed patients were described as close contacts with positive PCR results. The secondary attack rate (SAR) was defined as the ratio of secondary confirmed patients with positive PCR results among the close contacts, according to the World Health Organization guidelines.17
Data collection
The data collected from all patients with confirmed cases were as follows: age, sex, date of diagnosis, date of symptom onset, comorbidity (including hypertension, diabetes, heart failure, asthma, chronic obstructive pulmonary disease, chronic kidney disease, chronic liver disease, hematologic disease, and dementia), symptoms at the time of confirmation or for the entire disease course (including fever, chills, cough, sputum, dyspnea, sore throat, rhinorrhea, myalgia, headache, loss of consciousness, nausea, vomiting, diarrhea, abdominal pain, chest pain, loss of smell, and loss of taste), the cycle threshold (Ct) value of SARS-CoV-2 PCR of respiratory tract specimens performed at and after the date of diagnosis, blood tests (hemoglobin, white blood cell count with differential, platelet count, liver function test, renal function test, C-reactive protein [CRP], and procalcitonin), administration route and amount of oxygen during oxygen therapy, and the status of mechanical ventilation or extracorporeal membrane oxygenation.
Statistical analysis
For comparison, Pearson’s χ2 tests and Fisher’s exact tests were used for categorical variables, while Student’s t-test and Mann-Whitney U tests were used for continuous variables, as appropriate. Spearman’s correlation was used to evaluate the relationship between two continuous variables. Multiple regression analysis was used to analyze the relationship between the variables and infectivity of COVID-19. The risk ratio is method to compare the risks for the two groups. Simply divide the cumulative incidence in exposed group by the cumulative incidence in the unexposed group. In this study calculated risk ratio and confidence intervals (CIs) based on null hypothesis (risk ratio equals to 1) testing. All statistical tests were two-sided with an α level of 0.05. All CIs were 95%. All statistical analyses were performed using R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) and the fmsb package.1819
Ethics statement
The study was approved by the Institutional Review Board of the Korea University Ansan Hospital (No. 2020AS0108). Written informed consent was obtained from all participants.
Go to :
RESULTS
Of the 502 patients, 298 were included in the study, while 388 without additional contact to the study population were excluded. These 298 patients were divided into 106 clusters with 5,909 contacts. The largest cluster consisted of 29 patients, with 40 contacts. Of the total cases, 92 were imported from abroad, while the remaining 206 were domestic cases. In case of domestic infection, the places of exposure were health care facilities (n = 60), religious gatherings (n = 53), workplaces (n = 28), schools (n = 5), and gym and fitness centers (n = 3), while 40 patients were unable to determine the origin of transmission. Eleven cases were confirmed to have been introduced from Daegu, the region where the first wave of COVID-19 in Korea. The baseline characteristics of the study population are shown in Table 1. A total of 127 patients (42.6%) were men, and the median age was 46 years (interquartile range [IQR], 30–58). Of the total patients, 114 (38.3%) had one or more underlying diseases, and the most common diseases were hypertension and diabetes, in the order of frequency. A total of 254 patients (85.2%) developed one or more symptoms at the time of diagnosis, while 277 patients (93.0%) developed symptoms at any period after the date of diagnosis. The mean duration of symptoms before diagnosis among symptomatic confirmed patients was 4 days (IQR, 3–8). The most common symptoms were cough, fever, sputum, sore throat, and headache, in the order of frequency. The median baseline Ct values of the upper and lower respiratory tract specimens at the time of diagnosis were 27.4 and 25.5, respectively. The median CRP and procalcitonin levels at the time of diagnosis were 0.23 mg/dL and 0.03 µg/mL, respectively. Ninety-four patients (31.5%) developed pneumonia, while eight (2.7%) died during the follow-up period.
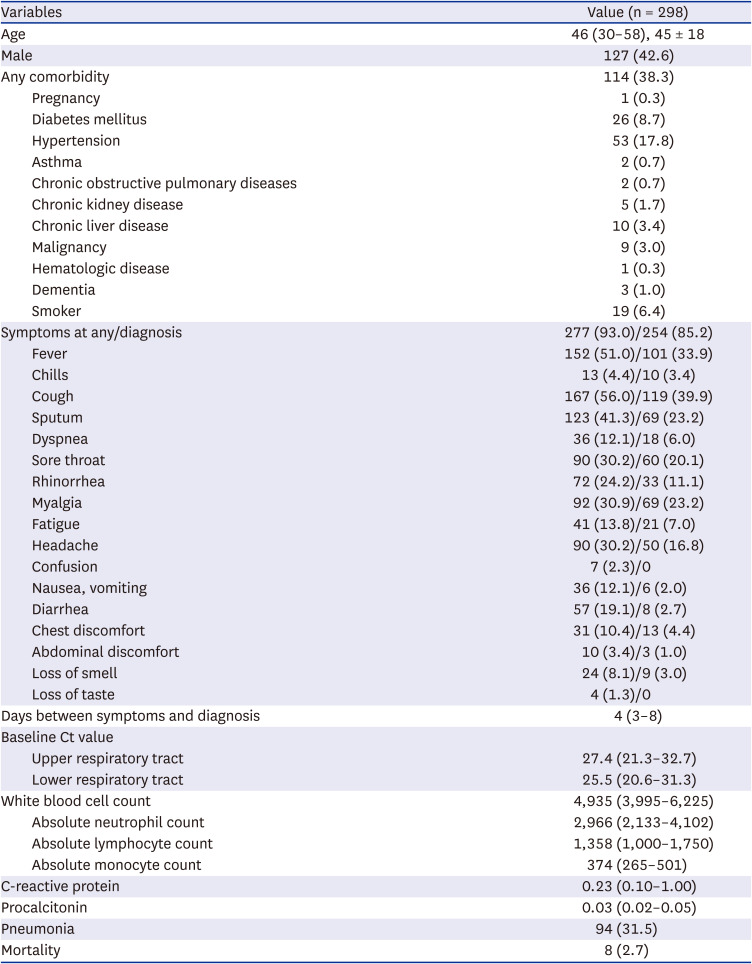
Table 1
Baseline characteristics of the study population
Data are expressed as number (%) or median (interquartile range), unless otherwise indicated.
Ct = cyclic threshold.
![]()
SAR of the overall study population was 3.5% (204/5,909). None of the 238 patients with 3,257 contacts developed secondary infection. In the cluster where the second confirmed case occurred, SAR varied, and the highest SAR was 68% (15/22), except in one exposed and confirmed patient. This cluster was from abroad, and the index case was a 46-year-old symptomatic woman who complained of cough, dyspnea, and fatigue. At the time of diagnosis, she was diagnosed with pneumonia, and the Ct values of the upper and lower respiratory tract specimens were 25.32 and 19.87%, respectively. Of the seven clusters with more than 100 contacts, two clusters showed high SAR, 44% and 7.6%, respectively. The cluster with 44% SAR acquired COVID-19 after attending a religious gathering; the index case was a 73-year-old symptomatic woman who complained of fever, cough, and headache at the time of diagnosis, and the Ct values of the upper and lower respiratory tract specimens at diagnosis were 15.03 and 14.41, respectively. The second cluster with a SAR of 7.6% acquired COVID-19 in the hospital, and the index case was an 81-year-old symptomatic patient with lung cancer. He complained of fatigue and pneumonia accompanied by hospitalization. The initial Ct values of upper and lower respiratory tract specimens at the time of diagnosis were 18.88 and 13.91, respectively. The patient died 6 days after the diagnosis.
Table 2 shows the secondary clinical attack rates for COVID-19 by different exposure settings. In all cases, secondary clinical attack rates were the highest in the order of religious gathering (13.5% [95% CI, 10.7–16.8%]), workplaces (8.49% [95% CI, 6.08–11.74%]), school (6.38% [95% CI, 3.39–11.69%]), inflow from abroad (2.12% [95% CI, 1.50–2.97%]), and health care facilities (1.92% [95% CI, 1.45–2.55%]). For symptomatic cases, religious gathering (15.7% [95% CI, 12.4–19.7%]), workplaces (8.84% [95% CI, 6.33–12.21%]), and school (6.38% [95% CI, 3.39–11.69%]) showed high secondary clinical attack rates. All cases at workplaces and school have complained any symptoms. There were no cases among those exposed at gym and fitness centers. Secondary clinical attack rates in healthcare facilities showed lower risk ratios in both symptomatic and asymptomatic subjects compared to the other exposure settings. As a survey at the beginning of the epidemic, the inflow rate from Daegu, the area where the first wave of COVID-19 spread in Korea, was 4.7% (95% CI, 2.64–8.22%).
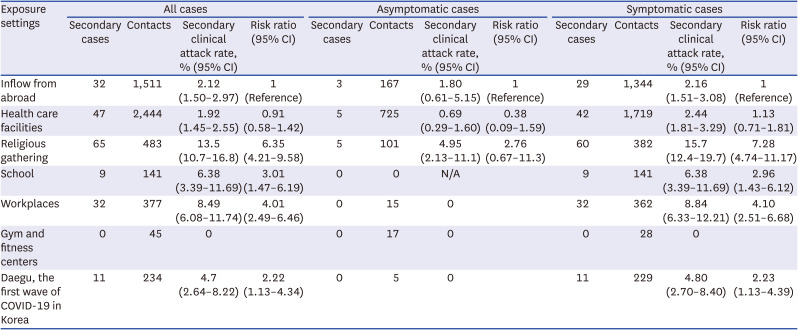
Table 2
Secondary clinical attack rates for COVID-19 by different exposure setting
![]()
The analysis of variables associated with high infectivity based on the secondary infection rate is shown in Table 3. Among the symptoms, sore throat at any period (β = 0.130, P = 0.024), dyspnea at diagnosis (β = 0.126, P = 0.030), and dyspnea at any period (β = 0.123, P = 0.033) were associated with increased infectivity. Laboratory findings showed that lower Ct values in lower respiratory tract samples (β = −0.353, P = 0.026) were associated with higher infectivity, and leukopenia (β = −0.115, P = 0.048) and lower bilirubin levels (β = −0.120, P = 0.041) were associated with lower infectivity. In addition to the presence of symptoms, age, sex, comorbidity, fever, cough, and pneumonia were not significantly correlated with infectivity in this study.
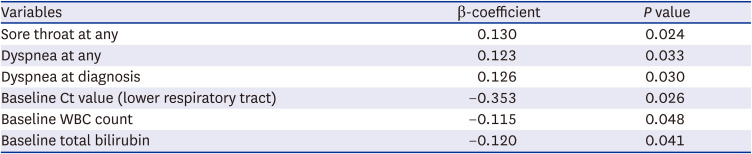
Table 3
Factors associated with infectivity of COVID-19 disease
![]()
Go to :
DISCUSSION
This study is significant as it analyzed the variables affecting the infectivity of COVID-19, including all asymptomatic patients. The variables associated with high infectivity in this study were sore throat during the disease period, dyspnea at diagnosis and during the disease period, lower Ct value at diagnosis, leukocytosis, and higher bilirubin level at diagnosis. Previous studies regarding the infectivity of SARS-CoV-2 reported that symptomatic patients were more infectious than asymptomatic patients, and high-risk groups for COVID-19 diseases, and the period of viral transmission.162021
In previous studies on SARS-CoV-2, high viral copy numbers have been associated with high viral loads and culturability.22 The Ct value in SARS-CoV-2 RT-PCR was correlated with the positivity rate of the virus culture.23 However, the cut-off Ct value associated with culture positivity is unknown, and not all cases with positive RT-PCR results are transmissionable. The results of RT-PCR test may be positive for more than 21 days, and the viral load detected in urine, saliva, and stool samples may be equal to or higher than that detected in naso/oropharyngeal samples.242526 In symptomatic COVID-19 patients, viral shedding has been reported to occur over a median of 4 days based on virus culture.23 In other studies, SARS-CoV-2 was detected in up to 8–9 days in virus culture after the onset of symptoms.2728 No difference was observed in the positive rate of viral culture between symptomatic and asymptomatic patients. The virus culture rate decreased to 6% when the Ct value was > 35. Another study reported that when the Ct value was 13–17, the virus culture test showed positive results; when the Ct value increased to 33, the culture showed a positive rate of 12%; and when the Ct value was ≥ 35, the virus culture test showed negative results.29 RT-PCR can show low genome copy numbers of specimens with negative culture; therefore, assessment of the infectivity of COVID-19 based on the results of RT-PCR is limited.22
Dyspnea is related to the high infectivity of COVID-19. Dyspnea is a subjective symptom induced by inflammation in the respiratory tract, stimulation of sensory receptors, and hypoxemia caused by alveolar involvement.30 The characteristic finding in COVID-19 patients is silent hypoxia or apathetic hypoxia, although the mechanism has not yet been clearly identified, but it is presumed to be an idiosyncratic effect on the respiratory control system during the course of infection.3132 Thus, dyspnea may reflect advanced hypoxia and the association between severity and infectivity. In addition, patients with dyspnea may more likely spread the virus because they produce more droplets and aerosols during deep breathing or removal of face masks than patients without dyspnea.
Sore throat was associated with high infectivity in the present study. Sore throat is one of the most common symptoms of upper respiratory infection and has a low specificity for distinguishing pathogens such as viruses or bacteria. Although it remains unknown when sore throat occurs during the development of COVID-19, it may be the first sign of the disease or often occurs during the early stage of upper respiratory tract infection.33 Sore throat may reflect the higher transmission of droplets in the early phase of COVID-19 accompanied by upper respiratory tract infection.
As in previous studies, low Ct values of lower respiratory tract specimens and high infectivity were associated with COVID-19. Patients with higher viral loads are more contagious based on results of culture tests; in most cases, SARS-CoV-2 loses its infectivity as the viral load decreases over time.2229 Although not all COVID-19 patients are tested at the same phase of the disease and are immediately diagnosed with COVID-19, it is difficult to assume that the high Ct value of the first PCR test indicates that the COVID-19 patients are not contagious. Low Ct values affecting high infectivity in this study may be interpreted as a variable related to severity. The Ct value of the upper respiratory tract sample did not show any correlation with infectivity; this finding seems to be related to the reliability of the test due to the process of upper respiratory tract sample collection.
Leukocytosis and elevated bilirubin levels were associated with high infectivity among blood tests. In previous studies, leukocytosis and lymphopenia were related to the severity of COVID-19, caused by the destruction of lymphatic tissue and lymphocyte apoptosis due to direct lymphocyte infection, which is not a specific feature of COVID-19.3435 Leukocytosis has been linked to high rate of hospitalization (24–30%) among COVID-19 patients with pneumonia.36 In addition, leukocytosis is associated with the severity and poor prognosis of COVID-19.34 In the case of bilirubin, previous studies reported that more severe COVID-19 patients have higher bilirubin levels.37 No study has reported that higher bilirubin levels are associated with high infectivity; however, increased bilirubin levels could also be considered as an indicator of severity.
SAR was analyzed according to the exposure settings in this study. The group with the highest SAR was religious gathering, which reflected the situation at the beginning of the COVID-19 epidemic in Korea. SAR in healthcare facilities was lower compared to other exposure settings including religious gathering, workplaces, and schools. This result is similar to the previous research, which can be inferred that unprotected close contact increases the risk of transmission.20 Considering the majority of patients in the study population were unvaccinated, nonpharmacological interventions such as mask wearing, social distancing, and hand hygiene may influence interpersonal transmission in addition to vaccination.
This study analyzed the factors affecting the infectivity of COVID-19 in all confirmed patients in Gyeonggi-do, the largest province in Korea, which manages the entire database of COVID-19 diseases. The advantage of this study is that all confirmed patients, including asymptomatic individuals, were investigated within a certain period in the largest province in Korea. All clusters and potential confounding factors were considered to minimize the bias. This study has some limitations. Adherence to non-pharmacological interventions such as wearing of face masks and social distancing was not monitored; the effects related to the variables cannot be completely excluded. However, during the early stages of the COVID-19 epidemic, although the epidemiological characteristics of the disease were not clear and the preventive effects of the mask were controversial, the public implemented infection control policies, including wearing of face mask, hand hygiene, and social distancing in Korea. One study reported a compliance rate of 94% in terms of wearing masks in Korea.38 Another limitation is that the study period covers wild-type virus before the emergence of the variants of SARS-CoV-2 and did not reflect the epidemic status of the variants. Further studies on the infectivity that reflects the characteristics of the variants of SARS-CoV-2 may be necessary.
In conclusion, the variables related to higher infectivity in COVID-19 were sore throat, dyspnea, low Ct value in the lower respiratory tract specimens, leukocytosis, and higher bilirubin levels. These variables may also be an indicator of infectivity reflecting severity, given that previous studies have reported low infectivity in asymptomatic patients. With regard to the control of SARS-CoV-2 spread, implementation of strategies that can determine highly contagious factors during contact tracing and surveillance may be required.
Go to :
 XML Download
XML Download