

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cardiovascular diseases (CVDs) account for a significant portion of medical costs and are responsible for around one-third of mortalities worldwide.1 In Korea, CVDs have become the second leading annual cause of death since 2015.2 Most CVDs can be prevented and managed by correcting behavioral risk factors, such as cigarette smoking, harmful use of alcohol, unhealthy diet, and sedentary lifestyle.3 Cardiac rehabilitation (CR) is a secondary prevention program that has been proven to promote the quality of life, improve exercise capacity, reduce rehospitalization rate, and even improve survival rates for patients with CVD.45
Since the introduction of a multidisciplinary program for the comprehensive rehabilitation of acute cardiac patients by Hellerstein in the 1950s,6 CR based on structured exercise has been developed. In the United States, which has been leading CR, patients’ participation varies among states but is reported to range from 10% to 30%,78 and the government is trying to raise the participation rate to 70% through the Million Hearts® program.9
Although CR for the patients with CVD was reimbursed by the National Health Insurance Service since February 2017, it is thought that the dissemination in the clinical field remains very insufficient.10 No plans have been proposed to raise the participation rate of CR in Korea.
Several social, psychological, personal, occupational, and medical factors can hinder CR participation;1112 hence, appropriate strategies are required to overcome these problems. Since the major barrier to CR participation is the poor transportation accessibility of specialized hospitals, community-based CR may be an ideal alternative, as it utilizes regional medical and public health management institutions with good accessibility and flexible operational time.13
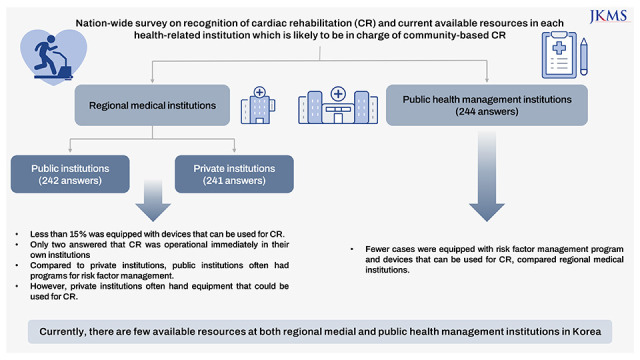
Therefore, we assessed the practicality of community-based CR by investigating the current status of regional medical and public health management institutions in Korea.
Go to : 
METHODS
Development of surveys
Internet-based, in-depth, nationwide surveys were conducted. The surveys were created based on the Global Survey of Cardiac Rehabilitation developed by Dr. Sherry Grace of the Cardiovascular Prevention and Rehabilitation Program, University Health Network, University of Toronto with the developer’s approval.14 The researchers modified the questionnaire according to the situation in Korea, and two questionnaires, one each for regional medical institutions and public health management institutions was developed. The questionnaires included questions on whether the necessary resources for operating CR were available, including management programs for risk factors of CVDs, equipment, facilities, and personnel, and whether they were willing to take charge of CR. In addition, the surveys asked what each institution deemed necessary for them to implement CR, why it would be difficult to operate CR, and what support they believed would be necessary.
Subjects of surveys
Regional medical institutions (where cardiologists, physiatrists, and cardiac surgeons who are authorized to prescribe CR worked) were selected, and questionnaires were distributed to these authorized doctors and director of each institution. The institutions were selected using data disclosed by the Health Insurance Review & Assessment Service. The candidate institutions were 1) secondary general hospitals, provincial medical centers, local hospitals, and clinics that do not perform percutaneous coronary intervention (PCI); 2) rehabilitation hospitals where two or more physiatrists work; 3) approved regional rehabilitation hospitals and convalescent rehabilitation hospitals; and 4) hospitals or clinics equipped with a physical therapy room. Hospitals unrelated to CVDs, such as specialized institutions for the spine, joints, orthopedics, psychiatry, gynecology, and cancer, were excluded. General hospitals with no cardiologists, physiatrists, or cardiac surgeons were excluded from the study, also.
In addition, public health centers and health center county hospitals were also included as regional medical institutions. For these institutions, questionnaires were sent to the head of each institution and personnel in charge of community care.
Public health management institutions, such as health living support centers, public sports facilities, welfare centers, and community centers, were also included. The questionnaires were sent to the head of each institution and the personnel in charge of life sports. Institutions without exercise equipment, senior citizens’ centers, welfare centers for people with disabilities, county offices, and private gymnasiums were excluded from the investigation.
Dispatch and collection of surveys
A total of 14 institutions, including two university hospitals in Seoul, a secondary general hospital in northwestern Gyeonggi-do, and 11 Regional Cardiocerebrovascular Centers, located across all regions of Korea participated in the survey. Printed questionnaires, project information, and an explanation of how to respond to the survey were sent on June 22, 2020. An official letter of cooperation from the Korean National Institute of Health was included to increase the response rate. The survey responses were gathered in Google survey format that was accessible through a QR code provided with the package or by connecting to www.crsurvey.co.kr. Responses were received until September 15, 2020. In some cases, responses were received by mail, at the convenience of the respondents.
Statistical analysis
Regional medical institutions were divided into public institutions that are officially operated by the government and private institutions. The differences between the two types of institutions were analyzed using the χ2 test. SPSS Ver. 23 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.
Ethics statement
Approvals from the Institutional Review Board were acquired from National Health Insurance Service Ilsan Hospital (approval No. 2020-04-011-005) and each of the other thirteen institutions. The need for informed consent was waived owing to the non-clinical nature of the study. Personal information, such as the responder’s sex, name, and address, was not collected; thus, participant anonymity was maintained.
Go to :
RESULTS
A total of 2,267 questionnaires were sent to 1,186 institutions. There were 420 private regional medical institutions, 245 public medical institutions, and 521 public health management institutions. A total of 241 and 242 responses were received from 173 regional private and 179 reginal public medical institutions, respectively. In total, 244 responses were gathered from 180 public health management institutions 44.9% of candidate institutions responded, whereas 32.1% of surveys dispatched received a reply (Table 1). Some (forty-four) answers from regional public medical institutions replied to the questionnaire meant for public health management institutions. However, as some items were identical in both questionnaires, from these answers that were obtained, the common items were extracted and analyzed even in these cases.

Table 1
The number of institutions and questionnaires were investigated
![]()
Current status of regional medical institutions
Programs for risk factor management, such as smoking cessation education, nutritional counseling, and exercise training program were provided at a higher rate in public medical institutions than in private institutions. However, electrocardiogram (ECG) monitoring during exercise is available at a higher rate in private institutions. Both types of institutions reported having less than 15% of the required equipment for CR program operation, such as exercise tolerance test, ECG, or blood pressure (BP)/heart rate (HR) monitoring during exercise. Exercise therapy rooms and devices for aerobic exercise were provided at a higher rate in private institutions. Basic programs to operate CR are more available in public institutions, whereas equipment is more available in private institutions, showing discrepancies between the two types of institutions. The defibrillators required for emergencies were provided at a very high rate in both institutions (Table 2).
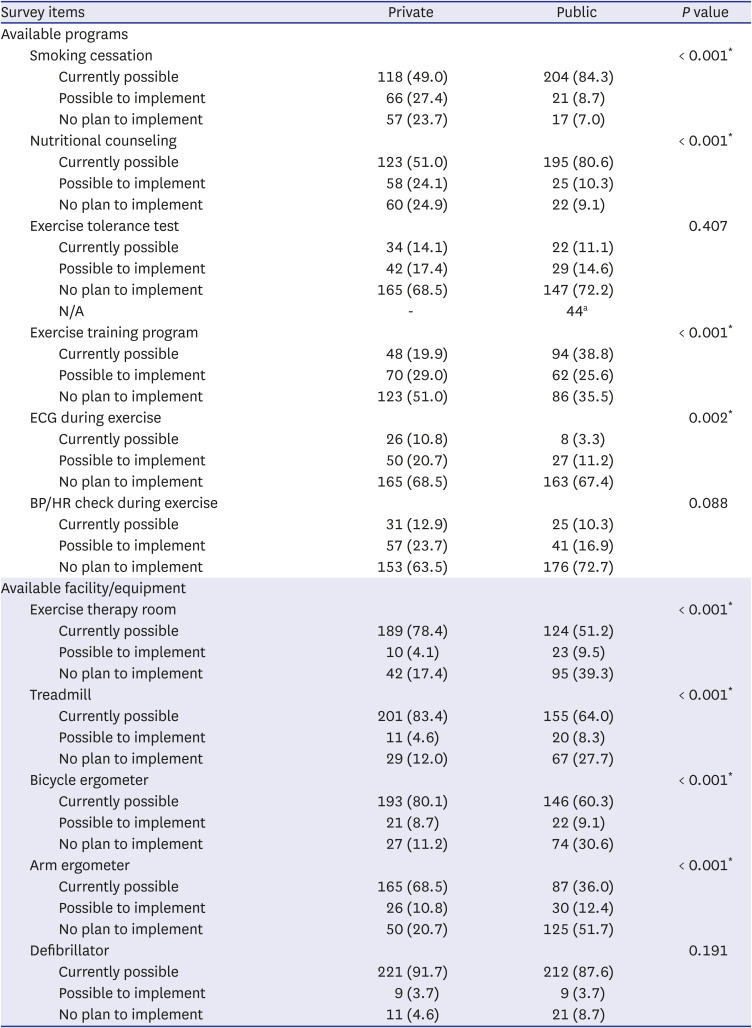
Table 2
Available resources for operating cardiac rehabilitation program of regional medical institutions
N/A = not applicable, ECG = electrocardiography, BP = blood pressure, HR = heart rate.
aThese answers were excluded from calculation of percentage.
*P < 0.05.
![]()
When monitoring equipment during exercise training was investigated thoroughly, ECG (wireless or wired) monitoring during exercise was more common in private institutions, with discrepancies between the two institutions. Of the private and public institutions, 28% and 37.9%, respectively, answered that they did not have monitoring equipment during exercise. Both institutions had more than half of the physiotherapists, but there were more athlete therapists and exercise specialists in public institutions (Table 3). This is because it is difficult to claim medical fees for athlete therapists or exercise specialists in medical institutions in Korea’s current medical system.
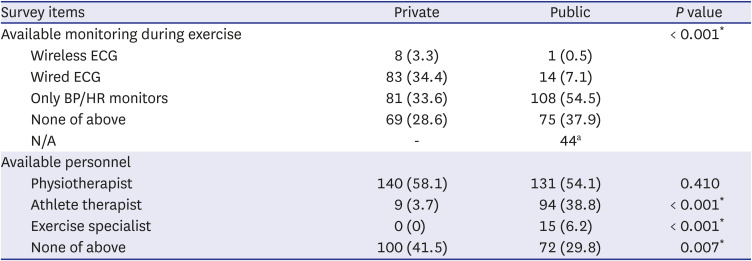
Table 3
Available monitoring and personnel for operating cardiac rehabilitation program of regional medical institutions
ECG = electrocardiography, BP = blood pressure, HR = heart rate, N/A = not applicable.
aThese answers were excluded from calculation of percentage.
*P < 0.05.
![]()
In private institutions, there was a higher rate of respondents who answered that they could perform CR at their own institutions with specific conditions, such as 1) PCI hospital requests with exercise prescriptions or referrals; 2) constant contact with PCI hospital is guaranteed; 3) the risk of cardiac attack is low during exercise; and 4) patients wish to receive CR at a regional medical institution. The number of respondents who replied that their institutions did not need to be responsible for providing CR was as low as 10% in both institutions.
The majority of institutions reported that the difficulty in managing CR would be due to the lack of facilities, equipment, and budget, as well as concerns regarding the risk of aggravating the patient's condition during exercise therapy. Compared to private institutions, the proportion of those who answered that they were unfamiliar with CR was higher in public institutions.
When asked about areas that needed support for CR operation, more than 70% of both institutions cited support for facilities, equipment, and human resources; educational programs for training CR professionals; and connection with PCI hospitals. The percentage of respondents who answered that financial support for operating a CR was needed was lower in public institutions. There was only one private institution and three public institutions which answered that CR was impossible or unnecessary (Table 4).
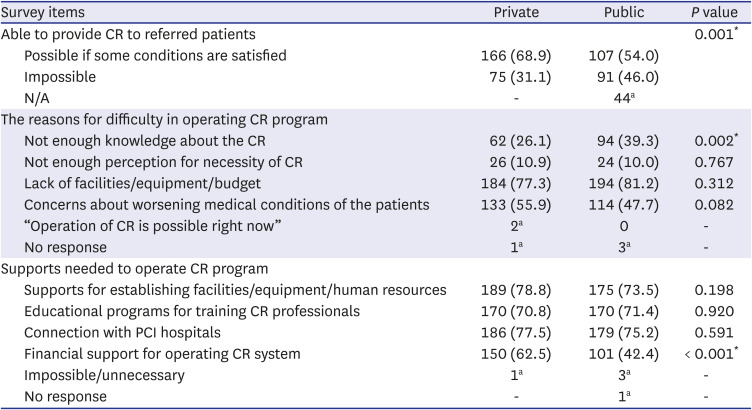
Table 4
Perception for cardiac rehabilitation of regional medical institutions
CR = cardiac rehabilitation, N/A = not applicable, PCI = percutaneous coronary intervention.
aThese answers were excluded from calculation of percentage.
*P <0.05.
![]()
A total of 16 answers (12 from private institutions and 4 from public institutions) satisfied the basic conditions for operating the CR program, including the exercise tolerance test, exercise training, ECG monitoring during exercise, and available personnel for CR operation. Among these, only two responded that CR was possible immediately, and all of them were private institutions. The remaining 14 institutions responded that CR was not operational because of the 1) ignorance of the concept and method of CR (four answers); 2) insufficient facilities, equipment, and employees (six answers); 3) concern about worsening patients’ condition during exercise training (six answers); 4) difficulty securing enough patients for operation of CR (two answers); and 5) financial burden of operating CR (one answer).
Current status of public health management institutions
Less than half of the current institutions are available for risk factor management programs and had exercise therapy rooms. Contrarily, more than half were equipped with treadmills and bicycle ergometers (68.9% and 77.0%, respectively), and more than 90% had defibrillators. However, only 19.7% answered that BP and HR checks during exercise were available at their institutions. The institutions where nurses or physiotherapists were working accounted for 27.5% and 34.8% of the total responses, respectively. Furthermore, of all responses received, 23.8% had exercise specialists, while 43.0% had no such personnel available (Table 5).
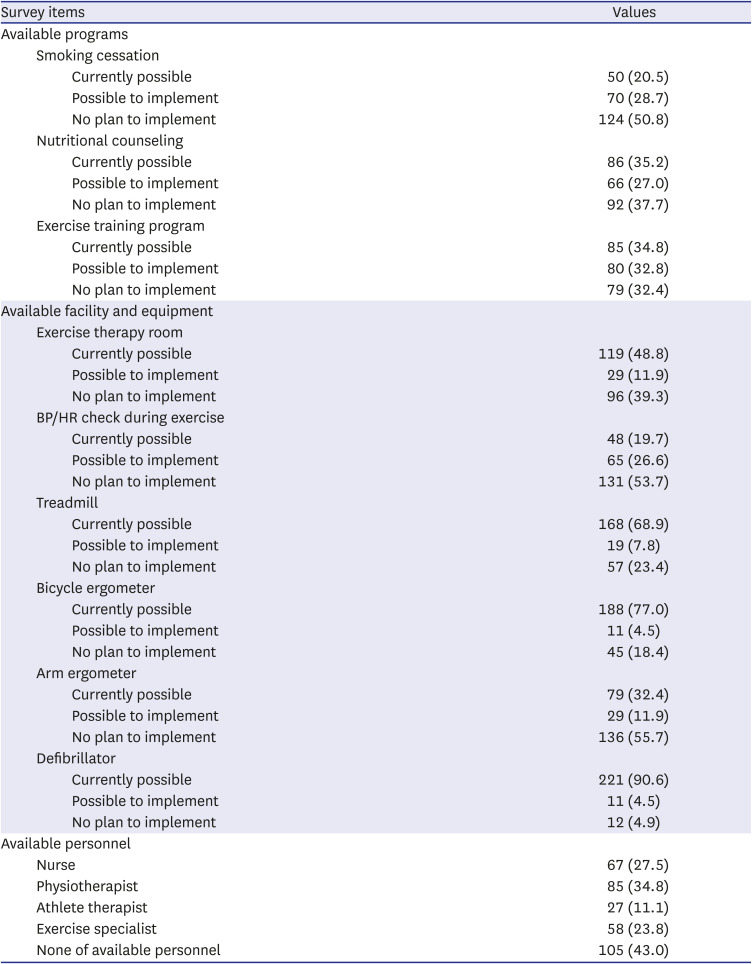
Table 5
Available resources for operating cardiac rehabilitation program of public health management institutions
![]()
Only one answer indicated that CR could be immediately operational, and three answered that CR is not the role of public health management institutions. As for the reasons for not being able to perform CR, answers describing the lack of facilities, equipment, and budget were much more common (73.4%). Fewer people responded that CR operation was not needed (16.0%), they did not know the concept and method of CR (37.7%), or they were concerned about the deterioration of the patient’s condition during exercise (33.6%). Public health management institutions generally answered that they need support in most operational areas to run CR in their institutions, as regional medical institutions did. However, answers that financial support for operating CR is needed was relatively low at 46.7%, whereas the other answers, such as support for establishing CR systems, educational program for training professionals, and connection with PCI hospitals, accounted for more than half (Table 6).
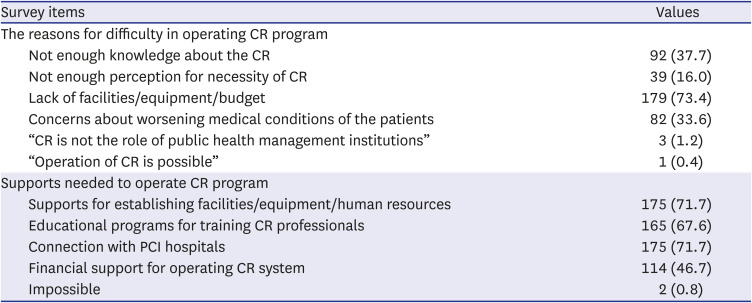
Table 6
Perception for cardiac rehabilitation of public health management institutions
Values are presented as number (%).
CR = cardiac rehabilitation, PCI = percutaneous coronary intervention.
![]()
Go to :
DISCUSSION
CR is an essential secondary prevention program for patients with CVD, and the most important element of CR is aerobic exercise training. The effects of CR are dose-dependent; hence, the patients who received 36 treatment sessions had significantly better outcomes than those who received fewer treatments.15 And life-long maintenance management is necessary even after the completion of exercise training sessions to sustain the clinical effects of CR.16 Therefore, sustainability and patients’ convenience to participate in CR are as important as developing expert exercise programs.
In the late 1990s, a well-organized CR program was introduced in several university hospitals in Seoul, Korea. Since 2008, the Ministry of Health and Welfare has designated 14 Regional Cardiocerebrovascular Centers nationwide and made the CR program mandatory to reduce regional variations and promote the distribution of CR.17 Since February 2017, CR has been reimbursed by the National Health Insurance Service. In 2019, a highly qualified clinical practice guideline for CR tailored to the situation in Korea was published.181920 However, despite these efforts, there are only 39 medical institutions that provide CR in Korea according to a recent report,21 which is less than that in other countries which have similar economic levels.22 Moreover, the rate of CR participation is also very low in Korea compared to that in other countries. According to a recent study, only 1.5% of patients with acute myocardial infarction participated in the CR program,10 which is much lower than other advanced countries with 30–40% of CR participation.923
Kim et al.10 suggested that at least 260 institutions would be required to operate CR programs in Korea, considering the incidence of acute myocardial infarction and the number of CR treatments that could be handled per institution. Apart from acute myocardial infarction, many CVDs require the implementation of CR; hence, more CR institutions than the estimate would be needed. Currently, approximately 160 PCI hospitals are identified in Korea. Even if CR programs will be installed in all PCI hospitals, approximately 100 additional institutions would be needed nationwide. Therefore, regional medical and health management institutions should be utilized in CR.
Accessibility is important for maintaining adherence to CR. One of the strategies to improve the low participation rate in CR is to activate community-based CR. In Korea, the population is aging at an unprecedented rate in the world. The proportion of elderly households is also gradually increasing.24 Elderly patients are likely to have problems with transportation to hospitals. For younger, economically active patients, a CR program that is flexible with time is needed.25 Therefore, utilizing the health-related resources of the community can facilitate CVD patients’ participation in CR in nearby institutions at a convenient time.26 For patients with high risk of heart attack during exercise, such as those with advanced heart failure, complex dysrhythmia, and complicated myocardial infarction, exercise training in specialized hospitals with a professional response system should be considered. However, for patients classified as having low to moderate risk of a cardiac attack during exercise as determined by a cardiopulmonary exercise test, CR can be safely provided in regional hospitals or clinics that do not perform PCI. In addition to regional medical institutions, health management institutions and gyms are good resources to fill the gaps in unmet community-based CR.27
However, as we can see from this study, it is still difficult to utilize regional health-related resources for CR in Korea. Although many institutions have equipment and facilities for exercise training, monitoring equipment for the patients’ medical conditions during exercise is lacking. Most institutions were aware of the need for CR but were burdened with the cost of building manpower and facilities to install and operate CR programs at their own institutions. Although the National Health Insurance Service reimburses CR, it is still believed that regional medical institutions have a high entry barrier. The management and control of CVDs are very important in national health policy. Considering the medical and social burden caused by CVDs, it is not desirable to take responsibility for the establishment of CR only for regional health-related institutions. Since CR has already been proven to be cost-effective,28 a systematic CR network should be established in order to effectively manage CVDs.29
Because this survey was conducted in the early stages of the coronavirus disease 2019 pandemic and each institution was focusing on quarantine work at the time, this voluntary survey research resulted in a somewhat lower response rate than expected. Of all the institutions included in this study, 44.9% responded, and more than half (352 out of 665 institutions) of the medical institutions replied. However, we believe that this response rate is not insufficient to reflect and represent the actual condition of regional CR resources. Even if the response rate increased, we surmise that the additional results would not have a significant impact. We also regard that forcibly drawing more answers from the institutions that did not voluntarily respond can result in a response bias in this research.
There are several additional limitations in this study. Since private medical institutions were selected through an internet search of data disclosed to the Health Insurance Review and Assessment Service, it was difficult to grasp the actual situation of each institution. It is possible that the questionnaires were sent to inappropriate institutions. We initially planned to conduct a field survey if the response was inadequate; however, field surveys were not possible during the pandemic because visitors’ access to hospitals was restricted due to the strict implementation of social distancing, especially when in medical institutions. Public medical institutions may have been overloaded with quarantine work, and health management institutions may have stopped operating. Therefore, it was not possible to verify whether the answers surveyed by each institution reflected reality. Although each region in Korea was supposed to be analyzed, there was a large deviation in the number of institutions and response rates in each region, and there were no clear patterns among regions. Moreover, though private health care institutions such as private gymnasiums have been excluded from the survey, it is expected that preparations for CR at these institutions are much poorer than those at public health management institutions.
In conclusion, currently there are few available resources for community-based CR at both regional medical institutions and public health management institutions in Korea. Therefore, long-term and specific policies for utilizing community institutions encompassing insurance fees and supporting human resources, equipment and budget, and linkages among the institutions are required for a well-functioning CR network.
Go to :
 XML Download
XML Download