

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
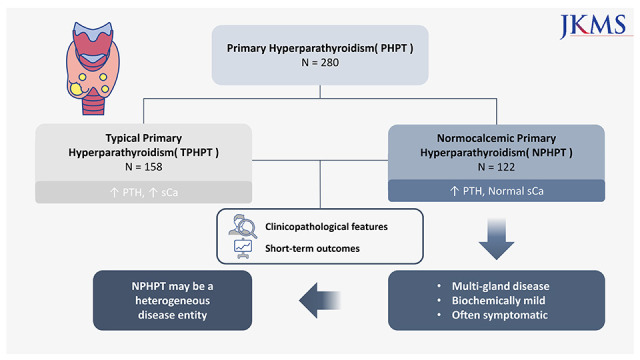
The concept of normocalcemic primary hyperparathyroidism (NPHPT) was first described in 2008, at the Third International Workshop on the Management of Asymptomatic Primary Hyperparathyroidism.1 It is defined as consistently elevated serum parathyroid hormone (PTH) levels with normal albumin corrected serum calcium (sCa) and ionized calcium (iCa), after excluding all secondary causes of PTH elevation.2 However, it is challenging to diagnose NPHPT because of the controversies over the optimal timing or frequency, and the reference range of blood tests.
Various attempts have been made to distinguish between NPHPT, typical primary hyperparathyroidism (TPHPT), and related disorders that can cause secondary hyperparathyroidism. Madeo et al.3 have suggested that the calcium/phosphorus (Ca/P) ratio is a cost-effective tool to identify PHPT with no requirements to measure PTH level. However, its sensitivity was as low as 67% for the NPHPT group compared to 89% for the TPHPT group. Since the negative predictive value was high (88%) in the study, the Ca/P ratio may be more useful to rule out NPHPT. Guo et al.4 proposed a parathyroid function index to be a reliable tool for distinguishing true NPHPT from vitamin D-deficient secondary hyperparathyroidism. Lavryk et al.5 presented the nomogram using Ca and PTH to distinguish healthy individuals from diseased patients, particularly those presenting atypical forms of PHPT. However, these studies are limited as they lack serum iCa measurements. Also, single measurements of sCa and PTH in the studies may overestimate the prevalence of NPHPT.
Owing to this lack of consistency in the diagnosis and the diverse methodology, the prevalence and complication rate of NPHPT vary widely among studies. The reported prevalence of NPHPT varies from 0.1% to 6%.67 In population-based studies, the risk of bone or renal complications did not increase as compared to the normal population.678910 However, reports of small cohorts in referral centers revealed cases of NPHPT with substantial rate of osteoporosis, low-trauma fractures, and renal stones.111213
The pathophysiology and etiology of NPHPT are still not conclusive. Among the multiple hypotheses, the most widely accepted concept is that NPHPT is an early form of TPHPT.1415 In addition, aging process, menopause, oral calcium loading, low free 25-hydroxyvitamin D level, a partial resistance to PTH, and altered parathyroid sensing are suspected to be possible drivers of pathogenesis.16171819202122 However, none of these have been proven to support all cases. Moreover, it is still not clear whether NPHPT progresses toward TPHPT over time. The optimal management strategy for NPHPT is also debatable.
In this study, we retrospectively investigated the clinicopathological features and short-term outcomes of surgically treated NPHPT patients and compared it to those of TPHPT patients. All patients were tested for iCa. Based on this, the true normocalcemic group with normal iCa and sCa and elevated iCa and normal sCa groups were further compared.
Go to : 
METHODS
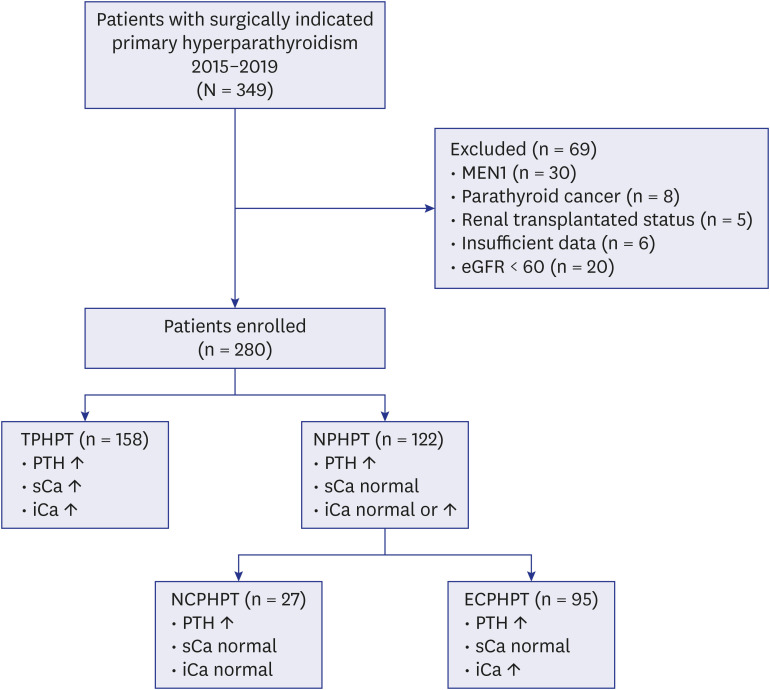
We screened a total of 349 patients with the diagnosis of PHPT who were indicated for a parathyroidectomy between 2015 and 2019 at Yonsei Severance hospital, Seoul, Korea. We finally enrolled 280 patients after excluding patients with multiple endocrine neoplasms, parathyroid malignancy, history of renal transplantation, missing data, and renal disease (estimated glomerular filtration rate [eGFR] < 60 mL/min/1.73 m2) (Fig. 1). The patients were divided into two groups according to the preoperative PTH level and corrected sCa and iCa: the TPHPT group (elevated PTH, sCa, and iCa: n = 158) and NPHPT group (elevated PTH, normal sCa, and normal or elevated iCa: n = 122). For subgroup analysis, the NPHPT group was further divided into two subgroups: the normo-ionized calcemic primary hyperparathyroidism (NCPHPT, elevated PTH, normal sCa, and normal iCa: n = 27) subgroup and elevated-ionized calcemic primary hyperparathyroidism (ECPHPT, n = 95) subgroup.
Clinicopathological factors such as age, sex, symptoms, and signs (including nephrolithiasis and bone fracture), laboratory results, preoperative imaging findings, and pathology of excised parathyroid glands were reviewed from patient medical records and pathology reports. Normal laboratory ranges at our institution are as follows: sCa, 8.5–10.5 mg/dL; iCa, 4.5–5.2 mg/dL; PTH, 15–65 pg/mL.
Surgical indications for PHPT in our cohort included age < 50 years, sCa > 1 mg/dL above the normal upper limit, nephrolithiasis, reduced eGFR of < 60 mL/min, osteoporosis, and a history of nontraumatic bone fractures.23
All the preoperative laboratory findings were checked more than twice, at least 3–6 months prior to the surgery and within a week before surgery. The most recent value was used for analysis. Most of the patients underwent preoperative imaging studies to examine localization, with cervical ultrasonography (US), 99mTc-methoxyisobutylisonitrile single photon emission computed tomography/computed tomography (99mTc-MIBI SPECT/CT) or SPECT, or both. In case of failed localization using US and SPECT, a four-dimensional CT scan was considered. Parathyroid venous sampling was performed when there were discordant or ambiguous results between the modalities.
All patients received focused parathyroidectomy unless the preoperative imaging study failed to localize the affected lesion. In case of failed localization, bilateral neck exploration was performed. All patients underwent intraoperative PTH monitoring (IOPTH) during the surgery. According to the Miami criterion, a more than 50% decrease in intraoperative PTH from the baseline value (preoperative PTH measured on the day before surgery) at 10 minutes after initiation of parathyroidectomy was considered as an indication for terminating the surgery. In cases where patients who underwent focused parathyroidectomy did not meet the Miami criterion, unilateral neck exploration with repeated IOPTH monitoring at 20 minutes after parathyroidectomy was performed when preoperative localization was definite. In cases where the Miami criterion was not met at the secondary IOPTH or vague results of preoperative localization were obtained in initially focused parathyroidectomy patients, further bilateral neck exploration was performed. There was no patient who did not meet the Miami criterion and underwent initial bilateral neck exploration and secondary bilateral neck exploration.
Statistical analyses was performed using SPSS v26.0 (IBM Corp., Armonk, NY, USA). χ2 and Fisher’s exact tests were used for categorical variables. Student’s t-test and Mann–Whitney U tests were applied for continuous variables. Statistical significance was set at P < 0.05.
Ethics statement
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Yonsei University College of Medicine (IRB No.4-2020-0043). The research was performed in accordance with the Declaration of Helsinki. The requirement for informed consent was waived owing to the retrospective nature of the study.
Go to :
RESULTS
Patient characteristics are presented in Table 1. The occurrence of NPHPT was common among younger individuals (age < 50 years, P = 0.025). Although the bone density measured by dual energy X-ray absorptiometry was higher in the NPHPT group (P = 0.008), the rate of nontraumatic bone fracture did not differ between the two groups. Nephrolithiasis was not uncommon in the NPHPT compared to TPHPT. Preoperative PTH, sCa, and iCa levels were significantly higher in the TPHPT group (P < 0.001, P < 0.001, and P < 0.001, respectively).
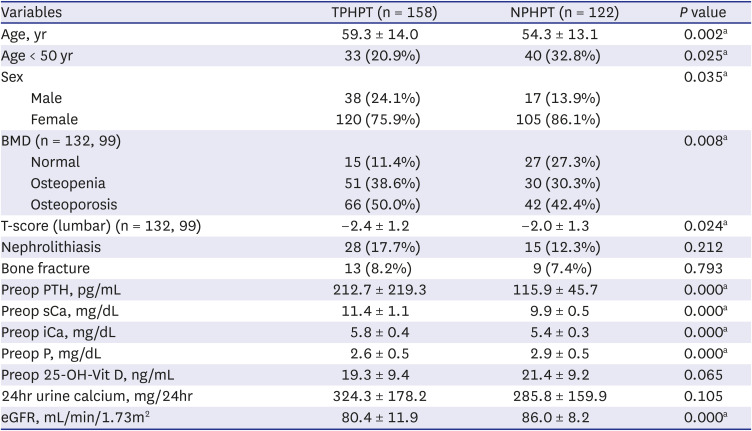
Table 1
Clinical characteristics of patients
All continuous variables expressed as mean ± standard deviation.
TPHPT = typical primary hyperparathyroidism, NPHPT = normocalcemic primary hyperparathyroidism, BMD = bone mineral density, PTH = parathyroid hormone, sCa = serum calcium, iCa = ionized calcium, P = phosphorus, 25-OH-Vit D = 25-hydroxy-vitamin D, eGFR = estimated glomerular filtration rate.
aStatistical significance.
![]()
The results of IOPTH and pathological findings are presented in Table 2. Although the drop rate of PTH (%) was lower in the NPHPT group, there was no significant difference observed between the two groups. Patients with NPHPT tended to higher number of multiple lesions than TPHPT patients (P = 0.004), and in regard to multi-gland disease, the size of the glands was smaller in NPHPT patients than that in TPHPT patients (P = 0.011). Among the patients who did not meet the Miami criterion in the TPHPT (15 patients) and NPHPT group (15 patients), four and two patients had multi-gland disease, respectively. All the 24 single-gland diseased patients showed further decline in IOPTH after 20 minutes. Remaining six multi-gland patients were converted into bilateral neck exploration and all patients were cured as of the last follow-up.
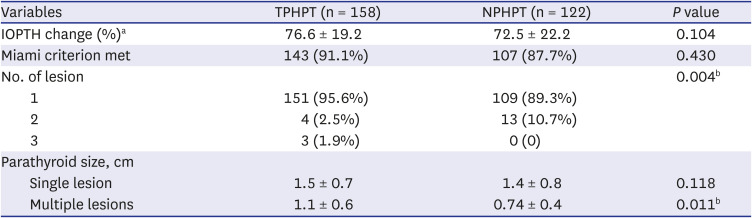
Table 2
Intraoperative parathyroid hormone monitoring and pathology
All continuous variables expressed as mean ± standard deviation.
TPHPT = typical primary hyperparathyroidism, NPHPT = normocalcemic primary hyperparathyroidism, IOPTH = intraoperative PTH monitoring.
Miami criterion; IOPTH drop ≥ 50% from the highest of either pre-incision or pre-excision level at 10 minutes after gland excision.
a% change from baseline; bStatistical significance.
![]()
The laboratory findings of the follow-up periods are summarized in Table 3. All patients underwent at least 12 months of follow-up. Postoperative PTH, sCa, iCa, and phosphorus showed no difference until 3 months in both the groups. Although the sCa level was higher in the TPHPT group at 12 months after surgery, all the laboratory findings, including PTH, sCa, iCa and phosphorus, were within the normal range in both the groups. Twelve months after surgery, the value of vitamin D was 32.6 ± 11.7 in the TPHPT group and 31.1 ± 9.1 in the NPHPT group (P = 0.309).

Table 3
Postoperative laboratory change
All continuous variables expressed as mean ± standard deviation.
TPHPT = typical primary hyperparathyroidism, NPHPT = normocalcemic primary hyperparathyroidism, PTH = parathyroid hormone.
aStatistical significance.
![]()
The results of subgroup analysis of the NPHPT group are presented in Table 4. Preoperative PTH was higher in the ECPHPT group (P = 0.002). Otherwise, signs or symptoms of hyperparathyroidism, including osteoporosis, osteopenia, nephrolithiasis, and nontraumatic bone fracture were not different between the two subgroups. The rate of multi-gland disease was higher in the NCPHPT group; however, the difference was not statistically significant. In case of single-gland disease, the size of the gland was larger in the ECPHPT group (P = 0.003). In case of multi-gland disease, NCPHPT group showed larger sized of parathyroid glands (P = 0.012).
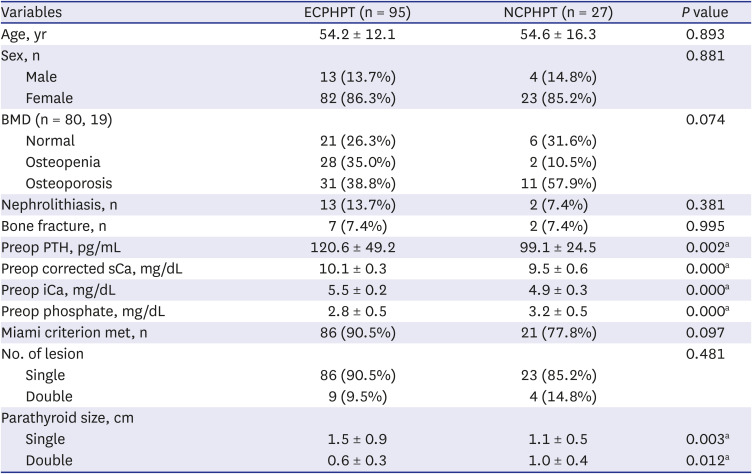
Table 4
Comparisons between ECPHPT and NCPHPT
All continuous variables expressed as mean ± standard deviation.
ECPHPT = normocalcemic primary hyperparathyroidism with elevated ionized calcium, NCPHPT = normocalcemic primary hyperparathyroidism with normal ionized calcium, BMD = bone mineral density, PTH = parathyroid hormone.
aStatistical significance.
![]()
The comparisons between TPHPT and NCPTHPT are summarized in Table 5. Although NCPHPT group showed milder laboratory profiles than that of TPHPT group, the incidences of bone related complications or nephrolithiasis were not uncommon compared to TPHPT group.
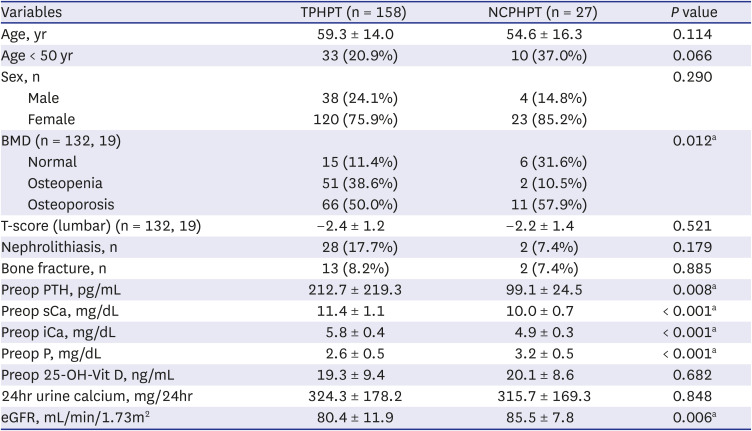
Table 5
Comparisons between TPHPT and NCPHPT
All continuous variables expressed as mean ± standard deviation.
TPHPT = typical primary hyperparathyroidism, NCPHPT = normocalcemic primary hyperparathyroidism with normal ionized calcium, BMD = bone mineral density, PTH = parathyroid hormone, sCa = serum calcium, iCa = ionized calcium, P = phosphorus, 25-OH-Vit D = 25-hydroxy-vitamin D, eGFR = estimated glomerular filtration rate.
aStatistical significance.
![]()
Go to :
DISCUSSION
According to our retrospective study of 280 patients who underwent parathyroidectomy for PHPT, 43.6% patients were preoperatively normocalcemic. When iCa levels were further analyzed, “true” NCPHPT patients were reduced to 9.6%. Previous studies have also demonstrated the importance of iCa in the diagnosis of NCPHPT. It reflects biologically activated calcium levels most accurately,2425 and directly acts on the calcium-sensing receptors to regulate PTH secretion.26 Many ‘normocalcemic’ patients are known to have elevated iCa levels.27 In many previous studies, iCa was not adopted for preoperative evaluation. Since sCa in PHPT patients often fluctuates, single measurement of sCa with upper-normal range can result in the misdiagnosis of NPHPT.28
In our cohort, blood tests, including iCa, were performed more than twice for every patient for an accurate diagnosis. Also, ‘true’ NCPHPT patients were selected separately based on the iCa levels. The biochemical profiles of NPHPT patients were milder than that of TPHPT patients, which was consistent with other studies.1520 The NCPHPT group showed further decrease in PTH, sCa, and iCa levels.
Contrary to the mild biochemical profile, the presentations of the NPHPT group were not indolent in our cohort. The occurrence of symptoms including bone-related complications (low traumatic fracture) and renal stones in NPHPT patients were similar to those of the TPHPT group. There are few studies that reported the substantial rate of symptomatic patients.11121529 As most of these results are from referral centers for metabolic bone disease, the possibility of an implicit selection bias has been raised.28 Since our institution is also a referral center, more patients with symptoms could have been included. In a recent multi-center, cross-sectional study conducted in Italy, the authors reported no difference in nephrolithiasis between the two groups. In contrast, the bone phenotype of NPHPT resembled the control group rather than the PHPT group.30
The NPHPT group more commonly showed small, multiple parathyroid lesions, which reduced the sensitivity of all types of preoperative imaging modalities. Lim et al. reported that normocalcemic patients require bilateral neck operations over 8 times more frequently than patients with a typical or normo-hormonal PHPT.31 The sensitivity of imaging modalities can be improved in combination with other parameters.32
Although the pathophysiology of NPHPT has not been clearly elucidated, our data suggests that NPHPT may be a different disease entity from TPHPT, and not the earliest form of typical, mild asymptomatic PHPT, considering its young age of onset and multiplicity. One of the hypotheses that explains the maintenance of normal sCa concentration in NCPHPT is the resistance of bones and kidney to PTH.20 This hypothesis is further supported by a recently published study on the genetic data of NPHPT.22 The authors of the study found that A986S polymorphism of calcium-sensing receptor, which is linked to PTH resistance, is an independent predictor of PTH level in NPHPT patients, but not in asymptomatic hyperparathyroidism. There are some studies that reported no conversion to hypercalcemia as the natural history of NPHPT, which support our hypothesis.711 On the other hand, there have been reports stating that a small percentage of patients proceed to frank hypercalcemia.1013 Further studies are required to evaluate the genetic and clinical differences between NCPHPT and asymptomatic or mild hyperparathyroidism.
It is notable in our study that subgroup analysis of ECPHPT (normocalcemic but elevated iCa) and NCPHPT (‘true’ normocalcemic with normal iCa) group showed no differences in symptoms and pathology. Current guidelines recommend checking iCa for precise diagnosis of NPHPT.2 However, our data suggest that measuring sCa might be enough to distinguish ‘normocalcemic’ group from TPHPT, which presents distinctive features of multi-gland disease with mild biochemical profile. This result is not conclusive, because of the small number of NCPHPT group.
This study has several limitations. First, it is a retrospective study with a small sample size. The prevalence of PHPT in Korea is known to be 0.007–0.0013%.33 The total number of true normocalcemic hyperparathyroidism was as small as 27, even though our center is large, tertiary referral center.
Second, the mean value of 25-OH-vitamin D (ng/mL) was < 20 ng/mL in our study. The threshold of vitamin D varies among guidelines, being ≥ 20 ng/mL or even ≥ 30 ng/mL.3435 A rigorous definition of NPHPT requires at least 30 ng/mL of 25-OH-vitamin D levels to exclude TPHPT or secondary hyperparathyroidism.28 There is an inverse relationship between PTH and 25-OH-vitamin D. Increasing vitamin D levels increase Ca levels by improving intestinal Ca absorption, which might change the expected diagnosis of NPHPT to TPHPT. This can explain the high prevalence of NPHPT in our study cohort. According to nationwide data from the Korea National Health and Nutrition Examination Survey, 71.4% of Korean adults have vitamin D deficiency (< 20 ng/mL), associated with environmental and occupational factors.36 If the criteria for vitamin D deficiency is set more strictly as < 30 ng/mL, the proportion of vitamin D deficiency in our population will further increase. While strict application of these criteria for vitamin D is challenging owing to geographical characteristics, clinicians in similar environment in our country have to be aware that the prevalence of normocalcemic PHPT would be much higher than reported.
Third, our study included only surgically treated patients, thus the natural history of normocalcemic PHPT was not evaluated. Kontogeorgos et al.9 reported that NPHPT is a common condition as 11% at follow-up and only one of 608 subjects developed mild hypercalcemia in 13 years. In a recent large-cohort study conducted in the United Kingdom, seven of 11 NPHPT patients experienced intermittent hypercalcemia.37 The results of the natural history of NPHPT remain elusive. Heterogeneous methodologies implied while checking laboratory values might have been the reason for these conflicting results. Further prospective, large-scale studies are needed to establish the natural course of the disease.
Despite these limitations, our study adds to the small body of literature on normocalcemic PHPT. According to our study, NPHPT might be a heterogeneous disease entity of PHPT with a high rate of multi-gland disease, which appears to be biochemically milder, but often symptomatic. It is hard to detect the lesions via imaging modality in multi-gland disease. Intraoperative PTH monitoring might help increase the success rate of surgery. The short-term outcomes of NPHPT after surgery did not differ from that of TPHPT.
Go to :
 XML Download
XML Download