

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was identified at the end of 2019 as the cause of the outbreak of acute respiratory syndrome in Wuhan, Hubei Province, China.1 Thereafter, it spread rapidly around the world, causing a pandemic, and was named coronavirus disease 2019 (COVID-19).2 Vaccination against SARS-CoV-2 began in several countries from mid-December 2020, and by ≤ 11 months later, nearly half of the global population had received at least one dose of vaccine.3 However vaccine inequity is significant among nations, and only about 3.6% of the population in low-income countries have been vaccinated with even one dose.3 Globally, 2.9 million people per week contract COVID-19, and the number of new deaths is still > 49,000 per week.4 As of November 1, 2021, the global cumulative numbers of persons infected with COVID-19 and consequent deaths have exceeded 247 and 5 million, respectively.5 Various vaccines and treatments are being developed to overcome COVID-19, but more therapeutic strategies are needed. Furthermore, viruses mutate over time, which seems to affect viral transmission and disease severity, as well as vaccine and therapeutic efficacy.678910 Until recently, the only drugs recommended by the World Health Organization (WHO) for treating patients with COVID-19 are corticosteroids and interleukin-6 receptor blockers (tocilizumab or sarilumab) in severe or critical patients.11 In the revised guidelines on September 24, 2021, the casirivimab/imdevimab combination was recommended in mild or moderate patients at the high risk of severe disease, and severe patients with seronegative status. Among antivirals, remdesivir has been approved by the U.S. Food and Drug Administration (FDA) for hospitalized patients with COVID-19 who require supplemental oxygen.12
Monoclonal antibodies (mAbs) targeting specific regions of viral surface proteins should be promising treatments against infectious diseases,1314 and they are therapeutically effective against several viruses.1516 Among the anti-SARS-CoV-2 mAbs for the treating COVID-19, combination therapies of bamlanivimab/etesevimab and casirivimab/imdevimab, and sotrovimab monotherapy have received emergency use authorization (EUA) from the FDA for outpatients with mild-to-moderate COVID-19 at high risk and they are recommended by the National Institutes of Health (NIH).12
Regdanvimab (CT-P59) is a recombinant neutralizing mAb constructed from the blood of convalescing patients with COVID-19, and it potently neutralizes the receptor-binding site of the SARS-CoV-2 spike protein as an antigen target.17 Results from a phase 2/3 randomized, double-blind, placebo-controlled clinical trial of outpatients with mild-to-moderate SARS-CoV-2 infection found that regdanvimab shortened the time to conversion to a negative real-time quantitative reverse transcriptase polymerase chain reaction (RT-PCR) result and clinical recovery without causing serious side effects or death, and lowered rates of oxygen therapy.18 Regdanvimab received product approval based on these results on February 5, 2021, under the condition of submitting the results of the phase 3 clinical trial thereafter, and it became available to improve clinical symptoms in patients aged ≥ 18 years at high-risk mild or moderate COVID-19 in Korea.19 High-risk was defined as age ≥ 60 years, or having ≥ 1 underlying disease such as cardiovascular or chronic respiratory diseases including asthma, hypertension, or diabetes, and moderate refers to patients with pneumonia.20 On March 26, 2021, the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) concluded that regdanvimab could be used to treat adult patients with COVID-19 who do not require supplemental oxygen but are at high risk of progression to severity.21 Then, on September 17, 2021, the Ministry of Food and Drug Safety extended the scope of administration based on the results of the phase 3 clinical trial of regdanvimab and granted official product approval. Accordingly, the indications for regdanvimab were designated as high-risk mild and all moderate COVID-19 patients, and the high-risk included age > 50 years, body mass index (BMI) > 30 kg/m2, cardiovascular disease (including hypertension), chronic lung disease (including asthma), diabetes mellitus, chronic kidney disease (including dialysis), chronic liver disease, or immunosuppression due to disease or treatment.22
No drugs had been approved in Korea for treating mild-to-moderate COVID-19 until the conditional approval of regdanvimab.23 Therefore, regdanvimab is presently the only agent available in Korea that could prevent progression in patients at high-risk mild-to-moderate COVID-19. However, since the results of the phase 3 clinical trial have not yet been published and accumulated data are scant, the basis for judgment regarding treatment selection in routine clinical practice is insufficient.
Busan Medical Center (BMC) in Busan, the second largest city in Korea, is a currently operating, dedicated COVID-19 treatment facility. As of April 16, 2021, about 3,000 inpatients have been treated, and regdanvimab has been administered to > 400 patients since its approval. This study aimed to evaluate the effectiveness and safety of regdanvimab administered to patients at high-risk mild-to-moderate COVID-19 in real-world clinical practice. Given the lack of accumulated data about regdanvimab, we hope that the present results will serve as a meaningful basis for drug selection to treat patients with COVID-19.
METHODS
Patient population and data elements
This observational study retrospectively analyzed the medical records of adult patients (aged ≥ 18 years) with COVID-19 (confirmed by RT-PCR) who were admitted to BMC between December 1, 2020 and April 16, 2021. Each patient followed up until death or discharge. The study period ended on May 14, 2021, allowing for the last date of discharge in all patients. The patients with high-risk mild-to-moderate COVID-19 eligible for regdanvimab were extracted and assigned to groups that were treated or not with regdanvimab. Since regdanvimab was supplied and administered at BMC from February 19, 2021, all patients given regdanvimab were hospitalized after that date. The patients who were not treated with regdanvimab were admitted before February 19, 2021, and some who were hospitalized when regdanvimab became accessible refused to be treated with it.
Baseline characteristics including age, sex, BMI, comorbidities, and co-medications were analyzed. Comorbidities consisted of diabetes mellitus, hypertension, and cardiovascular, chronic lung, chronic kidney, and chronic liver diseases, as well as pneumonia, which is an indicator of moderate COVID-19. Co-medications included those that were presumed to affect COVID-19 treatment in previous studies, and those administered to treat comorbidities. These were classified as angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs),2425 statins,2627 aspirin,2829 and immunomodulators.3031 Immunomodulators include immunosuppressants and corticosteroids.
Several laboratory parameters at baseline that were also collected from electronic medical records (EMRs), included complete blood cell count, electrolytes, renal function, hepatic panel, C-reactive protein (CRP), lactate dehydrogenase (LDH), D-dimer, troponin I, ferritin, and creatine kinase.
Study exposure
The exposure in this study was regdanvimab. Regdanvimab administration was also identified in the EMRs. Regdanvimab was administered at the recommended dose of a single intravenous infusion of 40 mg/kg. Azithromycin, corticosteroids, hydroxychloroquine, lopinavir/ritonavir, and remdesivir, were evaluated as other treatment exposures of interest.
Study outcomes
The primary outcome was a composite of in-hospital death, or disease aggravation. Disease aggravation indicators included the need for oxygen therapy (low- or high-flow oxygen therapy, and mechanical ventilation) or transfer to a tertiary hospital for further invasive treatment. The secondary outcomes were length of hospital stay (days) and adverse reactions including fever or systemic pain, injection site reaction, hypersensitivity, and gastrointestinal, hematological, renal, and hepatic toxicity.
Statistical analysis
We assessed differences in demographic characteristics, baseline clinical characteristics, and co-medications between the groups. Summary statistics are presented as medians with interquartile ranges (IQRs) for continuous variables, and numbers and percentages for categorical variables. Between-group differences were examined using independent t-tests and χ2 tests, as appropriate. The low accuracy of χ2 tests was compensated for using Fisher exact tests.
Although the study was limited to patients suitable for regdanvimab administration, the baseline characteristics between the regdanvimab treated and untreated groups differed. Therefore, we balanced measured covariates by estimating propensity scores (PS) of regdanvimab administration using a multivariable logistic regression model, adjusted for the variables of age, sex, BMI, comorbidities, and disease severity. PSs were matched using the optimal method without designation of a caliper to prevent omission of the group treated with regdanvimab, and the results were confirmed. All baseline variables in the PS-matched cohort were descriptively analyzed. Detailed information on the modeling of PS matching was described in Appendix 1.
Differences in outcomes between groups with and without (reference) regdanvimab therapy in the PS-matched cohort and whether the estimated effect of regdanvimab remained consistent in the overall cohort were determined by multivariable logistic regression analyses. Variables in the multivariable analyses that affect the prognosis of COVID-19 were included as risk factors in the regdanvimab dosing criteria.21 Co-medications were included, and sex was added based on recent findings.323334 To confirm the consistency of the results, we performed sensitivity analyses by changing the covariates included in the PS estimation model, changing the matching method, and adding covariates in the multivariable logistic regression model of analyzing matching data.
Missing data
Among the 970 patients included in the study, 73 (7.5%) had no BMI information and were excluded from analyses. Some of the 897 patients included in the analysis had missing baseline laboratory values, and Table 1 shows laboratory results after excluding them.
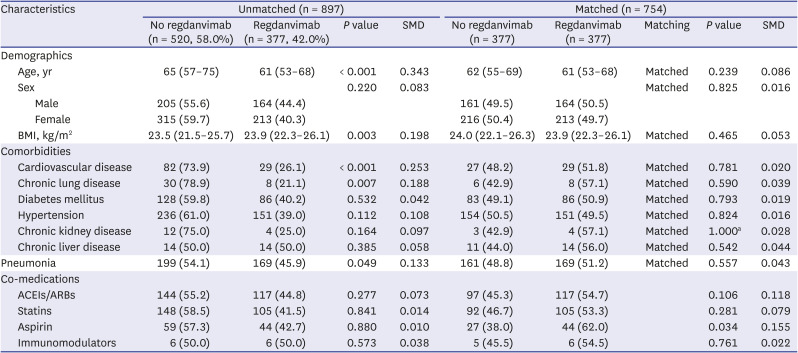
Table 1
Baseline characteristics in unmatched and propensity score matched cohorts of patients
Data are presented as number (%) or medians (interquartile range). Continuous variables were analyzed using Student t-tests. Categorical variables were analyzed using χ2 tests. Chronic kidney disease in matched cohorts was analyzed using Fisher exact test.
SMD = standardized mean difference, BMI = body mass index, ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin-receptor blocker.
aFisher exact test.
![]()
All data were statistically using R version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria), and values with P < 0.05 were considered significant.
Ethics statement
The Institutional Review Board (IRB) of Pusan National University approved this study (PNU IRB/2021_66_HR) and waived the requirement for informed consent. The data used in this study were anonymized after extracting patient data from the institution’s EMRs and did not contain any personally identifiable information.
RESULTS
Baseline patient characteristics
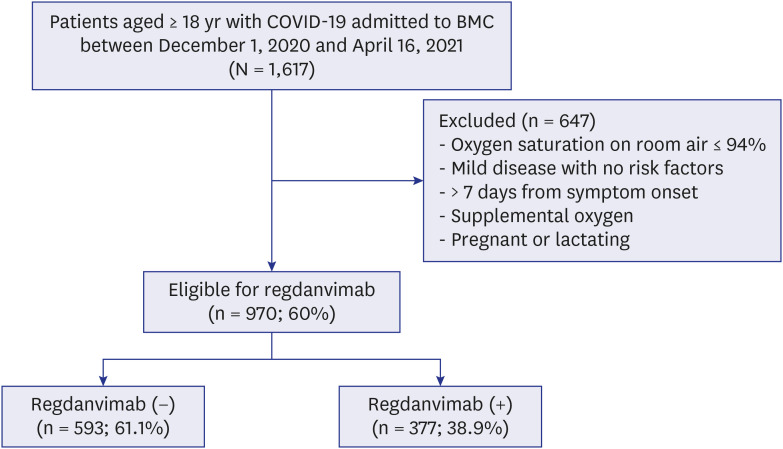
Among 1,617 patients with COVID-19 who were admitted during the study period, 970 (60.0%) were eligible for regdanvimab administration. These were assigned to receive treatment with (n = 377; 38.9%) or without (n = 593; 61.1%) regdanvimab (Fig. 1). Some immobile patients (n = 73) in the untreated group with missing height and weight records were excluded from analysis. Table 1 shows the baseline characteristics of the 897 patients. Patients in group without regdanvimab were older (median age 65 [IQR, 57–75] vs. 61 [53–68] years, P < 0.001), but sex did not significantly differ (P = 0.220). They had a lower BMI (23.5 [21.5–25.7] vs. 23.9 [22.3–26.1] kg/m2, P = 0.003), and a higher proportion of comorbid cardiovascular (73.9% vs. 26.1%, P < 0.001) and chronic lung (78.9% vs. 21.1%, P = 0.007) diseases. The proportion of patients with moderate COVID-19 (with pneumonia), was also higher in the untreated group (54.1% vs. 45.9%, P = 0.049). Other comorbidities (diabetes mellitus, hypertension, chronic kidney disease, and chronic liver disease) and co-medications (ACEIs/ARBs, statins, aspirin, and immunomodulators) did not significantly differ between the two groups.
Propensity-matched cohort characteristics
We created a PS-matched cohort of 754 patients, among whom, 377 were treated with regdanvimab and 377 were not. Demographics and comorbidities did not significantly differ between the PS-matched groups (Table 1). Among the co-medications that were not included in the matching variables, aspirin was prescribed to more patients in the regdanvimab group (Table 1). Supplementary Fig. 1 shows the distributions of covariates before and after PS matching. Differences in baseline characteristics were attenuated in the matched, compared with the unmatched cohort (Supplementary Fig. 2).
Patients in the PS-matched cohort who were treated with regdanvimab had significantly lower CRP (0.4 [0.4–1.8] vs. 0.7 [0.4–2.7] mg/dL, P < 0.001), LDH (206.0 [180.8–240.0] vs. 216.0 [190.5–257.0] IU/L, P = 0.011), and ferritin (169.0 [100.5–307.0] vs. 221.5 [124.3–378.3] ng/mL, P = 0.048] values, whereas D-dimer, troponin I, and creatine kinase values did not significantly differ (Table 2). Supplementary Table 1 shows details of the missing baseline laboratory data.
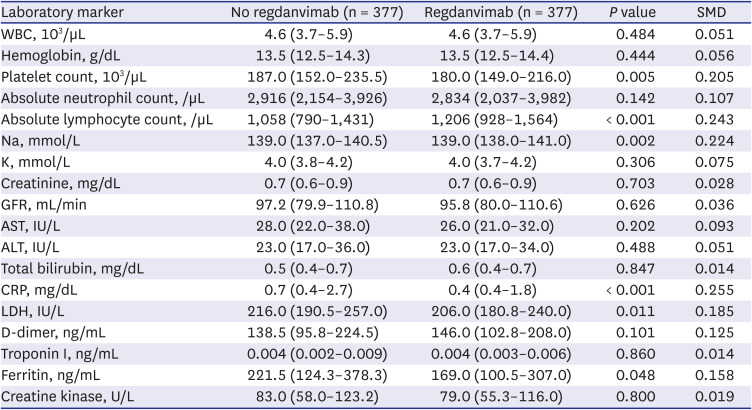
Table 2
Baseline laboratory data in propensity score-matched cohort
Data are presented as medians (interquartile range). Variables were analyzed using Student t-tests.
SMD = standardized mean difference, WBC = white blood cell, GFR = glomerular filtration rate, AST = aspartate transaminase, ALT = alanine transaminase, CRP = C-reactive protein, LDH = lactate dehydrogenase.
![]()
Regarding the use of other unapproved treatments for COVID-19, azithromycin, corticosteroids, lopinavir/ritonavir, and remdesivir were used significantly more in the regdanvimab-untreated group than in the regdanvimab-treated group throughout the entire hospital stay, and similar results were obtained except that remdesivir was not used in both groups, even if limited to administration before progressing to severe disease (Table 3).
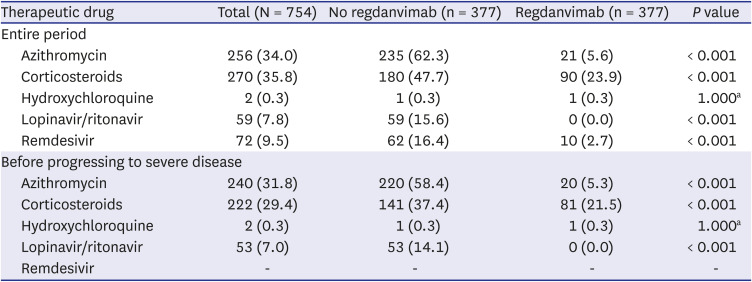
Table 3
Use of other therapeutics in propensity score-matched cohort
![]()
Clinical outcomes of PS-matched cohort
Table 4 shows the clinical outcomes in the PS-matched cohort. The composite outcome of death, or disease aggravation was reached by 19 (5%) and 81 (21.5%) patients treated with and without regdanvimab, respectively (absolute risk difference, −16.4%; 95% confidence interval [CI], −21.1, −11.7; relative risk difference [RRR], 76.5%; P < 0.001). Regdanvimab was also associated with a significant reduction in the composite outcome of death, or disease aggravation in univariate (odds ratio [OR], 0.194; 95% CI, 0.112, 0.320; P < 0.001) and multivariable-adjusted analyses (OR, 0.169; 95% CI, 0.095, 0.289; P < 0.001) (Supplementary Table 2). The secondary outcome, length of hospital stay, was shorter in the group treated with, than without regdanvimab (mean, 11.9 ± 3.3 vs. 13.7 ± 5.4 days; P < 0.001). The hematological adverse reactions of white blood cell abnormalities, thrombocytopenia, and lymphocytopenia were more frequent in the group that were not treated with regdanvimab, but other investigated adverse reactions did not significantly differ between the groups (Table 4).
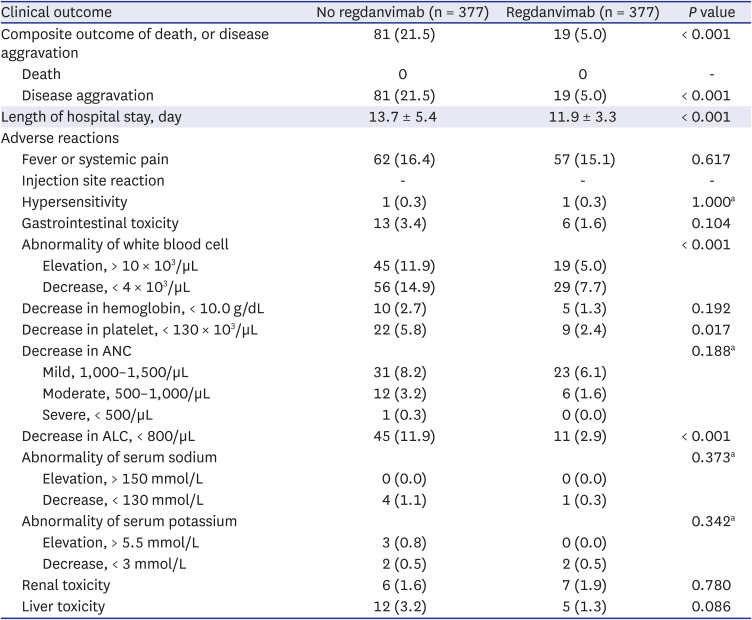
Table 4
Clinical outcomes in propensity score-matched cohort
Data are presented as number (%) or mean ± SD. Continuous and categorical variables were analyzed using Student’s t-tests and χ2 tests, respectively.
ANC = absolute neutrophil count, ALC = absolute lymphocyte count.
aFisher exact test.
![]()
Multivariable adjustment in the overall cohort
Regdanvimab was significantly associated with a reduction in the composite outcome of death, or disease aggravation in the overall cohort in the multivariable-adjusted analysis (OR, 0.148; 95% CI, 0.084, 0.247; P < 0.001) (Supplementary Table 2). Supplementary Table 2 shows the association between regdanvimab and the composite outcome of death, or disease aggravation among the analytical methods in the PS-matched and overall cohorts. These results were consistent with sensitivity analyses performed by various methods (Fig. 2).
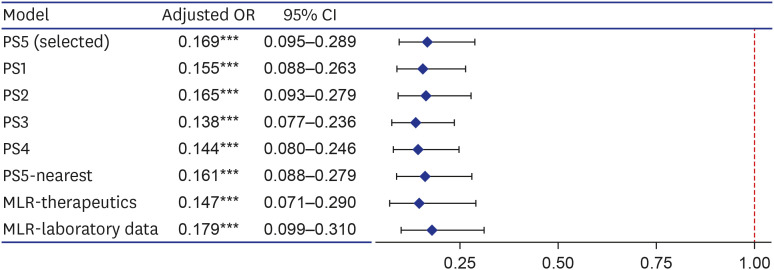
Fig. 2
Forest plot for effects of regdanvimab on composite outcome of death, or disease aggravation in sensitivity analyses. Sensitivity analyses were performed by changing the covariates included in the PS estimation model (PS1–5), changing the matching method (PS5-nearest), and adding covariates in the multivariable logistic regression model of analyzing the matching data (MLR-therapeutics and laboratory data). The covariates included in each PS estimation model are as follows; PS5 included variables corresponding to the regdanvimab administration criteria of European Medicines Agency and gender according to clinical judgment (age, sex, BMI, cardiovascular disease, chronic lung disease, diabetes mellitus, hypertension, chronic kidney disease, chronic liver diseases, and pneumonia); PS1 included all measured covariates (age, sex, BMI, cardiovascular disease, chronic lung disease, diabetes mellitus, hypertension, chronic kidney disease, chronic liver diseases, pneumonia, ACEIs/ARBs, statins, aspirin, and immunomodulators); PS2 included variables that were statistically significant for both exposure and outcome, and significant for outcome (age, cardiovascular disease, hypertension, chronic kidney disease, and pneumonia); For PS3, variables corresponding to the Korean regdanvimab administration criteria were included according to clinical judgment (age, cardiovascular disease, chronic lung disease, diabetes mellitus, hypertension, and pneumonia); PS4 included variables of PS3 and what significant for outcome (age, cardiovascular disease, chronic lung disease, diabetes mellitus, hypertension, chronic kidney disease, and pneumonia). PS5-nearest was the result of performing nearest matching by designating a caliper, which was 0.094 (0.2 of the standard deviation of the logit of the PS). MLR-therapeutics was the result of adding other treatment exposures (azithromycin, corticosteroids, hydroxychloroquine, lopinavir/ritonavir, and remdesivir), and MLR-laboratory data was that of adding the baseline laboratory data (C-reactive protein, lactate dehydrogenase, D-dimer, troponin I, ferritin, and creatine kinase).
OR = odds ratio, CI = confidence interval, PS = propensity score, MLR = multivariable logistic regression, BMI = body mass index, ACEI = angiotensin-converting enzyme inhibitor, ARB = angiotensin-receptor blocker.
Variables of significance (***P < 0.001).
![]()
DISCUSSION
This retrospective analysis evaluated the effects and safety of regdanvimab in a PS-matched cohort of patients with mild-to-moderate COVID-19. Regdanvimab reduced disease aggravation by ≤ 77% in the PS-matched cohort compared with conventional treatment (RRR, 76.5%; P < 0.001), without increasing adverse outcomes, and this effect was also evident in the result of multivariate model considering other influencing factors (OR, 0.169; 95% CI, 0.095, 0.289; P < 0.001). The results were consistent across analytical or matching methods, and disease aggravation in the overall cohort was consistently reduced. In terms of mortality, none of the patients died in the PS-matched cohort, but in the overall cohort, 17 (3.3%) of 520 without regdanvimab treatment died compared with none in the regdanvimab group (Supplementary Table 3).
The results from part one of a phase 2/3 randomized clinical trial of patients with mild-to-moderate COVID-19 found that regdanvimab 40 mg/kg reduced the need for hospitalization or oxygen therapy by > 50% compared with placebo a (4.0% vs. 8.7%). It was more effective in patients with moderate COVID-19 (6.5% vs. 15.8%) and even more effective in moderate COVID-19 aged ≥ 50 years (7.5% vs. 23.7%).18 Although the results of the phase 3 clinical trial of regdanvimab have not yet been published, press releases state that it reduces the incidence of hospitalization or death by 72% among high-risk patients and by 70% in all patients.3536 Here, we presumed that the regdanvimab effect on preventing the disease aggravation was somewhat greater because we targeted patients with high-risk mild or moderate COVID-19 who were indicated for regdanvimab.
The present results are comparable to those of other studies of neutralizing mAbs. Although some administration protocols differed, the results of the phase 3 BLAZE-1 study showed that bamlanivimab 700 mg and etesevimab 1,400 mg reduced COVID-19 related hospitalization or death by 87% compared with a placebo (0.8% vs. 6%, P < 0.001).3738 Moreover, four patients given a placebo died, whereas no-one given bamlanivimab and etesevimab died (P = 0.010).3738 The number of medically attended visits was reduced by 49% by neutralizing antibody mixture comprising 1,200 mg each of casirivimab and imdevimab compared with a placebo in all study subjects,39 and by 67% in a post-hoc analysis of high-risk patients.4041 Sotrovimab, a single agent neutralizing mAb, was approved for EUA by FDA in May 2021.42 According to the unpublished interim results from phase 1/2/3 COMET-ICE study, a single dose of 500 mg of sotrovimab reduced the rate of hospitalization or death by day 29 by about 79% compared with a placebo in adult patients with mild or moderate COVID-19 with risk factors.43 In Korea, until recently, all confirmed COVID-19 patients were hospitalized regardless of severity. Therefore, in this study, death or disease aggravation was defined as a composite primary outcome instead of hospitalization or death as used in other studies. In other studies, hospitalization was defined as a case of hospitalization for more than 24 hours due to acute treatment or requiring oxygen therapy or mechanical ventilation, so it could be considered as similar outcome.
Fewer adverse reactions occurred in the group with, than without regdanvimab, which is presumably because more alternative therapeutic agents were administered to the latter group. Moreover, although not included in this paper, in the sensitivity analysis results that included alternative therapeutics administered before severe transition as covariates in the multivariate model, none of these (azithromycin, corticosteroids, lopinavir/ritonavir) had a significant effect on the composite outcome of death, or disease aggravation. None of the alternative therapeutics have been proven to be effective in treating mild-to-moderate COVID-19, but in the absence of established therapeutics, it may have been an unavoidable choice for treating patients. However, it should be noted that the use of these drugs increases the side effects without increasing the effectiveness.
This study has some limitations. We reduced bias in the observational studies using PS-matched and multivariable logistic regression analyses, but the possibility that unmeasured confounding factors might remain cannot be ruled out. Other factors that might affect outcomes, such as insurance type and income level, were not included. The entire cost of COVID-19 treatment is covered by the Korean government, so insurance type or income level was not considered as an influencing factor in the present study. However, these should be considered an important factor in other countries. Vaccination was not included in the investigation because no breakthrough infection occurred after vaccination among our study participants. In addition, since only a few mutant virus infections were confirmed, this study did not consider them as influencing factors and did not include them. However, breakthrough infection is also likely to increase as rates of vaccination and mutant virus infection increase, so these might also become important factors affecting treatment outcomes. The secondary outcomes were somewhat ambiguous. In terms of hospitalization, since BMC manages non-critical COVID-19 patients and some patients suffering from deterioration involve in transfer to a tertiary hospital rather than stay, the length of the hospital stay in BMC might partly reflect deterioration of the patient’s clinical status. In addition, discharge was delayed for some patients due to reasons unrelated to the progress of COVID-19, such as those who were guardians of pediatric patients or had unrelated comorbidities. Therefore, the length of the hospital stay might be difficult to equate with the clinical status of patients. Unlike other countries, patients diagnosed with COVID-19 have been mostly hospitalized regardless of severity in Korea. Therefore, the meaning of hospitalization or length of the hospital stay may differ from that in other countries. The adverse reactions of fever or systemic pain, injection site inflammation, hypersensitivity, and gastrointestinal toxicity were retrospectively identified based on EMRs; thus, minor symptoms might have been omitted or not closely followed up. Other adverse events identified based on laboratory data only included those during hospitalization, and not for longer periods.
Despite these limitations, the present findings have several important implications. Regdanvimab is the only neutralizing mAb against SARS-CoV-2 available in Korea, and it has shown significant clinical effectiveness as a single agent. However, the results of the phase 3 clinical trials await publication, and sufficient evidence for its routine clinical application is lacking. We hope that the real-world evidence provided herein, along with the results of the phase 3 clinical trials, will serve as a basis for effectively treating COVID-19. Controlling the transition to severe disease will prevent the collapse of medical systems in a pandemic situation where large number of patients are affected, and will also have important economic implications. The use of therapeutics cannot be overlooked, as COVID-19 continues to thrive despite vaccination.
Studies on the therapeutic effects of neutralizing antibodies, including regdanvimab, on mutated variants are currently in progress.444546 Further studies of the regdanvimab effectiveness in actual clinical practice are needed on breakthrough or mutant virus infection.
In conclusion, regdanvimab was significantly associated with lower odds of disease aggravation in 754 PS-matched patients at a 1:1 ratio who were administered with regdanvimab or not (n = 377 each; OR, 0.169; 95% CI, 0.095, 0.289; P < 0.001) without increasing adverse reactions.
 XML Download
XML Download